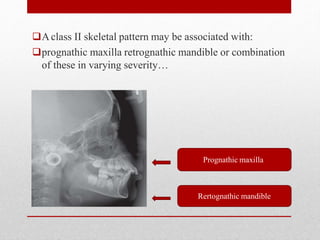
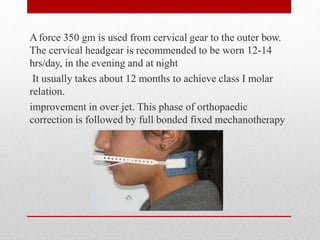
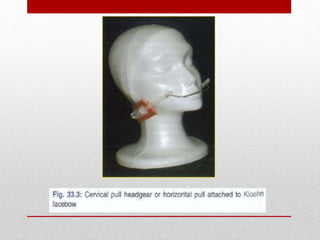
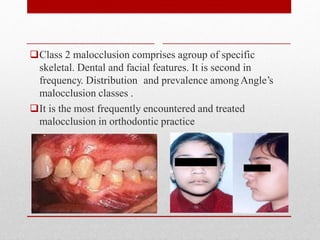
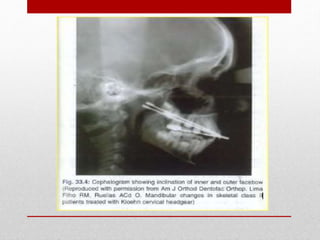
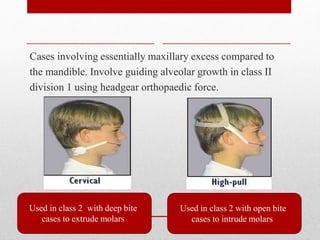
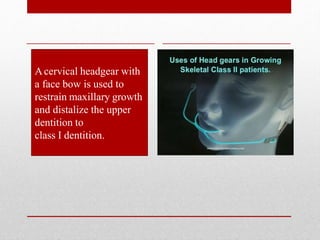
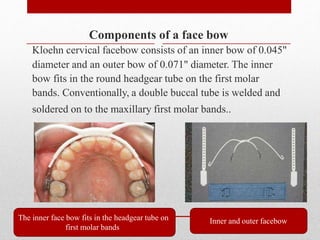
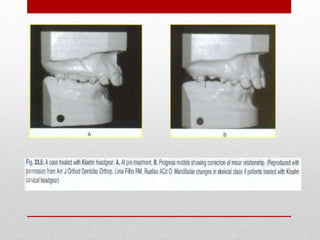
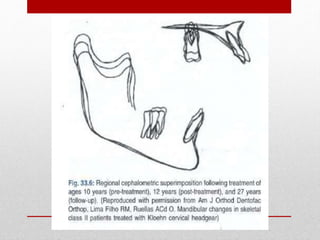
Class II malocclusion is characterized by a protrusive maxilla and/or retrusive mandible. Early intervention during the mixed dentition stage utilizes cervical headgear to guide maxillary growth. A Kloehn facebow applies distalizing forces to the maxillary molars, inhibiting forward growth of the maxilla while allowing normal mandibular growth. This redirects occlusion to a Class I relationship and improves the patient's skeletal and dental profile.