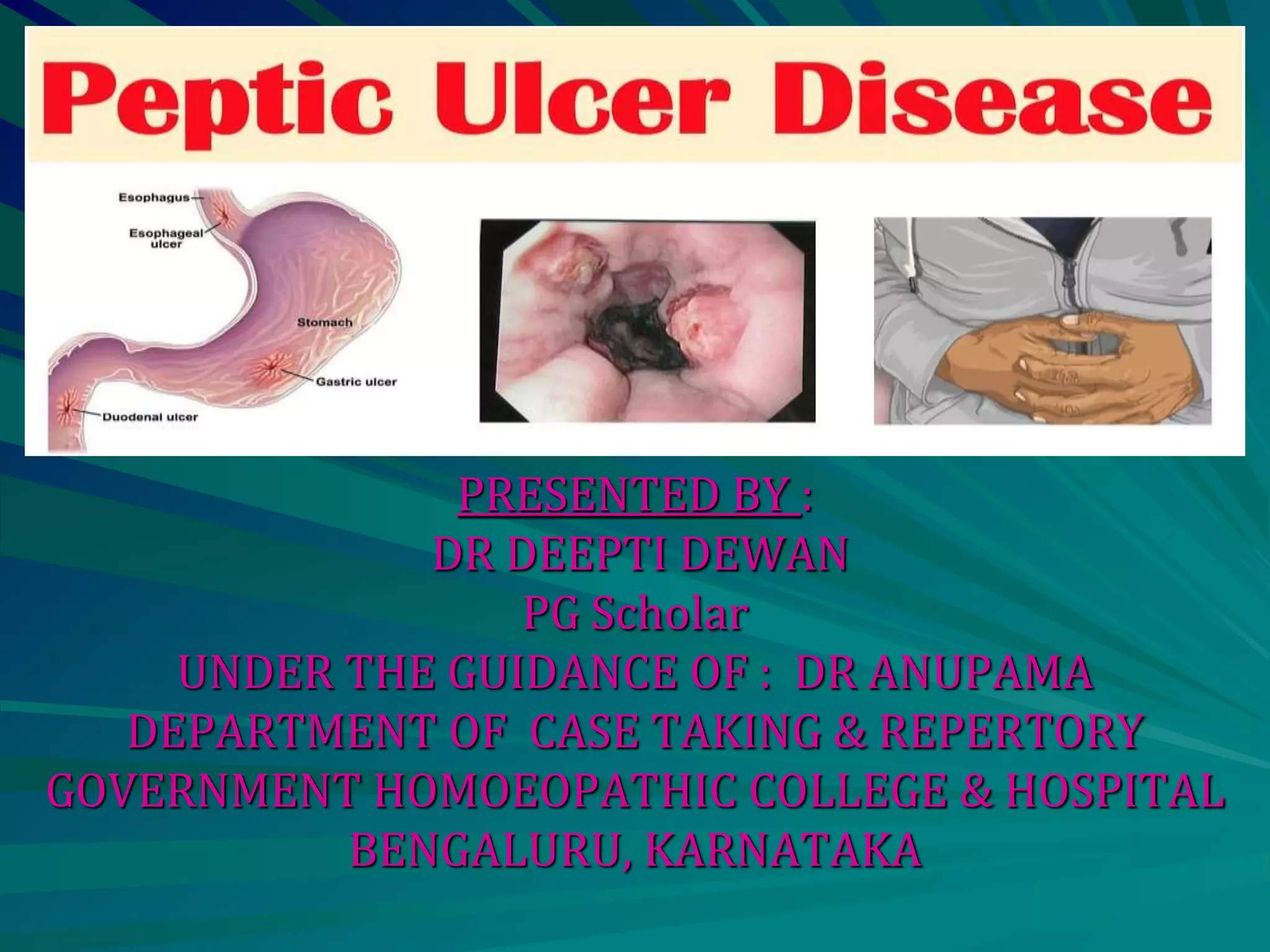
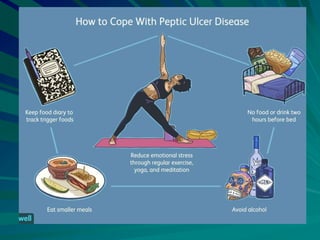
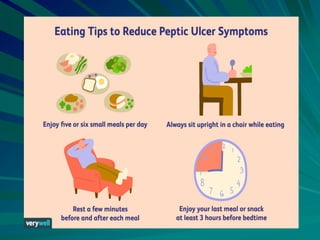
This document discusses acid peptic disease (APD) including peptic ulcers, gastric ulcers, and duodenal ulcers. It covers the incidence, common etiologies like H. pylori infection and NSAID use, typical clinical presentations of pain relieved by food or alkalis, and important investigations like endoscopy. Differential diagnoses and treatments including lifestyle changes, medications, and potential complications of hemorrhage, perforation, and obstruction are summarized. Homeopathic management using acute medicines and constitutional remedies is also mentioned.