2
Preliminary questions tothe group
• What is your experience in outbreak
investigations?
• If yes, what difficulties did you face?
• What would you like to learn about outbreak
investigations?
3.
3
Outline of thesession
1. Outbreaks and epidemics
2. Outbreak detection
3. Outbreak investigation
4. Managerial aspects of outbreak
investigations
4.
4
Endemic versus epidemic
•Endemicity
Disease occurring in a population regularly at a
usual level
• Tuberculosis, Malaria
• Epidemics
Unusual occurrence of the disease in excess of its
normal expectation
• In a geographical location
• At a given point of time
e.g. Hepatitis E, measles, cholera
Outbreaks
5.
5
Outbreaks versus epidemics
•Occurrence of cases of an illness in excess of
expected numbers
• Scale
Outbreak
• Limited to a small area, within one district or few blocks
Epidemic
• Covers larger geographic areas
• Linked to control measures in district/state
No exact precise threshold: Use a word or the other
according to whether you want to generate or deflect
attention
• Be aware of legal implications of the use of the term
“Epidemic” in India (Epidemic disease act, being revised)
Outbreaks
6.
6
Sources of information
todetect outbreaks
• Event-based surveillance
Rumour register
• To be kept in standardized format in each institution
• Rumours need to be investigated
Community informants
• Private and public sector
Media
• Important source of information, not to neglect
• Case-based surveillance
Review of routine surveillance data and triggers
Detection
7.
7
Early warning signalsfor an outbreak
• Clustering of cases or deaths
• Increases in cases or deaths
• Single case of disease of epidemic potential
• Acute febrile illness of an unknown etiology
• Two or more linked cases of disease with outbreak
potential
(e.g., Measles, Cholera, Dengue, Japanese encephalitis or plague)
• Unusual isolate (Cholera O 139)
• Shifting in age distribution of cases (Cholera O 139)
• High vector density
• Natural disasters
Detection
8.
8
Importance of timelyaction: The first
information report (Form C)
• Filled by the reporting unit
• Submitted to the District Surveillance Officer
as soon as the suspected outbreak is verified
• Sent by the fastest route of information
available
Telephone
Fax
E-mail
Detection
9.
9
The rapid responseteam
• Composition
Epidemiologist, clinician and microbiologist
• Entomologist when vector-borne disease
Gathered on ad hoc basis when needed
• Role
Confirm and investigate outbreaks
• Responsibility
Assist in the investigation and response
Primary responsibility rests with local health staff
Detection
10.
10
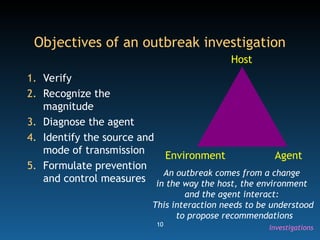
Objectives of anoutbreak investigation
1. Verify
2. Recognize the
magnitude
3. Diagnose the agent
4. Identify the source and
mode of transmission
5. Formulate prevention
and control measures
Host
Environment Agent
An outbreak comes from a change
in the way the host, the environment
and the agent interact:
This interaction needs to be understood
to propose recommendations
Investigations
11.
11
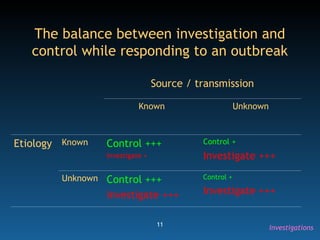
The balance betweeninvestigation and
control while responding to an outbreak
Source / transmission
Known Unknown
Etiology Known Control +++
Investigate +
Control +
Investigate +++
Unknown Control +++
Investigate +++
Control +
Investigate +++
Investigations
12.
12
Steps in outbreakresponse
1. Verifying the outbreak
2. Sending the rapid response team
3. Monitoring the situation
4. Declaring the outbreak over
5. Reviewing the final report
Investigations
13.
13
Step 1: Verifyingthe outbreak
• Validate the source of information
? Change in the reporting system
? Change in the population size
? Acute reporting of old, chronic cases
• Check with the concerned medical officer:
? Abnormal increase in the number of cases
? Clustering of cases
? Epidemiological link between cases
? Triggering event
? Deaths
Investigations
14.
14
Step 2: Sendingthe rapid response team
• Review if the source and mode of transmission are
known
• If not, constitute team with:
Medical officer
Epidemiologist
Laboratory specialist
• Formulation of hypothesis on basis of the description
by time, place and person (Descriptive epidemiology)
? Does the hypothesis fits the fact
YES: Propose control measures
NO: Conduct analytical studies
Investigations
15.
15
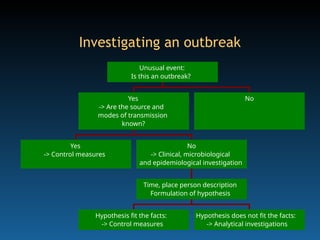
Yes
-> Control measures
Hypothesisfit the facts:
-> Control measures
Hypothesis does not fit the facts:
-> Analytical investigations
Time, place person description
Formulation of hypothesis
No
-> Clinical, microbiological
and epidemiological investigation
Yes
-> Are the source and
modes of transmission
known?
