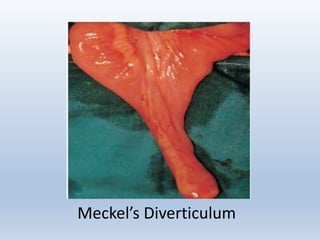
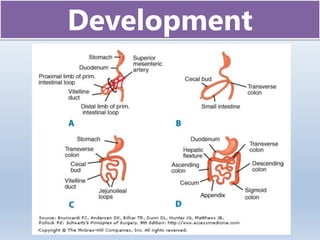
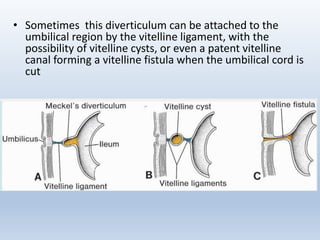

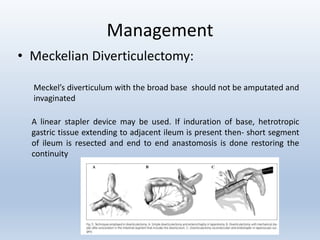
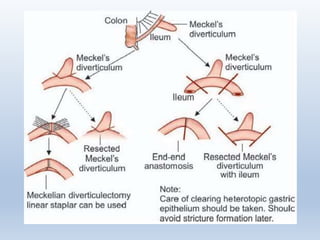


Meckel's diverticulum is the most common congenital abnormality of the gastrointestinal tract, affecting approximately 2% of the population. It is a true diverticulum that forms from incomplete closure of the vitelline duct during fetal development. Meckel's diverticulum can contain heterotopic gastric or pancreatic tissue which can lead to ulceration and bleeding. Clinical presentations include hemorrhage, intestinal obstruction, diverticulitis, and intussusception. Diagnosis is often made through scans like a Meckel's scan or CT scan, and treatment involves surgical resection of the diverticulum.

















































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)




![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)