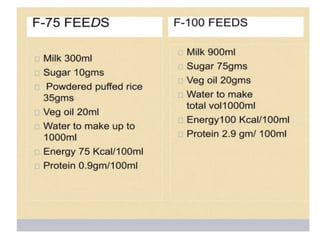
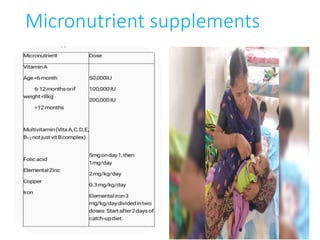
The document discusses several national health programs related to maternal and child health in India. It describes the objectives and components of programs like Mission Indradhanush, which aims to increase immunization coverage across the country, the Adolescent Reproductive and Sexual Health (ARSH) Program, the Weekly Iron Folic Acid Supplementation program, the Menstrual Hygiene Scheme, and the management of children in Nutritional Rehabilitation Centers. Key details provided include the phases of Mission Indradhanush, components of ARSH like adolescent friendly clinics and outreach activities, and the stabilization, transition, and rehabilitation phases of hospital-based management in NRCs.