No
Unusual event:
Is this an outbreak?
Investigating an outbreak
16.
16
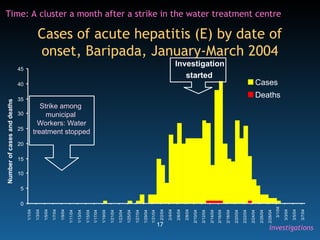
Example: Outbreak ofacute hepatitis (E)
in Baripada, Orissa, 2003
• Identification of a cluster of acute hepatitis
cases
• Diagnosis: HEV infection
• Use time, place and person analysis of
surveillance data to suggests hypotheses
18
Chip
at
rive
r
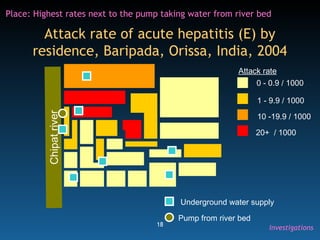
Attack rate ofacute hepatitis (E) by
residence, Baripada, Orissa, India, 2004
0 - 0.9 / 1000
1 - 9.9 / 1000
10 -19.9 / 1000
20+ / 1000
Attack rate
Underground water supply
Pump from river bed
Place: Highest rates next to the pump taking water from river bed
Investigations
19.
19
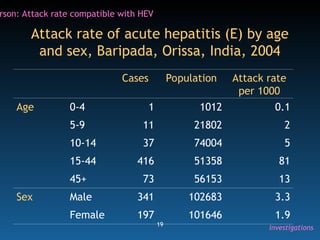
Attack rate ofacute hepatitis (E) by age
and sex, Baripada, Orissa, India, 2004
Cases Population Attack rate
per 1000
Age 0-4 1 1012 0.1
5-9 11 21802 2
10-14 37 74004 5
15-44 416 51358 81
45+ 73 56153 13
Sex Male 341 102683 3.3
Female 197 101646 1.9
rson: Attack rate compatible with HEV
Investigations
20.
20
What hypotheses wouldyou generate for
the outbreak of acute hepatitis (E)
in Baripada, Orissa, 2003?
• Time:
It happens a month after a strike in the water
treatment plant
• Place:
It is clustered around a water source that takes
water from the river
• Person:
Adults are mostly affected
The river water may have been supplied untreated in the area of the
outbreak because of the strike at the water treatment plant
21.
21
Descriptive versus analytical
investigations
•Descriptive investigations
Based upon cases only
Look at time, place and person epidemiology
Raise hypotheses
• Analytical investigations
Based upon a study of the cases and non-cases
Compare:
• Cases with controls with respect to exposure
• Exposed with unexposed with respect to incidence
Test hypotheses
• How could we test the hypothesis for the Baripada
investigation?
Investigations
22.
22
Steps of afull outbreak investigation
using analytical epidemiology to identify
the source of infection
1. Determine the existence of an outbreak
2. Confirm the diagnosis
3. Define a case
4. Search for cases
5. Generate hypotheses using descriptive findings
6. Test hypotheses based upon an analytical study
7. Draw conclusions
8. Compare the hypothesis with established facts
9. Communicate findings
10. Execute prevention measures
Requires assistance from qualified
field epidemiologist (FETP)
23.
23
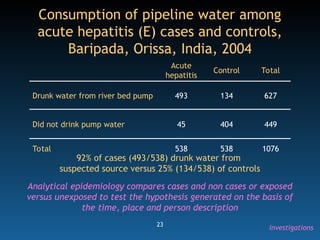
Acute
hepatitis
Control Total
Drunk waterfrom river bed pump 493 134 627
Did not drink pump water 45 404 449
Total 538 538 1076
92% of cases (493/538) drunk water from
suspected source versus 25% (134/538) of controls
Consumption of pipeline water among
acute hepatitis (E) cases and controls,
Baripada, Orissa, India, 2004
Analytical epidemiology compares cases and non cases or exposed
versus unexposed to test the hypothesis generated on the basis of
the time, place and person description
Investigations
24.
24
3. Monitoring thesituation
• Trends in cases and deaths
• Implementation of containment measures
• Stocks of vaccines and drugs
• Logistics
Communication
Vehicles
• Community involvement
• Media response
Investigations
25.
25
4. Declaring theoutbreak over
• Role of the district surveillance officer /
Medical health officer
• Criteria
No new case during two incubation periods since
onset of last case
• Implies careful case search to make sure no
case are missed
Investigations
26.
26
5. Review ofthe final report
• Sent by medical officer of the primary health
centre to the district surveillance officer /
medical and health officer within 10 days of
the outbreak being declared over
• Review by the technical committee
Identification of system failures
Longer term recommendations
Investigations
27.
