Learning Objectives
At theend of the presentation, students should be able to;
• Define nutritional assessment and explain its importance
• Identify the different methods
• Conduct and interpret anthropometric measurements
• Conduct simple clinical and dietary assessments
• Establish the need for nutrition intervention, plan and follow up
actions
• Identify the patients/clients at nutrition risk requiring nutrition
intervention 4
5.
Healthy diet enhancesgrowth and
health throughout life, meets
special needs of pregnancy &
lactation, & recuperation
Malnutrition results imbalance of
nutrients and energy in the diet
Micronutrient deficiencies,
underweight, overweight, obesity,
low birth weight, wasting, stunting,
etc.
5
Introduction
6.
Introduction Cont...
● Nutritionalassessment is the interpretation of
anthropometric, biochemical, clinical and dietary data
to determine whether a person or groups of people
are well nourished or malnourished [1]
6
7.
Introduction Cont...
● Nutritionalassessment is important for
identifying people at risk of malnutrition,
informing nutrition education and counseling,
establishing appropriate nutrition care plans,
and evaluating the effectiveness of nutrition
interventions. [1]
7
8.
Why Nutritional Assessment
1.Whenever a patient come to a health care setting it is
important to determine the patient nutrition risk because,
it can always be associated with the outcome of patient
hospital stay time.
2.Patient who tend to have poor nutritional status or
malnutrition have a higher rate of morbidity or mortality.
3.It is therefore, to be important of their status and monitor it
through out the period of care
8
9.
Malnutrition Epidemiology
Malnutrition associatedwith increased complications
Poor wound healing
Immunocompromised status
Organ function impairment
Healthcare utilization (resources and cost)
30- 50% prevalence, depending on the criteria and practice setting
studied
Morbidity/Mortality. [9]
9
10.
Case
NR is a25 y/o female who presented at GOPD for routine checkup.
Vitals taken at the beginning of her appointment include; BP 120/70,
HR 80, RR 18, SPO2 98%, RBG 3.4mmol/L, Ht 5.6m, Wt 65kg.
Prior to her appointment, labs were obtained including a serum
albumin of 2.1g/dL (3.5-5.5g/dL) and prealbumin of 10mg/dL (15-
36mg/dL).
NR past medical history is for generalized anxiety disorder and
depression, currently on venlafaxine XR 75mg PO daily.
She reports lack of appetite and a weight loss of 5kg within the last 3
months. 10
11.
Case Question #1
Whattype of malnutrition syndrome does NR most
likely have?
A. Acute disease-associated
B. Chronic disease-associated
C. Starvation-associated
D. None of the above
11
12.
Case Question #2
Whichmay indicate that NR is malnourished?
A. Dietary intake
B. Serum prealbumin level
C. Weight loss history
D. All of the above
12
13.
Case Question #3
IfNR becomes hospitalized, when should nutritional
assessment be performed?
A. Within 24 hours
B. Within 48 hours
C. Within 96 hours
D. Within 1 week
13
14.
NUTRITION ASSESSMENT
• Nutritionalassessment is the process of exploring and
determining the nutritional status of individuals or groups for
the purpose of identifying nutritional needs and planning
personal health care or community programme to meet these
needs
• It is the systematic process of collecting and interpreting
information in order to make decisions about the nature and
cause of nutrition related health issues that affect an individual
14
15.
Screening vs Assessment
NutritionalScreening – process to identify an
individual who is malnourished through the
use of appropriate screening and assessment
methods.
Nutritional assessment – A more comprehensive
evaluation to make a diagnosis of a
malnutrition syndrome and guide intervention
and expected outcomes. 15
16.
Objectives of NutritionalAssessment
● To establish the nutritional status by objective
measurement using appropriate parameters in
relation to specific indication such as assessment of
anemic status
● To develop adequate nutrition nursing care plan for a
client in a multidisciplinary setting.
16
17.
