FATE OF REDBLOOD CELLS
Life span in blood stream is 60-120 days
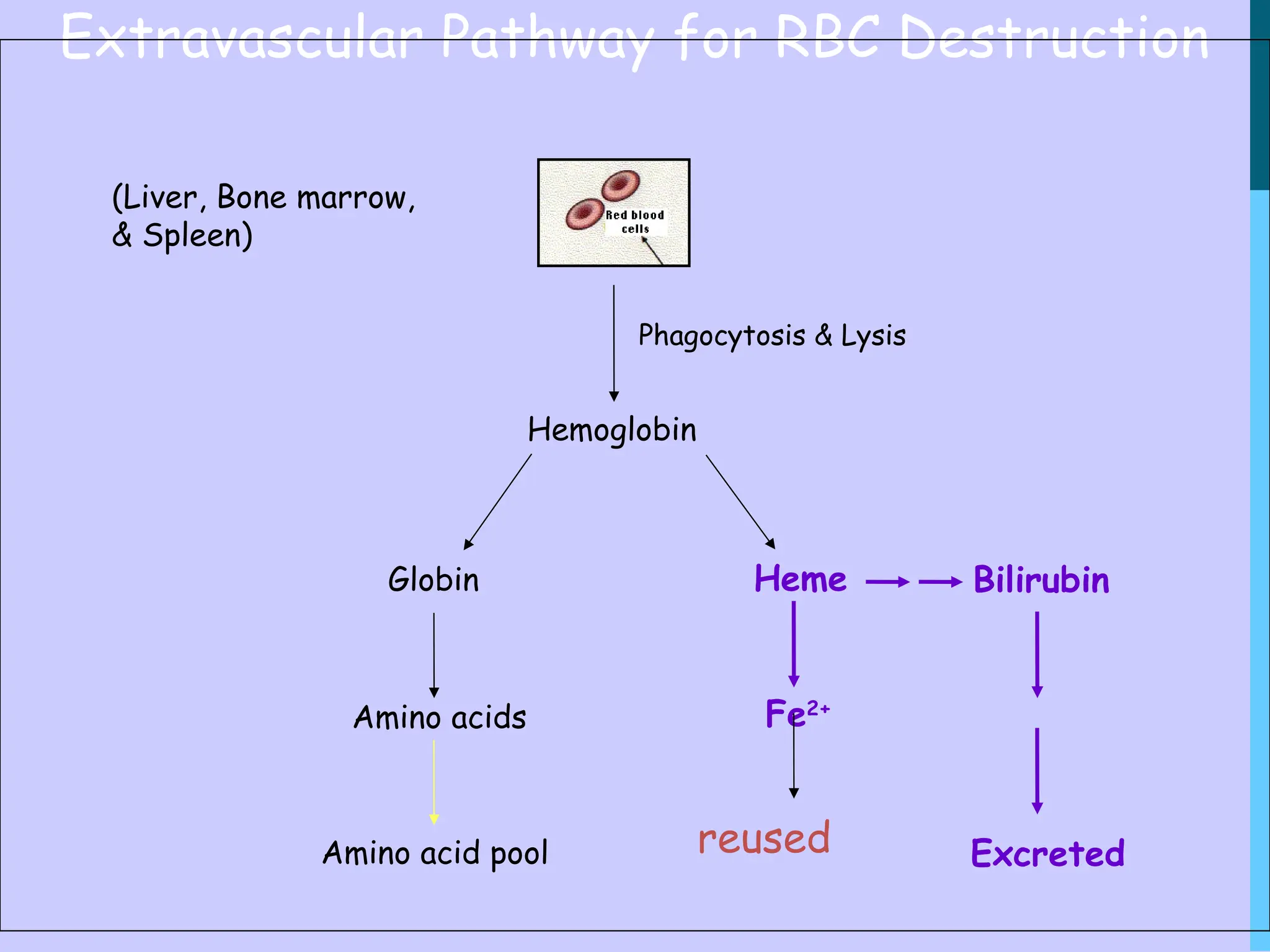
Senescent RBCs are phagocytosed and lysed
by tissue macrophages which are a part of
reticuloendothelial system.