27
Outbreak preparedness:
A summaryof preparatory action
• Formation of rapid response team
• Training of the rapid response team
• Regular review of the data
• Identification of ‘outbreak seasons’
• Identification of ‘outbreak regions’
• Provision of necessary drugs and materials
• Identification and strengthening appropriate laboratories
• Designation of vehicles for outbreak investigation
• Establishment of communication channels in working
conditions (e.g., Telephone)
Management
28.
28
Managerial aspects ofoutbreak response
• Logistics
Human resources
Medicines
Equipment and supplies
Vehicle and mobility
Communication channels
• Information, education and communication
• Media
Daily update
Management
29.
29
Control measures foran outbreak
• General measures
Till source and route of transmission identified
• Specific measures, based upon the results of the
investigation
Agent
• Removing the source
Environment
• Interrupting transmission
Host
• Protection (e.g., immunization)
• Case management
Management
30.
30
Take home messages
1.Do not ignore or hide outbreaks
2. Respond to early warning signals
3. Investigate outbreaks to:
Control the current outbreak
Learn about the disease in the local setting
4. Outbreaks require an organized, well
managed response
31.
31
Additional reading
• CDCtext book on principles of epidemiology
• Section 5 of operations manual
• Module 8 of training manual
Detection
Editor's Notes
#2 The usual warming up questions for a few minutes.
#4 The difference between endemic and epidemic.
Self explanatory.
#5 The difference between outbreak and epidemic.
The take home message is: There is no formal difference. You are the one who decide how much importance you want to give to the event.
If you are having lots of measles and none wants to help, call it a major epidemic.
If it is a cluster well under controlled that the press is blowing out of proportion, call it a small outbreak.
#6 This slide is a booster dose for the lecture on alert.
#7 The early warning signals for an outbreak.
Provide additional examples.
#8 The First Information Report is a quick document, a sort of post card from the field that says: This is the alert, we are on our way, we will investigate and we will bring more information.
#10 An outbreak comes from a break in the balance between the host, the environment and the agent.
We need to understand this breach of balance to propose effective control measures.
Hence the objectives of the investigations.
#11 This is an important slide.
There is a balance between investigation and control measures in outbreak response.
Underline the 2 x 2 table matrix that is the way we think in epidemiology ;-)
#12 The steps in outbreak response.
Response is a broader term that covers (1) investigations and (2) control measures.
#13 The step 1 of the outbreak investigation.
We need to verify not to fall in the trap of pseudo outbreaks.
#14 Step 2.
The rapid response team is the strong arm of outbreak response. Multi-disciplinary is the key word.
The slide also introduces the key notion of the two levels:
Generating hypotheses on the basis of descriptive information
Testing hypotheses on the basis of analytical methods.
We want people to be proficient at the first and aware of the second.
#15 A flow chart presentation of the same.
If the descriptive epidemiology suggests you are dealing with a very well known classical scenario, you may not need analytical methods.
But if there is something you do not understand, then you do need them.
#16 The following few slides will go through an example of hypothesis generation and testing.
It is an hepatitis E outbreak in Orissa.
#17 This is the TIME information: What does it suggest?
Give a moment to the participants. Encourage them to follow the (1) describe and (2) analyze/ interpret steps.
Probably a point source outbreak. It leads us to look into what happened one month earlier: There was a strike in the municipal water treatment plant.
#18 This is the PLACE information.
Give a moment to the participants. Encourage them to follow the (1) describe and (2) analyze/ interpret steps.
It seems the disease clusters around the one source of water supply that comes directly from the river.
#19 This is the PERSON information.
Give a moment to the participants. Encourage them to follow the (1) describe and (2) analyze/ interpret steps.
The attack rate by age and sex is highly compatible with HEV.
#20 Here we summarize the time, place and person information to “connect the dots” and come with a picture that generates an hypothesis:
The hypothesis reads as:
The river water may have been supplied untreated in the area of the outbreak because of the strike at the water treatment plant
#21 Again we emphasize the difference between the two levels:
Descriptive / hypothesis raising
Analytical / hypothesis testing
We want them to be proficient at the first and aware of the second.
Brainstorm with the participants how to go about the analytical approach.
#22 If we go for a fully fledged investigation with analytical methods, we will use the classical 10 steps.
But that is beyond the skills we expect from the participants of the course.
We would need help from a 2-year scholars of a Field Epidemiology Training Programme.
#23 If we get back to the Baripada HEV example, this is how the analytical epidemiology was approached with a case control study.
See the language in purple at the bottom: The objective is to remain at a broad, conceptual level.
#24 Back to our steps in the investigations. Now step 3: Monitoring the situation.
#27 But we do not wait for an outbreak to happen.
We want to be prepared.
Here is a list of the actions to undertake to be ready.
#28 So far we have gone through the logical, methodological , intellectual aspects of outbreak investigations.
But there is a managerial aspect also.
#29 The control measures to undertake.
They should be based on the results of the investigations.
If the outbreak says it was the food handler of the village there is no point in chlorinating the well!