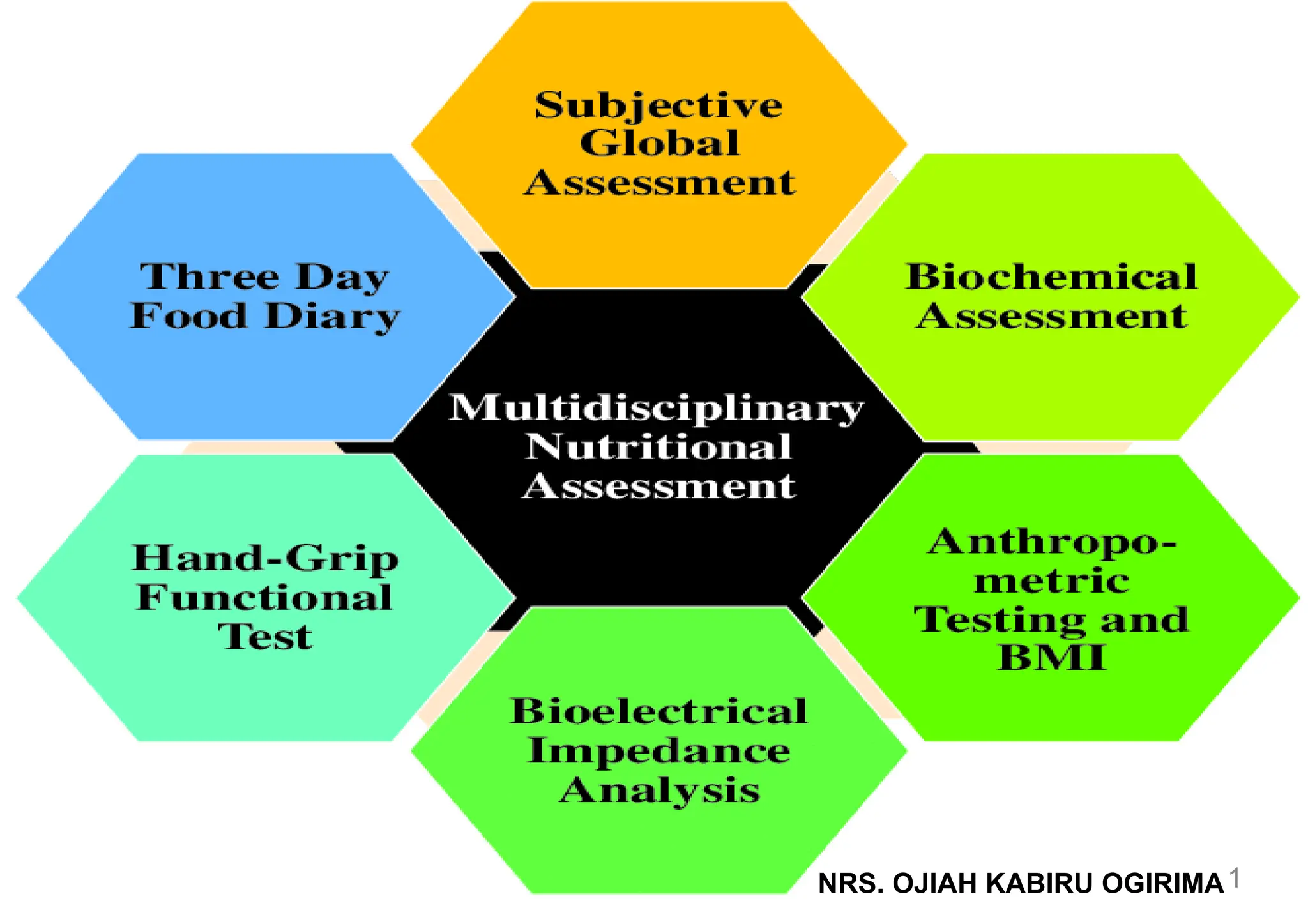
Nutritional assessment components
Nutritionalassessment of patients may include:
History and clinical diagnosis.
Clinical signs and physical examination
The ABCD Methods of Nutritional Assessment
Mini Nutritional Assessment (MNA)
Subjective Global Assessment (SGA)
Malnutrition Universal Screening Tool (MUST)
Nutrition Risk Screening 2002 (NRS 2002)
Functional outcomes
17
18.
