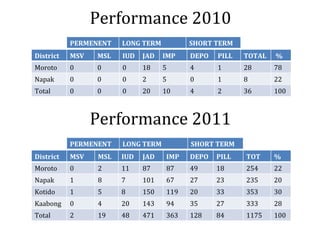
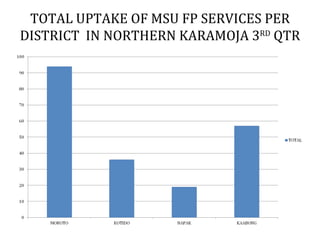
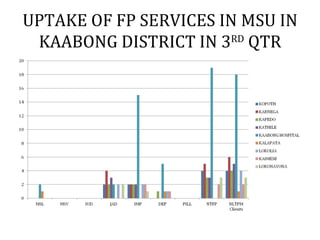
The document summarizes MSI's family planning services in Northern Karamoja, Uganda for the third quarter of 2012. MSI provided family planning services through outreaches to health facilities in Moroto, Napak, Kotido, and Kaabong districts. The report shows uptake of various family planning methods by district for 2010, 2011, and the third quarter of 2012. It identifies challenges like low uptake due to cultural beliefs and lack of spouse support, as well as opportunities to increase training and outreach.