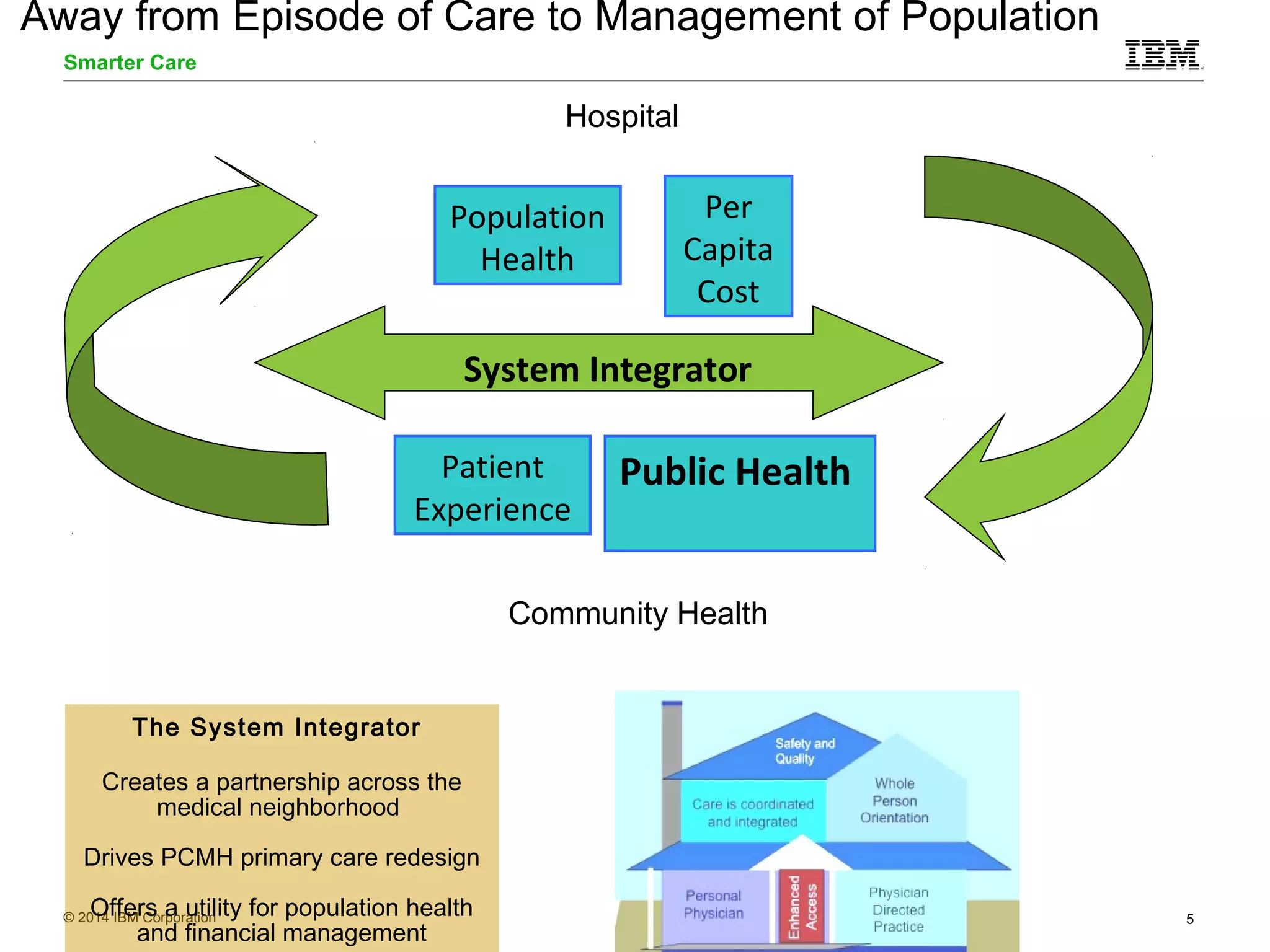
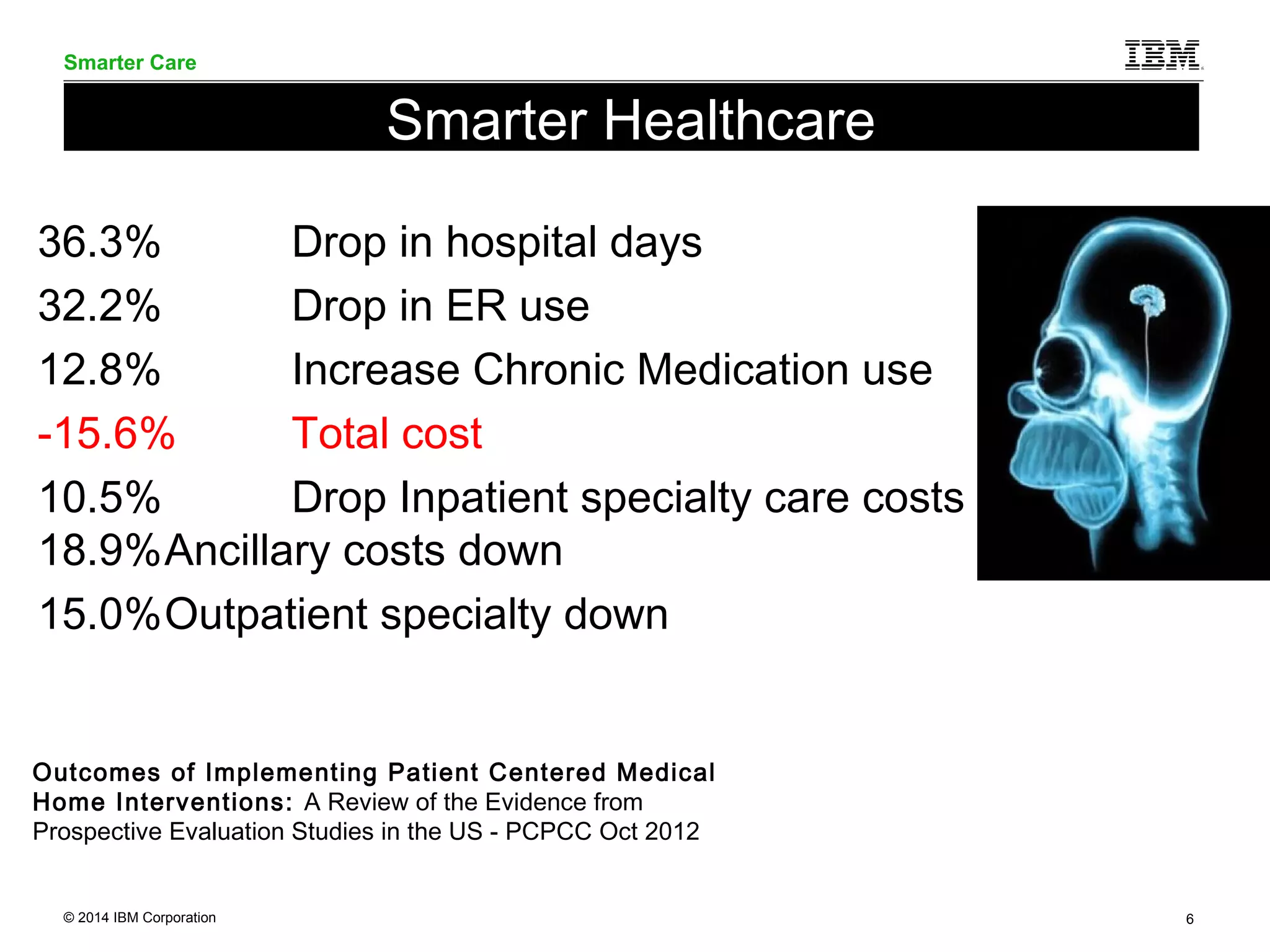

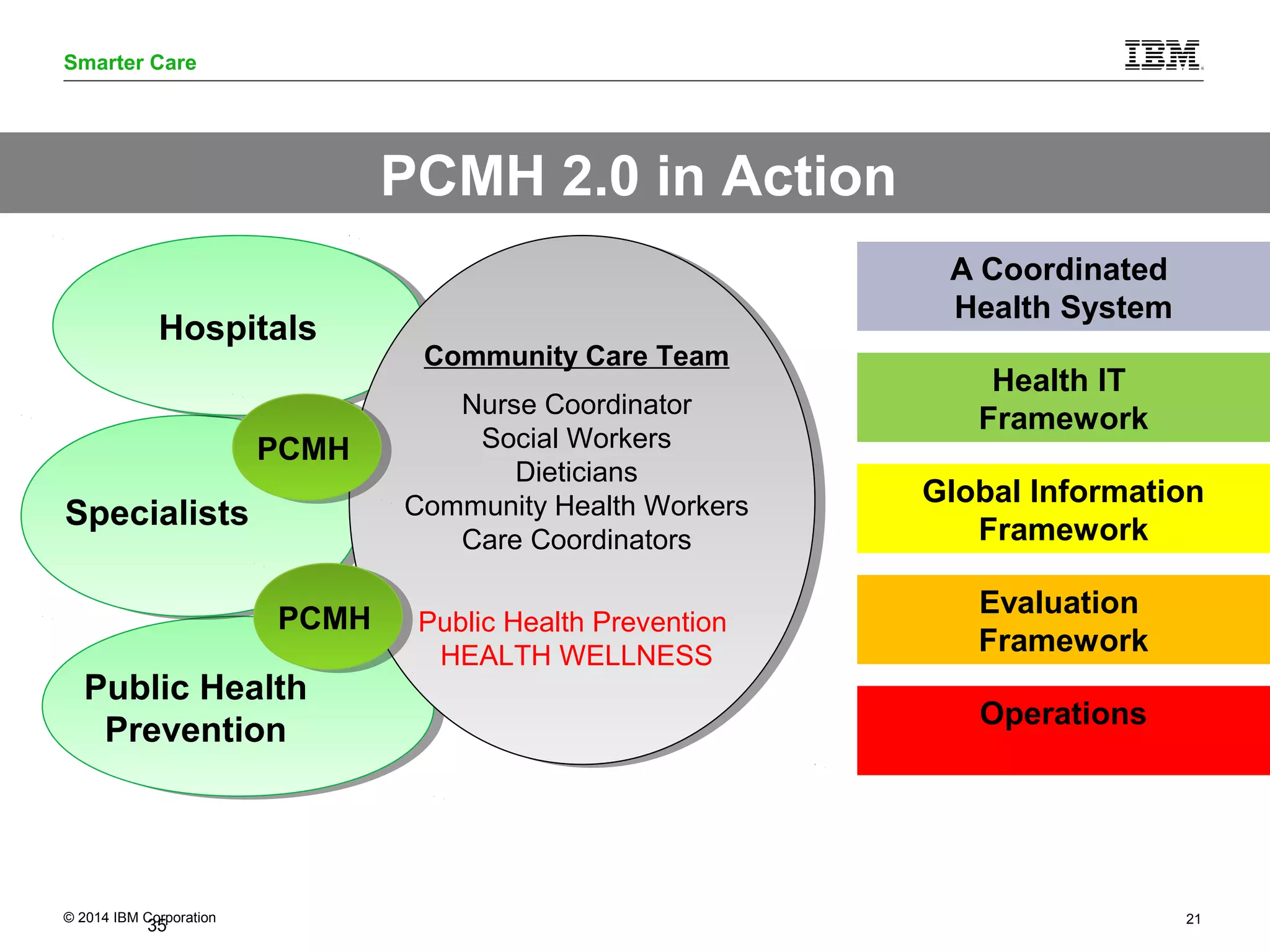
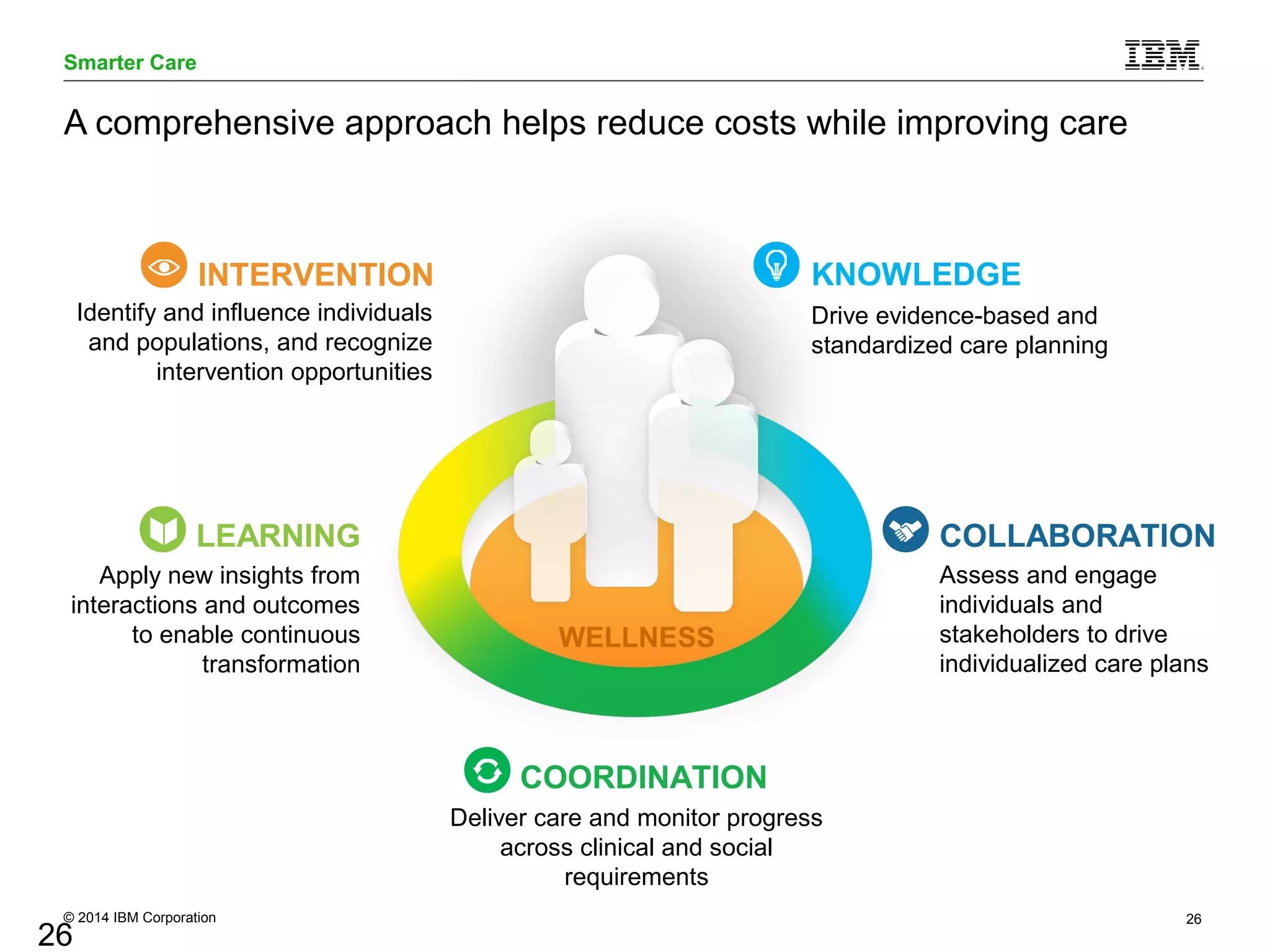


The document outlines the objectives and evidence supporting the Patient-Centered Medical Home (PCMH) model, highlighting its effectiveness in reducing healthcare costs and improving patient care across several states. It details various case studies demonstrating significant reductions in hospitalization and overall healthcare expenditures due to PCMH implementations. Additionally, it emphasizes the importance of care coordination, technology integration, and patient engagement in achieving better health outcomes.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