History and ClinicalDiagnosis
Elements included are…
Assessment of usual foods, fluids & supplements
Foods avoided due to allergies or preference
Medications and nutritional supplements
Satisfaction with diet
Social and access to adequate diet.
Body weight & height
Eating difficulties/gastrointestinal complaints (i.e. N/V/D/C, problems
swallowing)
Medical and surgical conditions (both acute and chronic)
18
Main Components
● Anthropometricassessment
● Biochemical assessment
● Clinical assessment
● Dietary assessment
The ABCD Methods of Nutritional Assessments
● Note: The ABCD methods of nutritional assessment are
complementary and should be used together to obtain a
comprehensive and accurate evaluation of the nutritional
status of individuals or groups. [4]
20
21.
Anthropometric Assessment
● Itis the measurement of the Physical dimensions of bones,
muscles and adipose tissues compared with population
standards or used to monitor changes in an individual over
time.
● Anthropometry can help identify under-nutrition (low weight-
for-height, low height-for-age, and low weight-for-age) and
overnutrition (overweight, obesity, and related diseases)
21
22.
Components of AnthropometricAssessment
● Height: This is the vertical distance from the top of the head
to the floor when standing upright. It can indicate the growth
and development of individuals or populations.
● Weight: This is the force of gravity on the body mass. It
reflect the intake, utilization, and excretion of nutrients in the
body.
● Body circumferences: These are the measurements of the
girth of different parts of the body, such as the head, waist,
hip, and limbs.
Body circumferences can indicate the distribution of fat and
muscle tissue in the body.
22
23.
Components of AnthropometricAssessment Cont.
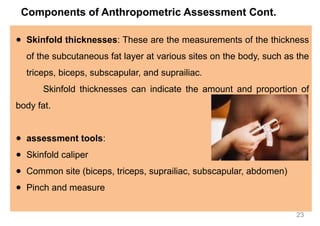
● Skinfold thicknesses: These are the measurements of the thickness
of the subcutaneous fat layer at various sites on the body, such as the
triceps, biceps, subscapular, and suprailiac.
Skinfold thicknesses can indicate the amount and proportion of
body fat.
● assessment tools:
● Skinfold caliper
● Common site (biceps, triceps, suprailiac, subscapular, abdomen)
● Pinch and measure
23
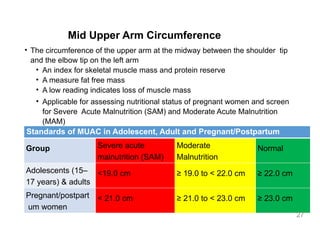
Mid Upper ArmCircumference
• The circumference of the upper arm at the midway between the shoulder tip
and the elbow tip on the left arm
• An index for skeletal muscle mass and protein reserve
• A measure fat free mass
• A low reading indicates loss of muscle mass
• Applicable for assessing nutritional status of pregnant women and screen
for Severe Acute Malnutrition (SAM) and Moderate Acute Malnutrition
(MAM)
Standards of MUAC in Adolescent, Adult and Pregnant/Postpartum
Group Severe acute
malnutrition (SAM)
Moderate
Malnutrition
Normal
Adolescents (15–
17 years) & adults
<19.0 cm ≥ 19.0 to < 22.0 cm ≥ 22.0 cm
Pregnant/postpart
um women
< 21.0 cm ≥ 21.0 to < 23.0 cm ≥ 23.0 cm
27
Body Mass Index(BMI)
• This is the calculation of body weight (Kg) in relation to
height (m2
) and a medical standard for assessing the
degree of body fatness
• A proxy to measure thinness, overweight and obesity in
adults and non pregnant population
• Weight is assessed using weighing scale
• Height is assessed using a stadiometer
30
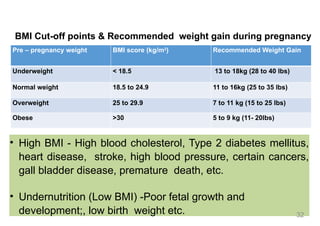
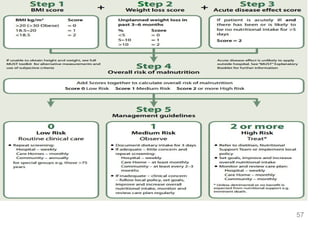
BMI Cut-off points& Recommended weight gain during pregnancy
Pre – pregnancy weight BMI score (kg/m2
) Recommended Weight Gain
Underweight < 18.5 13 to 18kg (28 to 40 lbs)
Normal weight 18.5 to 24.9 11 to 16kg (25 to 35 lbs)
Overweight 25 to 29.9 7 to 11 kg (15 to 25 lbs)
Obese >30 5 to 9 kg (11- 20lbs)
• High BMI - High blood cholesterol, Type 2 diabetes mellitus,
heart disease, stroke, high blood pressure, certain cancers,
gall bladder disease, premature death, etc.
