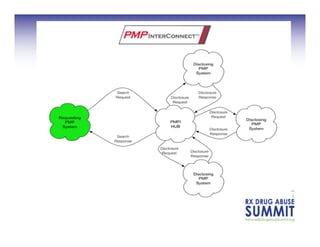
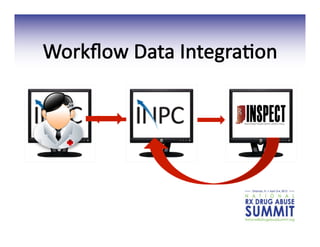
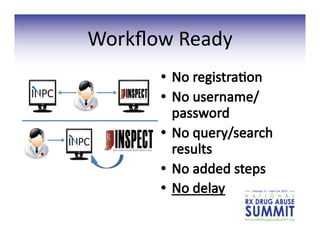
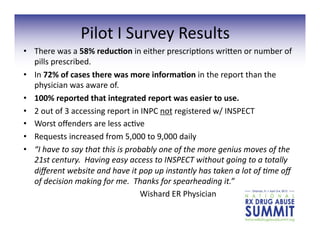
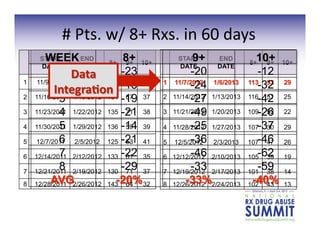
This document summarizes a presentation on recent developments related to Prescription Drug Monitoring Programs (PDMPs). The presentation covered: an overview of PDMPs including their role in tracking controlled prescription drugs; best practices for PDMPs based on research; evidence that PDMPs can effectively reduce prescription drug abuse and overdoses when certain criteria are met; and current initiatives to improve interstate data sharing and integrate PDMP data into healthcare workflows through health IT. The goal is to leverage PDMPs to improve clinical care and public health outcomes related to prescription drug misuse.


![16
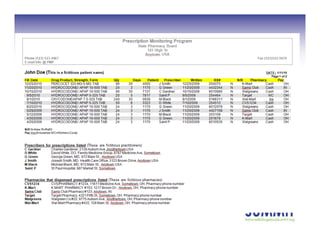
PDMP
Effec;veness
grey
literature
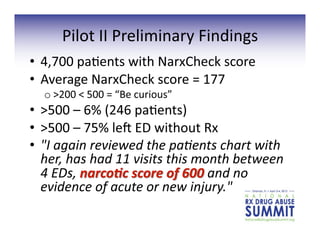
• Surveys
indicate
prescribers
find
PDMPs
to
be
a
useful
clinical
tool.
• Surveys
find
clinicians
in
many
cases
report
altering
their
prescribing
a]er
reviewing
a
PDMP
report.
• Proac;ve
repor;ng
reduces
doctor
shopping
by
increasing
awareness
among
providers
about
at-‐risk
pa;ents
leading
to
changes
in
prescribing
behaviors.
1.
PMP
Center
of
Excellence,
“Trends
in
Wyoming
PMP
prescrip3on
history
repor3ng:
evidence
for
a
decrease
in
doctor
shopping?”
2010,
hgp://www.pmpexcellence.org/sites/all/pdfs/NFF_wyoming_rev_11_16_10.pdf
2.
PMP
Center
of
Excellence,
“Nevada’s
Proac3ve
PMP:
The
Impact
of
Unsolicited
Reports”
October,
2011.
hgp://www.pmpexcellence.org/sites/all/pdfs/nevada_nff_10_26_11.pdf
4.
Alliance
of
States
with
Prescrip3on
Monitoring
Programs,
“An
Assessment
of
State
Prescrip3on
Monitoring
Program
Effec3veness
and
Results”
Version
1,
11.30.07,
hgp://
pmpexcellence.org/pdfs/alliance_pmp_rpt2_1107.pdf
5.
Kentucky
Cabinet
for
Health
and
Family
Services
and
Kentucky
Injury
Preven3on
and
Research
Center,
2010
KASPER
Sa3sfac3on
Survey.
6.
Lambert
D.
Impact
evalua3on
of
Maine’s
prescrip3on
drug
monitoring
program.
Muskie
School
of
Public
Service,
University
of
Southern
Maine:
Portland,
Maine,
March,
2007.
7.
Communica3on
from
LA
PMP
to
PMP
Center
of
Excellence.](https://image.slidesharecdn.com/newpdmpdevelopmentsfinal-130328084634-phpapp02-150514035500-lva1-app6891/85/Newpdmpdevelopmentsfinal-130328084634-phpapp02-16-320.jpg)






























![The-Case-for-Practice-Integration[1]](https://cdn.slidesharecdn.com/ss_thumbnails/f8309d43-8226-4580-ab57-0beb0b770357-160412231650-thumbnail.jpg?width=640&height=640&fit=bounds)






![[1] rpp sd kelas 6 bhinneka tunggal ika](https://cdn.slidesharecdn.com/ss_thumbnails/1rppsdkelas6-bhinnekatunggalika-151008024944-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

![[1] rpp sd kelas 6 bhinneka tunggal ika](https://cdn.slidesharecdn.com/ss_thumbnails/1rppsdkelas6-bhinnekatunggalika-150829053745-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
























