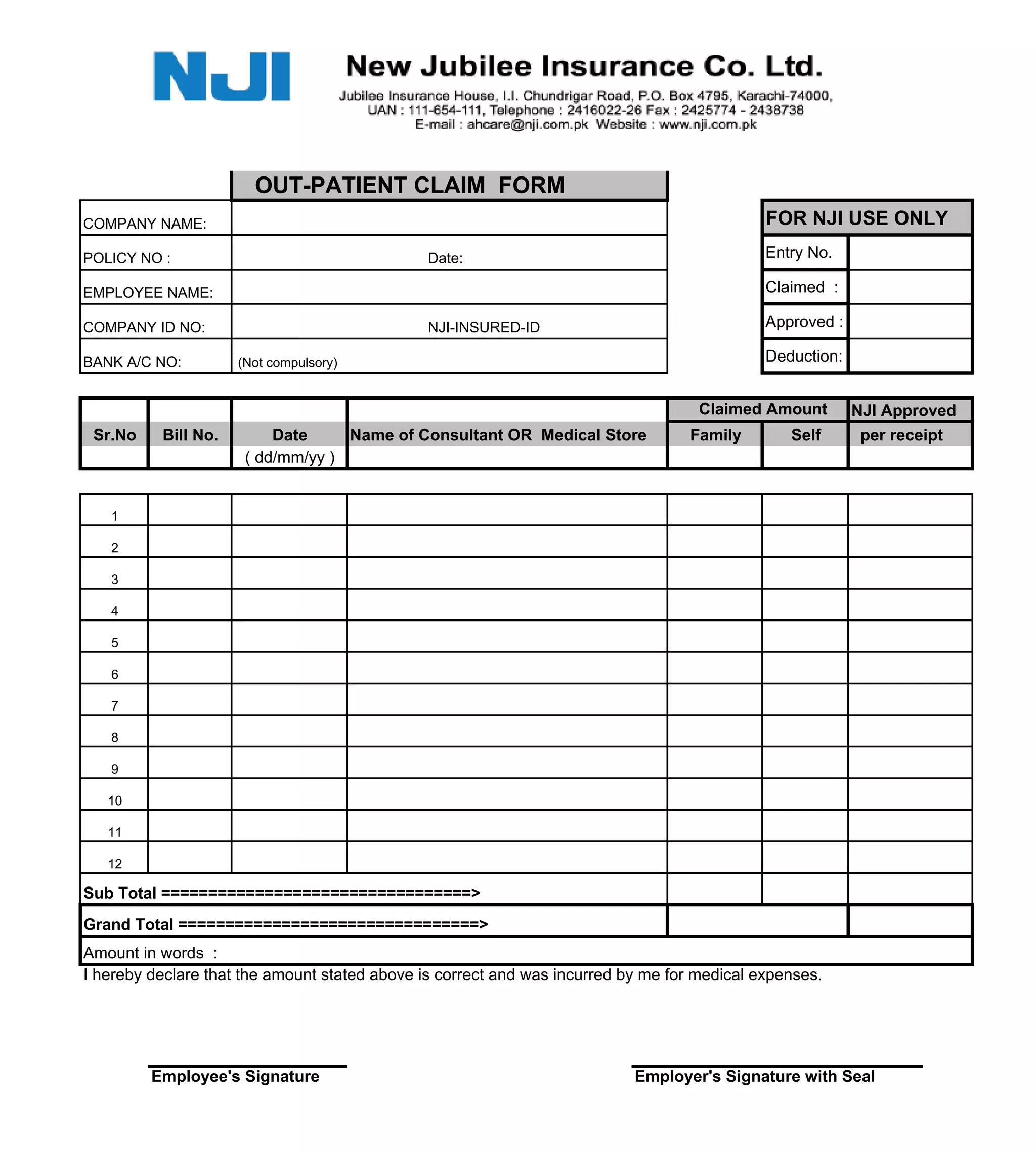
This document is an out-patient claim form for reimbursement of medical expenses from a company's insurance provider. It requests information such as the employee and policy details, bills and receipts for medical expenses, and signatures from the employee and employer certifying the accuracy of the claimed expenses. Supporting documents like diagnosis reports and prescriptions must also be attached for approval and reimbursement of the expenses.