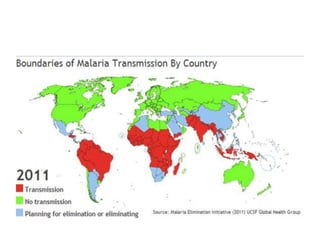
1. Malaria is a major global health problem caused by Plasmodium parasites and transmitted via mosquito bites. P. falciparum causes the most severe and potentially fatal form of the disease.
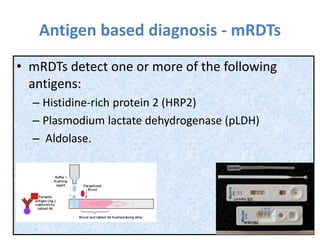
2. Accurate diagnosis of malaria species and parasite load is important for guiding treatment. Standard diagnosis methods include microscopy of blood smears and rapid diagnostic tests detecting malaria antigens.
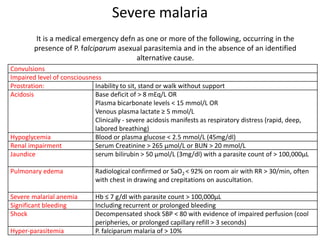
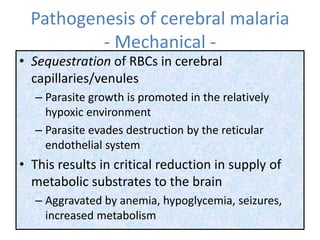
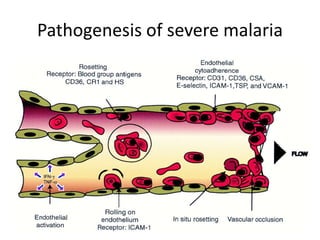
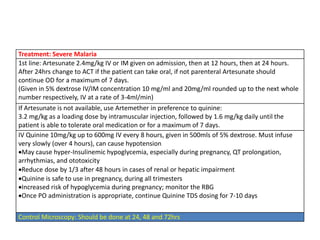
3. Severe malaria is a medical emergency defined by danger signs such as cerebral malaria, jaundice, severe anemia, respiratory distress, or low blood sugar, and requires prompt parenteral treatment with artemisinin derivatives like artesunate or quinine.