• Undernutrition (Low BMI) -Poor fetal growth and
development;, low birth weight etc. 32
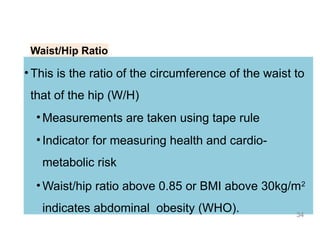
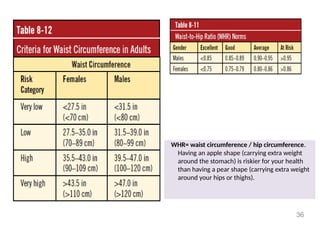
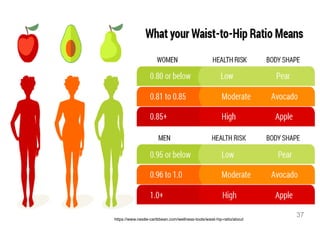
Waist/Hip Ratio
• Thisis the ratio of the circumference of the waist to
that of the hip (W/H)
• Measurements are taken using tape rule
• Indicator for measuring health and cardio-
metabolic risk
• Waist/hip ratio above 0.85 or BMI above 30kg/m2
indicates abdominal obesity (WHO). 34
WHR= waist circumference/ hip circumference.
Having an apple shape (carrying extra weight
around the stomach) is riskier for your health
than having a pear shape (carrying extra weight
around your hips or thighs).
36
Biochemical Assessment
● Biochemicalindices are a set of laboratory assessment used to
determine nutritional status of individual as influenced by intake and
utilization of nutrient.
● This method involves measuring the levels of nutrients or their
metabolites in the blood, urine, feces, or other tissues that have a
relationship with the nutrient
● Biochemical indices are used to detect the serum levels of Albumin, Pre-
albumin, transferin, Vitamins C, D, Zinc, amino acid etc.
● Biochemical tests can help diagnose nutrient deficiencies or excesses,
such as anemia, diabetes, or hyperlipidemia 38
39.
Biochemical Assessment Cont...
Serumferritin (100mcg/L) - iron level - Iron deficiency anaemia
Serum Transferrin Receptor marker (Men: 2-5 mg/L. Women:
1.9-4.4 mg/L) - Iron status - early & late pregnancy
Serum Vitamin D (100 to 150 nmol/L (40 to 60 ng/mL)) - Bone
mineral density, cell repair.
Serum level of omega 3 (the desired HDL) - Functional
efficiency of the heart is compromised. Etc.
39
40.
Biochemical indices
Fluids
Intake 2-3liters per day
Average output: 1700-3000 mL/day
Protein levels
Serum prealbumin:
• Normal – 15-36 mg/dL
• Used to measure the effectiveness of TPN
• Shorter half life than albumin
Serum albumin
• Normal = 3.5 – 5g/dL
• Serum ferritin - iron level - Iron deficiency anaemia
*May be unreliable in face of inflammation 40
41.
Biochemical Indices…..
C-reactive protein(CRP elevated may indicate inflammation, normal
makes albumin reliable)
White blood cell count (above 12,000 indicate inflammation)
Serum glucose (above 180-200g/dL)
Nitrogen balance (NB), or nitrogen equilibrium, occurs when nitrogen
intake equals nitrogen output (NB = 0).
