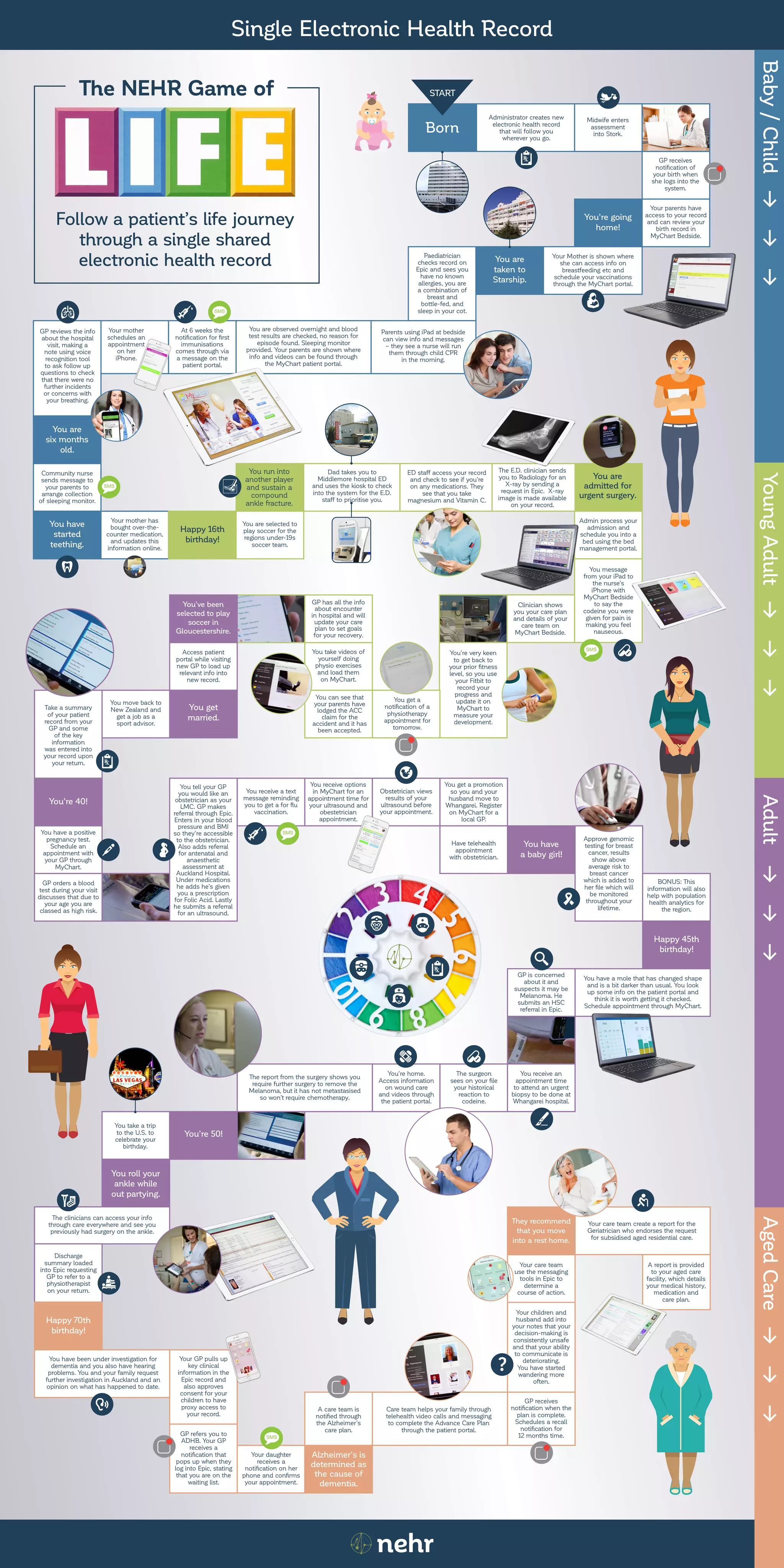
This document summarizes a patient's life journey through a single shared electronic health record from birth to aged care. Key events include the patient's birth record being created, various medical encounters like injuries and illnesses throughout life that are documented in the record and accessible by different care providers, and the patient's record being updated with information as they age, such as an advance care plan. The single shared record allows information to be continuously updated and accessible to support the patient's care at each stage of life.