Lysis can also occur intravascularly (in blood
stream)
Handling of Free(Intravascular) Hemoglobin
• Haptoglobin: hemoglobin-
haptoglobin complex is readily
metabolized in the liver and spleen
forming an iron-globin complex and
bilirubin. Prevents loss of iron in
urine
5.
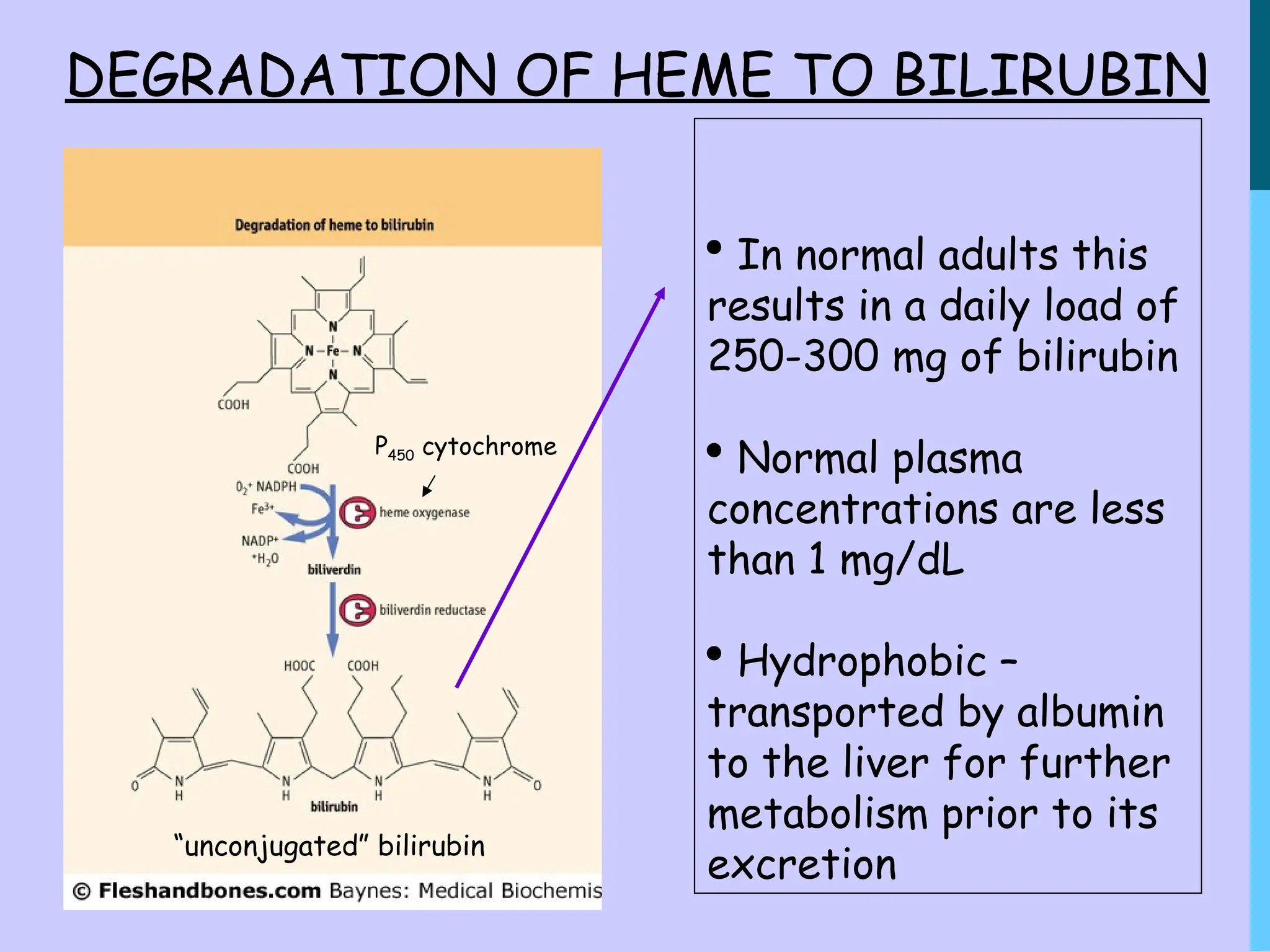
DEGRADATION OF HEMETO BILIRUBIN
P450 cytochrome
In normal adults this
results in a daily load of
250-300 mg of bilirubin
Normal plasma
concentrations are less
than 1 mg/dL
Hydrophobic –
transported by albumin
to the liver for further
metabolism prior to its
excretion
“unconjugated” bilirubin
6.
