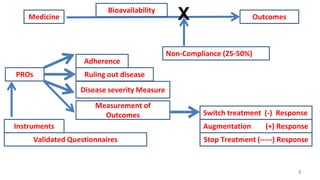
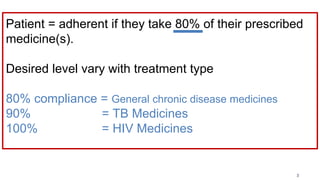
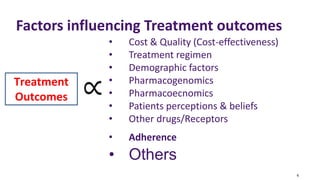
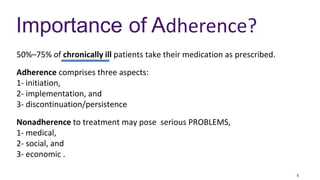
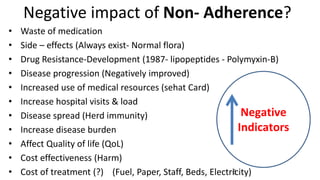
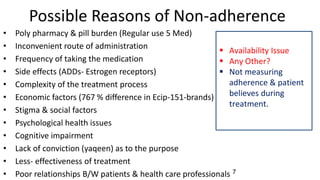
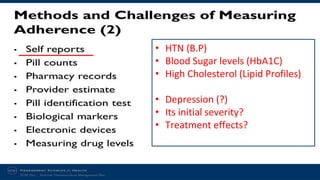
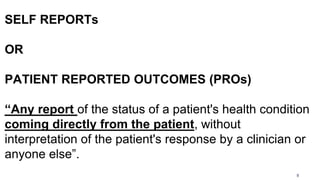
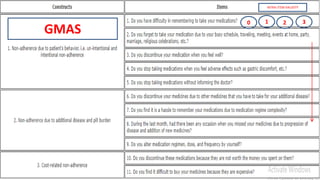
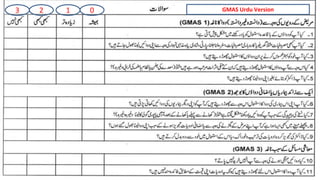
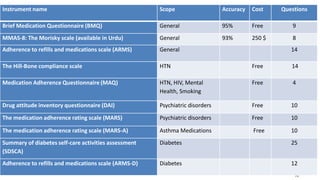
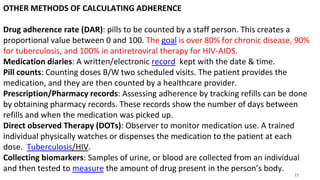
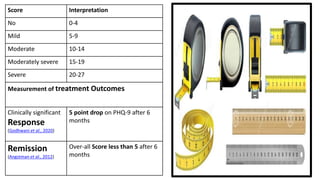
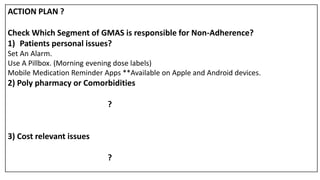
The document discusses medication non-compliance and various ways to measure it. It notes that 50-75% of chronically ill patients do not take their medication as prescribed. Several validated questionnaires are available to measure adherence, including the Morisky Medication Adherence Scale (MMAS-8) and the General Medication Adherence Scale (GMAS). Measuring adherence through questionnaires, pill counts, pharmacy records, and biomarkers can help healthcare providers understand reasons for non-compliance and address them to improve treatment outcomes.































![Group 03 QbD[1].pptxvvvvvvvvvvvvvvvvvvffff](https://cdn.slidesharecdn.com/ss_thumbnails/group03qbd1-240324171757-864b5c1b-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