A positive NB or anabolic state exists when nitrogen intake exceeds
nitrogen output.
A net 24-hour positive NB of 2 to 4 g is optimal for anabolism
41
42.
Clinical Assessment
● Involvesphysical examination from head through the hair,
eyes, tongue, lips, neck, upper arm, palms, chest, abdomen,
thighs, legs and feet.
● Physical signs and symptoms of malnutrition can be valuable
in detecting nutritional deficiencies, delayed growth and
development, Pallor of the skin, mucus membranes of the
mouth and eyes, nail bed or palm surfaces, Hair colour, body
appearances, oedema
42
43.
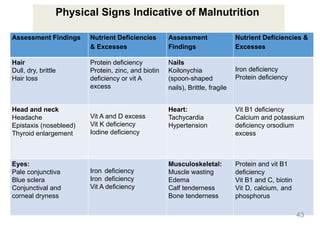
Physical Signs Indicativeof Malnutrition
Assessment Findings Nutrient Deficiencies
& Excesses
Assessment
Findings
Nutrient Deficiencies &
Excesses
Hair
Dull, dry, brittle
Hair loss
Protein deficiency
Protein, zinc, and biotin
deficiency or vit A
excess
Nails
Koilonychia
(spoon-shaped
nails), Brittle, fragile
Iron deficiency
Protein deficiency
Head and neck
Headache
Epistaxis (nosebleed)
Thyroid enlargement
Vit A and D excess
Vit K deficiency
Iodine deficiency
Heart:
Tachycardia
Hypertension
Vit B1 deficiency
Calcium and potassium
deficiency orsodium
excess
Eyes:
Pale conjunctiva
Blue sclera
Conjunctival and
corneal dryness
Iron deficiency
Iron deficiency
Vit A deficiency
Musculoskeletal:
Muscle wasting
Edema
Calf tenderness
Bone tenderness
Protein and vit B1
deficiency
Vit B1 and C, biotin
Vit D, calcium, and
phosphorus
43
44.
Dietary Assessment
● Thismethod involves assessing the past or current intake of nutrients
from food by individuals or groups
● Dietary assessment can help evaluate the quality and quantity of food
consumption, identify dietary patterns and preferences, and provide
nutrition education and counseling
● Dietary assessment involves documenting of intake using
dietary subjective report and objective observation.
● Subjective dietary assessment uses methods such as 24-hours’
dietary recall (24HR), dietary history, Food Frequency Questionnaire.
● Objective data are collected with the help of a trained interviewer.
44
45.
24 Hour Recall
•Clientsare asked to report all foods and beverages
consumed in the past 24 hours.
•Interviewer must be trained to prompt for details
such as cooking methods and portion sizes.
45
Diet History
• Clients’record food and beverages consumed over three
consecutive days (usually one weekdays and two
weekend days)
• The consumed items can be measured using a scale or
other household items, such as measuring spoons or
estimated using a portion size guideline.
47
48.
Food Frequency Questionnaire(FFQ)
● Clients report how frequently certain food and
beverages item were consumed over a specific period
of time.
● Most FFQ version ask portion size, questions of every
food item, as well as general questions about common
cooking practices
48
49.
● This isa well-validated tool to identify older adults
who are malnourished or at risk of becoming
malnourished.
● It consists of 18 items that cover anthropometric,
dietary, lifestyle, and health-related factors.
● It gives a score that indicates the nutritional status
of the individual
Mini Nutritional Assessment
49
50.
● This isa well-validated tool to identify older adults
who are malnourished or at risk of becoming
malnourished.
● It consists of 18 items that cover anthropometric,
dietary, lifestyle, and health-related factors.
● It gives a score that indicates the nutritional status of
the individual
Mini Nutritional Assessment
50
51.
● This isa clinical method that involves a comprehensive
history and physical examination of the patient.
● It evaluates weight changes, dietary intake, gastrointestinal
symptoms, functional capacity, and physical signs of
malnutrition.
● It classifies the patient into one of three categories: well
nourished, moderately malnourished, or severely
malnourished
Subjective Global Assessment
51
52.
