Download as PDF, PPTX

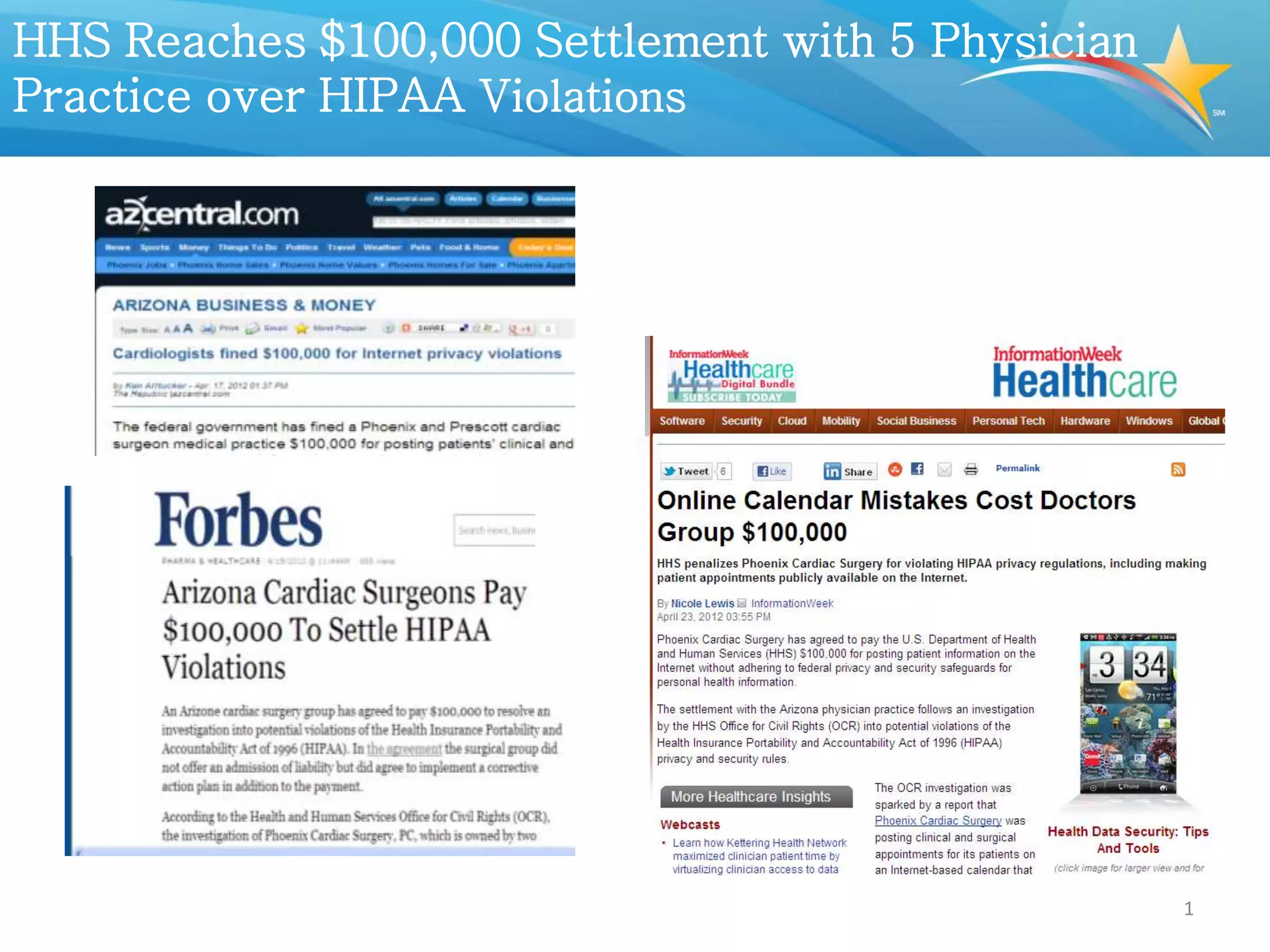
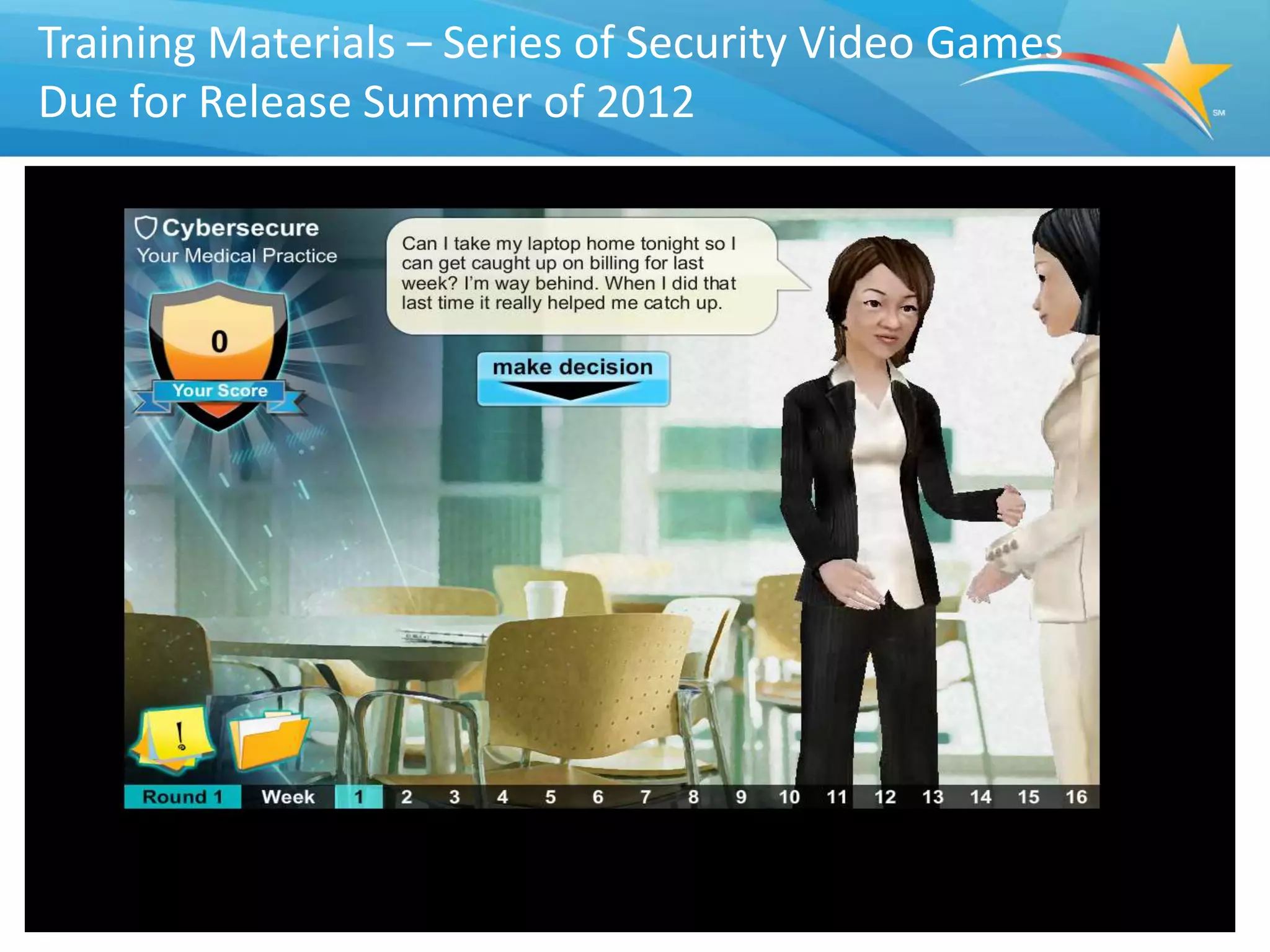


The document outlines the importance of creating a culture of privacy and security in healthcare organizations to comply with HIPAA regulations and protect patient trust. It discusses the roles of covered entities and business associates, recent breaches highlighting compliance failures, and the consequences of insufficient security practices. Additionally, it emphasizes strategies for improving privacy and security culture within healthcare organizations and the government's role in providing guidance and resources.



































































































