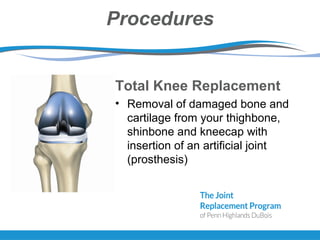
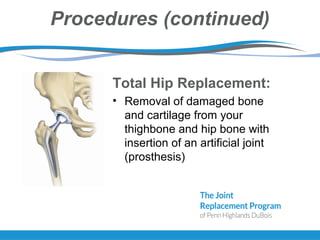
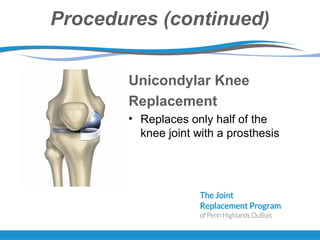
The document provides information about total joint replacement surgery and recovery. It discusses the procedures for total knee, total hip, and unicompartmental knee replacement surgeries. It outlines the pre-operative education process, what to expect during hospitalization including physical and occupational therapy, pain management, and discharge planning. The roles of nursing, physical therapy, social work, and caregivers in the recovery process are also summarized.