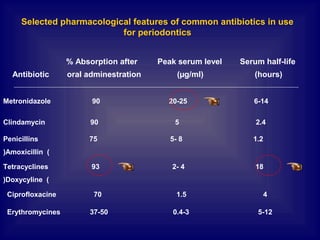
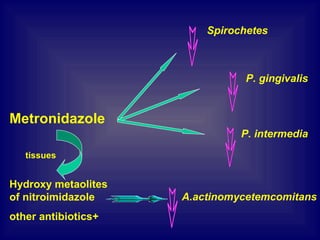
- Metronidazole is commonly used antibiotic in periodontal therapy that is effective against anaerobic bacteria. It can attain effective concentrations in gingival tissues, saliva, and crevicular fluid.
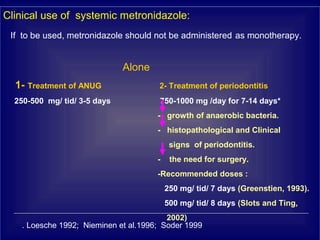
- Systemic antibiotic therapy with metronidazole should be reserved for acute periodontal infections, as an adjunct to periodontal treatment, or for patients who continue experiencing periodontal breakdown despite treatment.
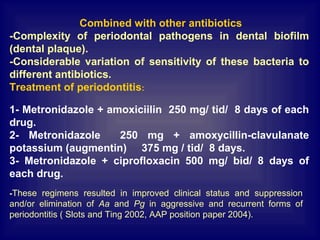
- When using metronidazole, it is recommended to not use it as a monotherapy but combine it with other antibiotics like amoxicillin or ciprofloxacin. Common dosing regimens include 250mg of metronidazole three times daily combined