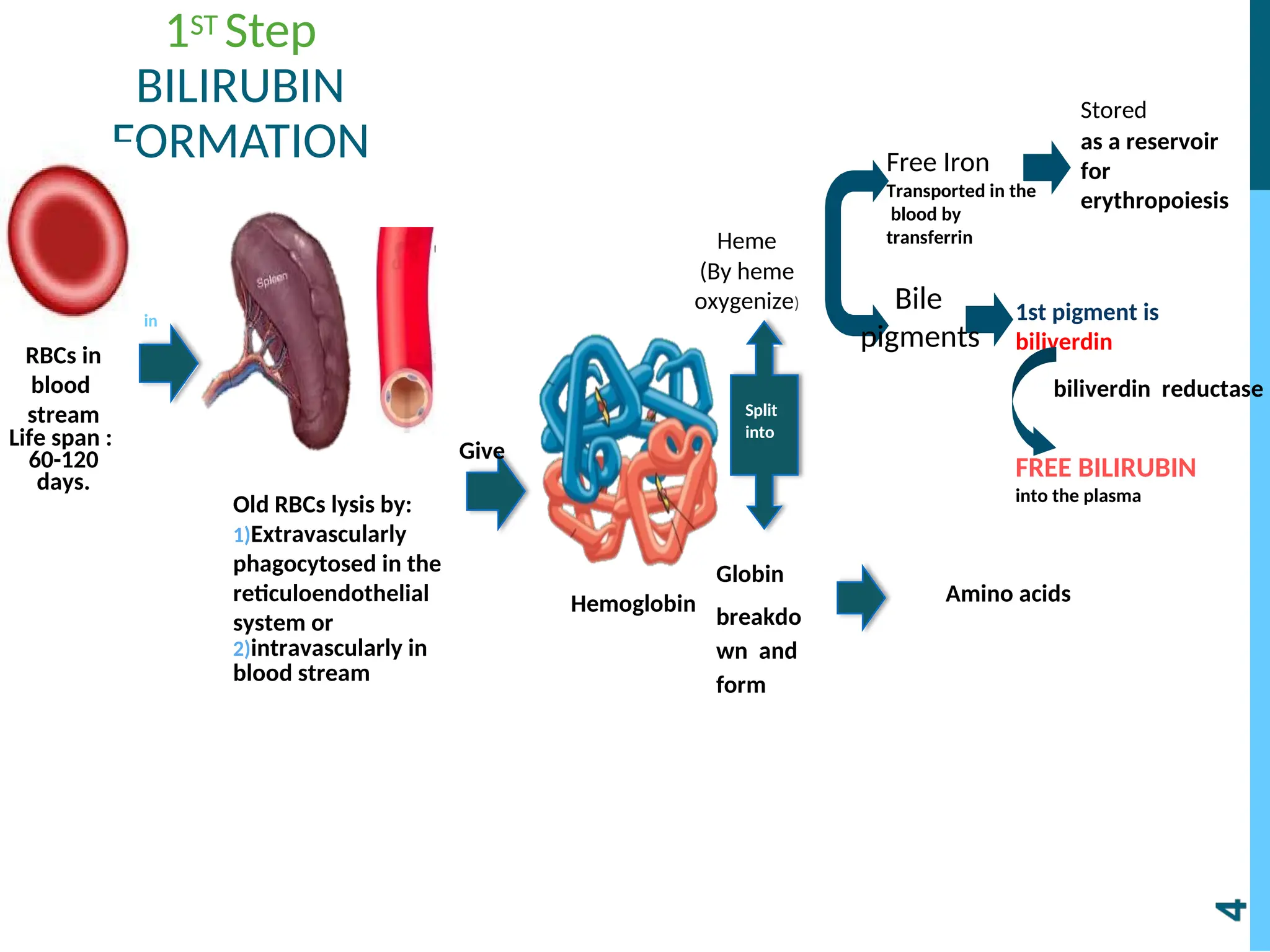
1ST Step
BILIRUBIN
FORMATION
RBCs in
blood
stream
Lifespan :
60-120
days.
Old RBCs lysis by:
1)Extravascularly
phagocytosed in the
reticuloendothelial
system or
2)intravascularly in
blood stream
Hemoglobin
in
Give
Split
into
Globin
breakdo
wn and
form
Amino acids
Free Iron
Transported in the
blood by
transferrin
Stored
as a reservoir
for
erythropoiesis
1st pigment is
biliverdin
FREE BILIRUBIN
into the plasma
Bile
pigments
biliverdin reductase
Heme
(By heme
oxygenize)
8.
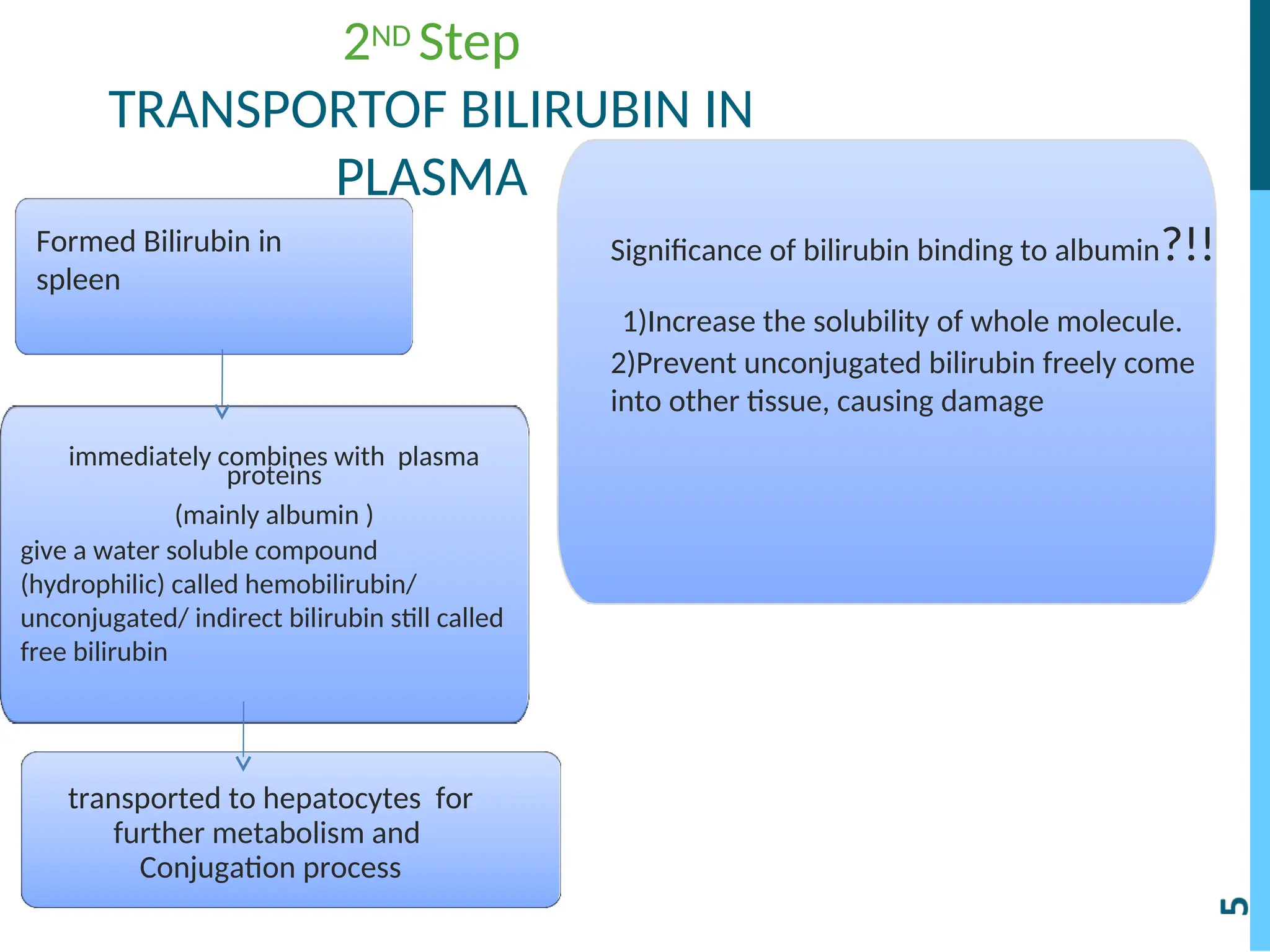
2ND Step
TRANSPORTOF BILIRUBININ
PLASMA
Formed Bilirubin in
spleen
immediately combines with plasma
proteins
(mainly albumin )
give a water soluble compound
(hydrophilic) called hemobilirubin/
unconjugated/ indirect bilirubin still called
free bilirubin
transported to hepatocytes for
further metabolism and
Conjugation process
Significance of bilirubin binding to albumin?!!
1)Increase the solubility of whole molecule.
2)Prevent unconjugated bilirubin freely come
into other tissue, causing damage
9.
Hepatic uptake “1stStep”-
Bilirubin(without the albumin)is absorbed
through the hepatic cell membrane, mediated
by a carrier protein organic anion transport
organic anion transport
protein 2 (oatp2) .
protein 2 (oatp2) .
10.
Conjugation of bilirubin-
-80% of free bilirubin conugate with 2 Uridine
diphospho-glucuronic acid (UDPGA) catalyzed
by the enzyme glucuronyl transferase in the
smooth ER, forming the compound Bilirubin
Diglucurnoide (the conjugated form of
bilirubin) that is water soluble
-20% of the rest bilirubin conjugate with
sulphate & other substances.
11.
