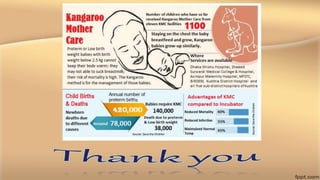
This document summarizes a study on implementing kangaroo mother care (KMC) in secondary level health facilities in Bihar, India. The study found that after intervention, there was a definite improvement in awareness of KMC among nurses and midwives. It also impacted infrastructure to allow for KMC in selected facilities. However, the study duration was relatively short and involved a small number of facilities, limiting the ability to fully assess the intervention's impact. Improving funding, determining sample size, and strengthening data collection could help strengthen future studies on rolling out KMC.