● Malnutrition UniversalScreening Tool (MUST) is a simple
and practical tool that can be used in various settings.
● It assesses the risk of malnutrition based on body mass
index, unintentional weight loss, and acute disease effect.
● It provides a score that indicates the level of risk and a
management plan based on the score
Malnutrition Universal Screening Tool
52
53.
● Nutrition RiskScreening 2002 (NRS 2002) is a tool that is
designed for hospitalized patients.
● It screens for the presence of impaired nutritional status
and increased nutritional requirements.
● It considers age, weight loss, body mass index, severity of
disease, and reduced dietary intake.
● It gives a score that indicates the need for nutritional
support
Nutrition Risk Screening 2002
53
54.
Importance of NutritionalAssessment
Nutritional assessment can help to:
● Prevent and treat malnutrition and its complications, such as
infections, delayed wound healing, impaired immune response, and
increased morbidity and mortality.
● Improve the quality of life and functional status of patients and
clients, especially those with chronic conditions, such as diabetes,
cardiovascular disease, and cancer.
● Enhance the effectiveness and safety of medical therapies, such as
surgery, chemotherapy, and radiotherapy.
● Reduce the length of hospital stay and the cost of health care. [3]
54
CONCLUSION
● Nutrition assessmentis a vital tool nurses and midwives can
utilize to render effective and efficient service to the
community.
● If effectively done, can assist to nib in the bud most of the life
threatening non communicable diseases and indeed help
save the lives of significant numbers adolescent girl and
women of reproductive age.
● Its effective utilization can be of immense benefit to the
people’s wellbeing, quality life and longevity.
58



![Introduction Cont...
● Nutritional assessment is the interpretation of
anthropometric, biochemical, clinical and dietary data
to determine whether a person or groups of people
are well nourished or malnourished [1]
6](https://image.slidesharecdn.com/nutritionalassessment-260209082634-0e76e16f/85/Nutritional-Assessment-in-Nursing-Practice-6-320.jpg)
![Introduction Cont...
● Nutritional assessment is important for
identifying people at risk of malnutrition,
informing nutrition education and counseling,
establishing appropriate nutrition care plans,
and evaluating the effectiveness of nutrition
interventions. [1]
7](https://image.slidesharecdn.com/nutritionalassessment-260209082634-0e76e16f/85/Nutritional-Assessment-in-Nursing-Practice-7-320.jpg)
![Malnutrition Epidemiology
Malnutrition associated with increased complications
Poor wound healing
Immunocompromised status
Organ function impairment
Healthcare utilization (resources and cost)
30- 50% prevalence, depending on the criteria and practice setting
studied
Morbidity/Mortality. [9]
9](https://image.slidesharecdn.com/nutritionalassessment-260209082634-0e76e16f/85/Nutritional-Assessment-in-Nursing-Practice-9-320.jpg)
![Main Components
● Anthropometric assessment
● Biochemical assessment
● Clinical assessment
● Dietary assessment
The ABCD Methods of Nutritional Assessments
● Note: The ABCD methods of nutritional assessment are
complementary and should be used together to obtain a
comprehensive and accurate evaluation of the nutritional
status of individuals or groups. [4]
20](https://image.slidesharecdn.com/nutritionalassessment-260209082634-0e76e16f/85/Nutritional-Assessment-in-Nursing-Practice-20-320.jpg)





![Importance of Nutritional Assessment
Nutritional assessment can help to:
● Prevent and treat malnutrition and its complications, such as
infections, delayed wound healing, impaired immune response, and
increased morbidity and mortality.
● Improve the quality of life and functional status of patients and
clients, especially those with chronic conditions, such as diabetes,
cardiovascular disease, and cancer.
● Enhance the effectiveness and safety of medical therapies, such as
surgery, chemotherapy, and radiotherapy.
● Reduce the length of hospital stay and the cost of health care. [3]
54](https://image.slidesharecdn.com/nutritionalassessment-260209082634-0e76e16f/85/Nutritional-Assessment-in-Nursing-Practice-54-320.jpg)































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










