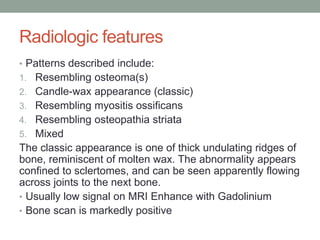




1. Melorheostosis is a rare sclerosing bone disorder of unknown cause that produces thickened bone along the surface and inner lining of bones. 2. It most commonly affects the lower extremities in individuals between 5-20 years old and presents with bone overgrowth patterns resembling candle wax or myositis ossificans on imaging. 3. Affected individuals may experience pain, joint stiffness, deformities, and leg length discrepancies. Skin thickening and vascular abnormalities can also occur.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)