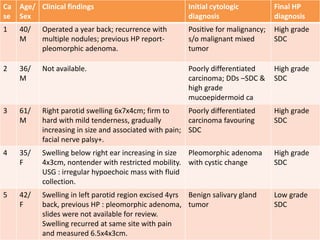
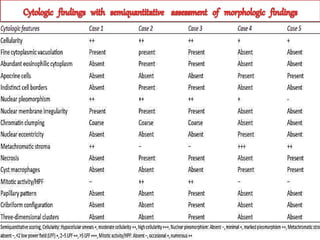
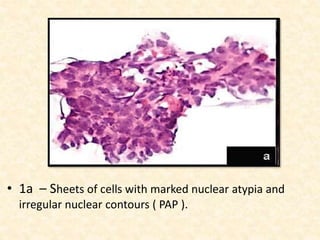
This study analyzed the cytological features of 5 cases of salivary duct carcinoma (SDC) diagnosed by fine needle aspiration biopsy and correlated them with histopathology findings. SDC is an aggressive salivary gland cancer that resembles breast cancer microscopically. On cytology, SDC commonly shows sheets of atypical cells with irregular nuclei, prominent stroma, and necrosis. While some cases clearly showed malignant features, others were more difficult to diagnose due to milder abnormalities. Immunohistochemistry may help in diagnosing ambiguous SDC cases. The study concluded that cytology is generally accurate for SDC, but ancillary tests are sometimes needed for definitive diagnosis, especially in less obviously malignant cases.

![Presentation dr rahul seminar (2)[1387]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationdrrahulseminar21387-210324042322-thumbnail.jpg?width=640&height=640&fit=bounds)














































