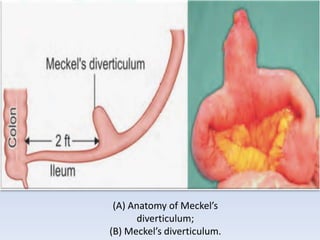
Meckel's diverticulum is a congenital diverticulum that arises from the terminal ileum due to incomplete closure of the vitellointestinal duct during fetal development. It is the most common congenital anomaly of the small intestine. Symptomatic cases typically present with severe hemorrhage in children under 2 years old. A technetium scan is a useful diagnostic tool to detect Meckel's diverticulum, including cases with minimal bleeding. Treatment involves resection of the affected segment of ileum containing the diverticulum.