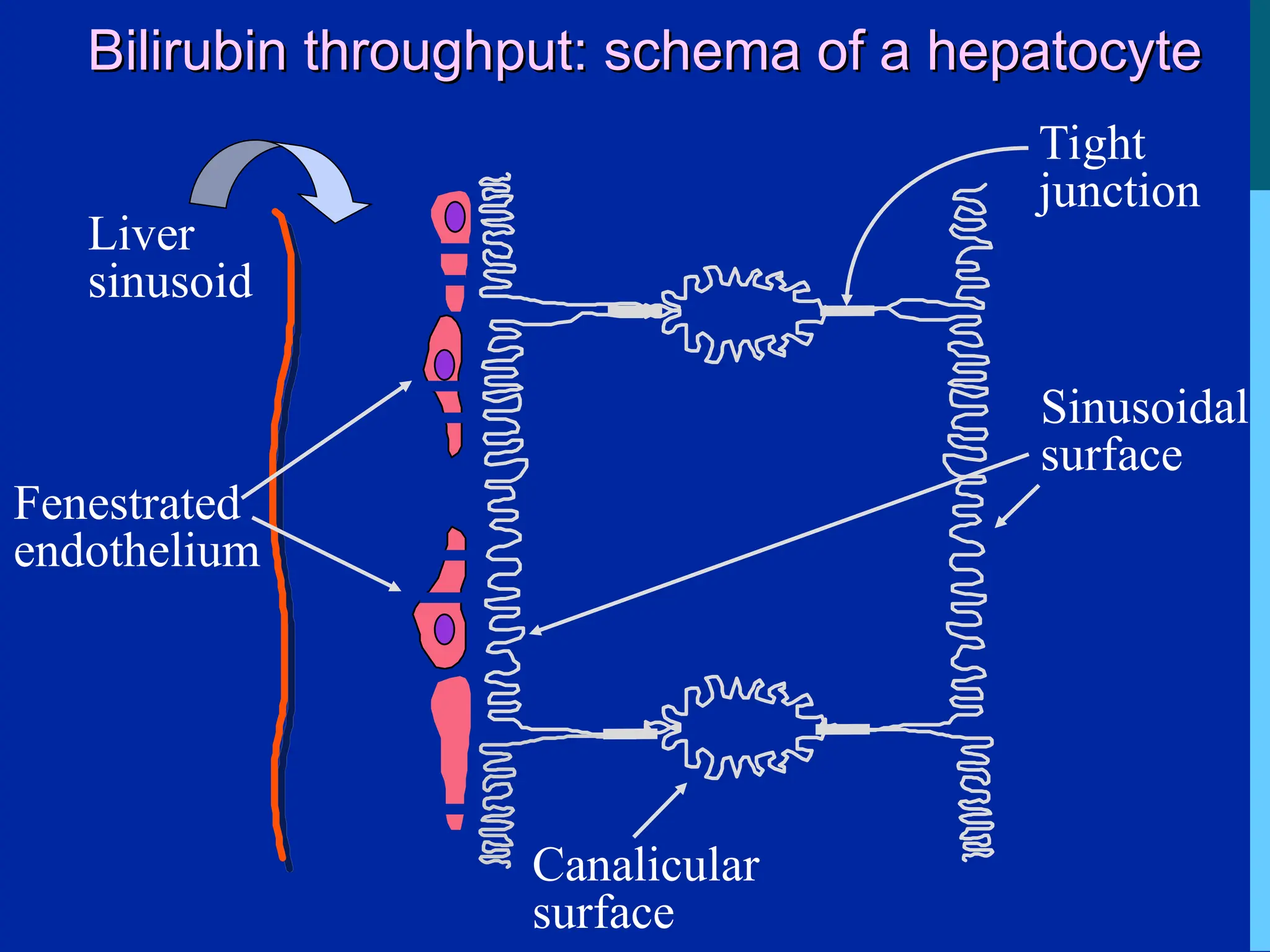
Bilirubin throughput: schemaof a hepatocyte
Bilirubin throughput: schema of a hepatocyte
Sinusoidal
surface
Canalicular
surface
Tight
junction
Liver
sinusoid
Fenestrated
endothelium
12.
