2. Vasculitis
Definition: inflammation of blood vessels caused by injury from leukocytes.
Most often classified by the size of the blood vessels affected.
The involved vessels determine the symptoms and signs.
Large Vessels- Aorta and the great vessels (subclavian, carotid)
CVA, claudication, blindness
Giant Cell Arteritis, Takayasu’s arteritis
Medium Vessels- Arteries with muscular wall
Mesenteric ischemia, cutaneous ulcers, mononeuritis multiplex
Polyarteritis Nodosa
Kawasaki Disease
Buerger’s Disease
Small Vessels- Capillaries, arterioles, venules
Palpable purpura, glomerulonephritis, pulmonary hemorrhage
ANCA Vasculitides (GPA, MPA, EGPA)
Cryoglobulinemic Vasculitis
IgA Vasculitis (HSP)
Anti-GBM
3.
4. Cryoglobulins
• Immunoglobulins that are characterized by their
insolubility at low temperatures and their dissolution
after rewarming.
• Classified based on their immunochemical composition:
- Single cryoglobulinemia = only one Ig isotype (IgM, IgG,
IgA, or less commonly free Ig light chains) that is
monoclonal (type I)
- Mixed cryoglobulinemia = two or more Ig isotypes
Type II- at least one of the Igs is monoclonal
Type III- all Ig isotypes are
polyclonal
*Over 90% of patients with mixed cryoglobulinemia are
HCV positive.
5. Detectable levels of circulating
cryoglobulins, without clinical
manifestations of vasculitis, have
been seen in a significant proportion
of patients with chronic infections or
inflammatory syndromes.
15-20% in HIV
15-25% in connective tissue diseases
40-65% in HCV
As high as 64% in HIV/HCV
coinfection
6. Illness Script
Epidemiology Prevalence is approximately 1 in 100,000
Pathophysiology Immune complex-mediated small- to medium-vessel vasculitis caused by
cryoglobulin-containing immune complexes.
Time Course Variable
Clinical Presentation Palpable purpura, arthralgias, fatigue, weakness, Raynaud’s phenomenon, peripheral
neuropathy, renal disease, signs of vascular occlusion including digital ischemia,
levido reticularis, and skin necrosis.
Diagnosis Clinical symptoms and labs +/- tissue biopsy
7. Clinical Features
• Cutaneous manifestations occur in nearly all patients
with cryoglobulinemic syndromes:
• Erythematous macules or purpuric papules,
typically over the lower extremities (90-95%).
• Hemorrhagic crusts, digital infarction, ulcers (10-
25%).
• Raynaud’s, livedo reticularis, acrocyanosis (more
common in type I).
• Postinflammatory hyperpigmentation (30-50%).
• Arthralgias (> 70% of patients). Most commonly in the
MCPs, PIPs, knees, and ankles. Typically exacerbated
by cold weather. Most common in type III, uncommon
in type I.
• Peripheral neuropathy (30-80%), most often seen in
types II or III.
8. Clinical Features
• Renal disease- typically a membranoproliferative
glomerulonephritis secondary to immune complex
deposition. Can also occur as a result of thrombotic disease
(seen in type I).
• Pulmonary involvement- usually subclinical with PFTs
showing evidence of small airway disease or impaired gas
exchange. Symptoms include dyspnea, cough, or pleurisy.
Occurs in 10-20% of patients, most commonly in types II or
III.
• Symptoms of hyperviscosity may also occur, mainly in type I
disease.
Blurry vision Ataxia
Headache Confusion
Diplopia Stroke
Vertigo Sudden deafness
Nystagmus
9. Pathophysiology
• A small- to medium-vessel vasculitis mediated by the precipitation of cryoglobulins
in the walls of blood vessels.
• Important distinction between cryoglobulinemia versus cryoglobulinemic vasculitis
as minute levels of cryoglobulins are often present in the serum of healthy
individuals.
• Pathogenic cryoglobulin levels are thought to be mediated by three main
mechanisms:
• Chronic immune stimulation and/or lymphoproliferation, resulting in higher
levels of immunoglobulins that can form cryoglobulins
• Enhanced immune complex formation
• Insufficient clearance of immune complexes, which then accumulate and
deposit in the wrong places
• Type I cryoglobulinemia: predominantly affects the skin, kidney, and bone marrow.
The main pathologic features are more often related to thrombosis.
• Types II and III cryoglobulinemia: predominantly affect the skin, kidney, and
peripheral nervous system. The main pathologic features are related to immune
complex vasculitis.
• Genome-wide association studies have shown an association between
cryoglobulinemic vasculitis and SNPs near the NOTCH4 and MHC Class II genes.
10. Brouet Classification
• Classifies cryoglobulinemia into three different subgroups based on the composition of the involved
immunoglobulins.
• Each subgroup partly correlates with pathogenicity and certain clinical features.
Type Composition Percent of Cases Associated Diseases
Type I Monoclonal (IgG, IgM,
or IgA)
10-15% Hematologic diseases: multiple
myeloma, Waldenstrom’s
macroglobulinemia, MGUS, CLL, B-cell
lymphomas
Type II Monoclonal IgM with RF
activity PLUS polyclonal
IgG or, rarely, IgA
50-60% HCV, HIV, HCV/HIV coinfection, HBV,
lymphoproliferative disorders,
autoimmune diseases (mainly SLE or
Sjogren’s syndrome)
Type III Polyclonal IgM PLUS
polyclonal IgG or IgA
25-30% Autoimmune diseases, particularly
Sjogren’s syndrome and less commonly,
SLE and RA. Can also be associated with
infections, mainly HCV.