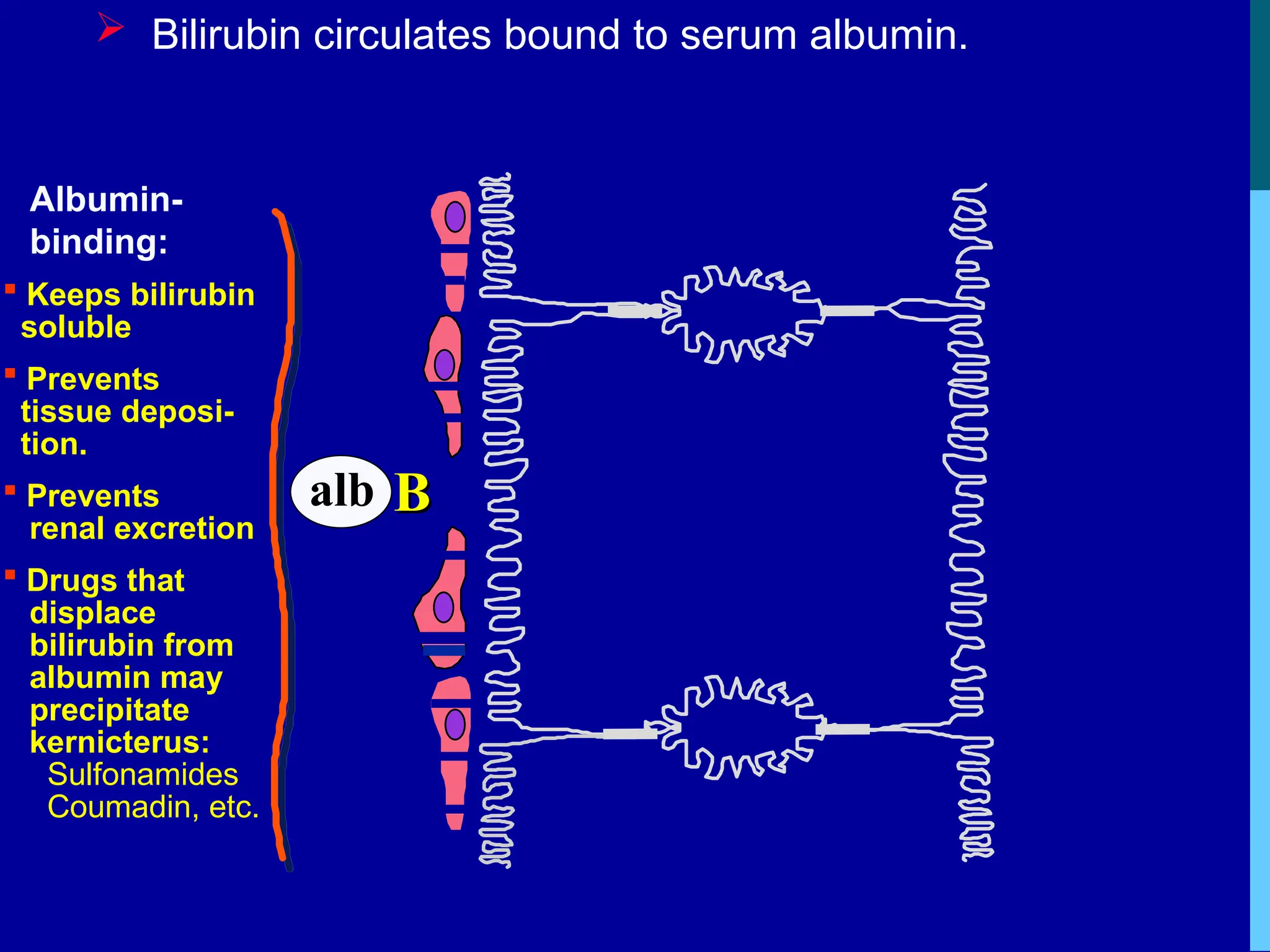
Bilirubin circulatesbound to serum albumin.
B
B
alb
Albumin-
binding:
Keeps bilirubin
soluble
Prevents
tissue deposi-
tion.
Prevents
renal excretion
Drugs that
displace
bilirubin from
albumin may
precipitate
kernicterus:
Sulfonamides
Coumadin, etc.
13.