11. Diagnosis
• Clinical features
Higher index of suspicion if classic signs/symptoms occur in the setting of
a clonal hematologic disease (multiple myeloma, Waldenstrom
macroglobulinemia), viral infection (HCV, HBV), or connective tissue
disease (RA, lupus, or Sjogren’s Disease).
PLUS
• Elevated cryocrit (does not correlate with disease severity or response to
therapy)
Most prominent lab hallmarks:
Elevated cryoglobulins ( > 1% or > 50 mcg/L)
Low C4 (mixed cryoglobulinemia)
Levels of C3 are generally unaffected or mildly diminished
• Immunochemical Analysis- determination of cryoglobulin isotype.
- Cryoglobulins are warmed and immunofixation is performed with
antibodies directed to various Ig heavy chains and light chains and to
complement components (e.g., C1q, C4, C3).
• Histologic confirmation of leukocytoclastic vasculitis on skin biopsy is NOT
needed if the patient has typical palpable purpura.
• Direct histologic or immunochemical evidence of cryoglobulins from
pathologic specimens- most definitive evidence for diagnosis but not part of
the formal criteria.
12. Additional Lab Studies
• Cr, UA
• RF (most often elevated in type
II), anti-CCP
• CH50 (often reduced in mixed
cryoglobulinemia)
• C1q, C2 (most useful for type II)
• HCV, HBV, HIV, EBV, CMV
• ESR, CRP
• ANA, anti-dsDNA, ANCA, anti-
Sm, Ro/SSA, La/SSB, RNP
13. Other Testing
• Imaging
• Skin Biopsy
• Mixed: most often reveals a leukocytoclastic vasculitis (~50%).
• Type I: more often noninflammatory thrombotic lesions,
sometimes with evidence of cutaneous infarction or
hemorrhage.
• Direct immunofluorescence microscopy of acute lesions often
reveals deposits of IgM, IgG, and/or C3 complement.
• Tissue Biopsy Otherwise
• Peripheral Nerve: typically show a vasculitis of the epineural
vessels. Necrotizing vasculitis or demyelination may be present.
Most studies have used sural nerve biopsies.
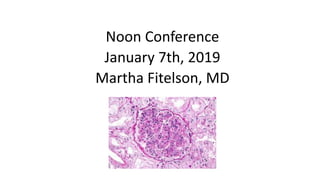
• Kidney: membranoproliferative glomerulonephritis on light
microscopy (60-80% in mixed) and granular or amorphous
subendothelial deposits on electron microscopy.
• Bone Marrow: In type 1, often reveals evidence of a
hematologic malignancy
• EMG: useful if neuromuscular involvement, such as
mononeuritis multiplex
14. Treatment
Two broad principles:
1.) Initial immunosuppressive therapy: provided for patients
with a rapidly progressive, organ- or life-threatening course
regardless of the underlying etiology. Usually includes a short
course of high dose glucocorticoids combined with either
Rituxan or Cyclophosphamide and, in some patients,
plasmapheresis.
2.) Treatment of underlying disease: antiviral therapy for those
with HCV (or other viral etiologies) or disease-specific therapy
for patients with lymphoproliferative disorders.
- Generally, treat with immunosuppression FIRST, then treat
the underlying etiology.
- Exceptions: patients with HIV or HBV, in which case you start
antiviral therapy at the same time or before
immunosuppressive agents.
15. Support for Immunosuppressive Therapy at the
Treatment Outset
Prospective Cohort Study (2010)
Rituximab plus Peg-interferon-alpha/ribavirin compared with Peg-
interferon-alpha/ribavirin in HCV-related mixed cryoglobulinemia
93 patients total with HCV Mixed Cryoglobulinemia (HCV-MC)
55 patients: peg-interferon-α weekly plus Ribavirin daily x 48 weeks
38 patients: Rituximab weekly x one month followed by peg-
interferon-α plus Ribavirin
*Patients who received combination therapy had more severe disease at
study outset.
Median Follow-Up at 48 months:
Similar response rates (74% vs. 73%) but the time to clinical response was
significantly shorter in the combination group (5.4 vs. 8.4 months) (p <
0.004).
Combination group: better renal response rates (80.9% vs. 40%, p = 0.04),
higher rates of cryo clearance (68.4% vs. 43.6%, p = 0.001), and enhanced
clonal B cell suppression (p < 0.01).
16. Role of Plasma Exchange
Typically administered daily for 10-14 sessions or three exchanges weekly x 2-
3 weeks. One plasma volume (~3L) should be exchanged per session.
Changes in the percent cryocrit following plasmapheresis do NOT correlate
with clinical activity. Assess treatment response by clinical evaluation.
Several settings in which it should be considered:
- Life-threatening disease (acute respiratory failure, pulmonary
hemorrhage, acute intestinal vasculitis)
- Symptomatic hyperviscosity syndrome
- Patients with rapidly progressive glomerulonephritis who require dialysis.
Late initiation of plasma exchange (two or more weeks after initiation of
dialysis) is unlikely to be beneficial.
- Severe or refractory skin ulcers due to cutaneous vasculitis
*Plasma exchange does not prevent the formation of new cryoglobulins, so
it is imperative to combine it with immunosuppressive therapy directed at
B-cell clones!