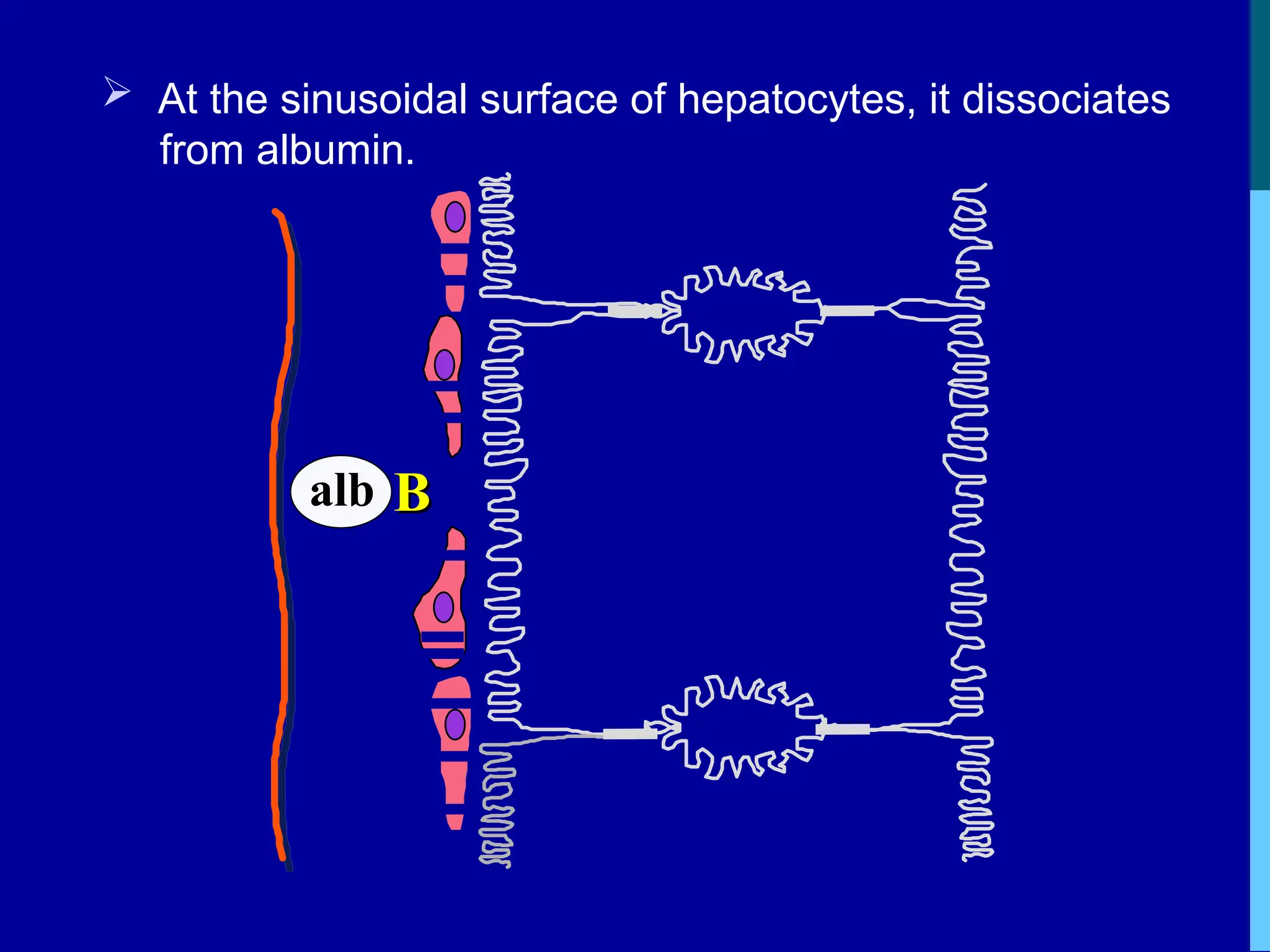
At thesinusoidal surface of hepatocytes, it dissociates
from albumin.
B
B
alb
14.
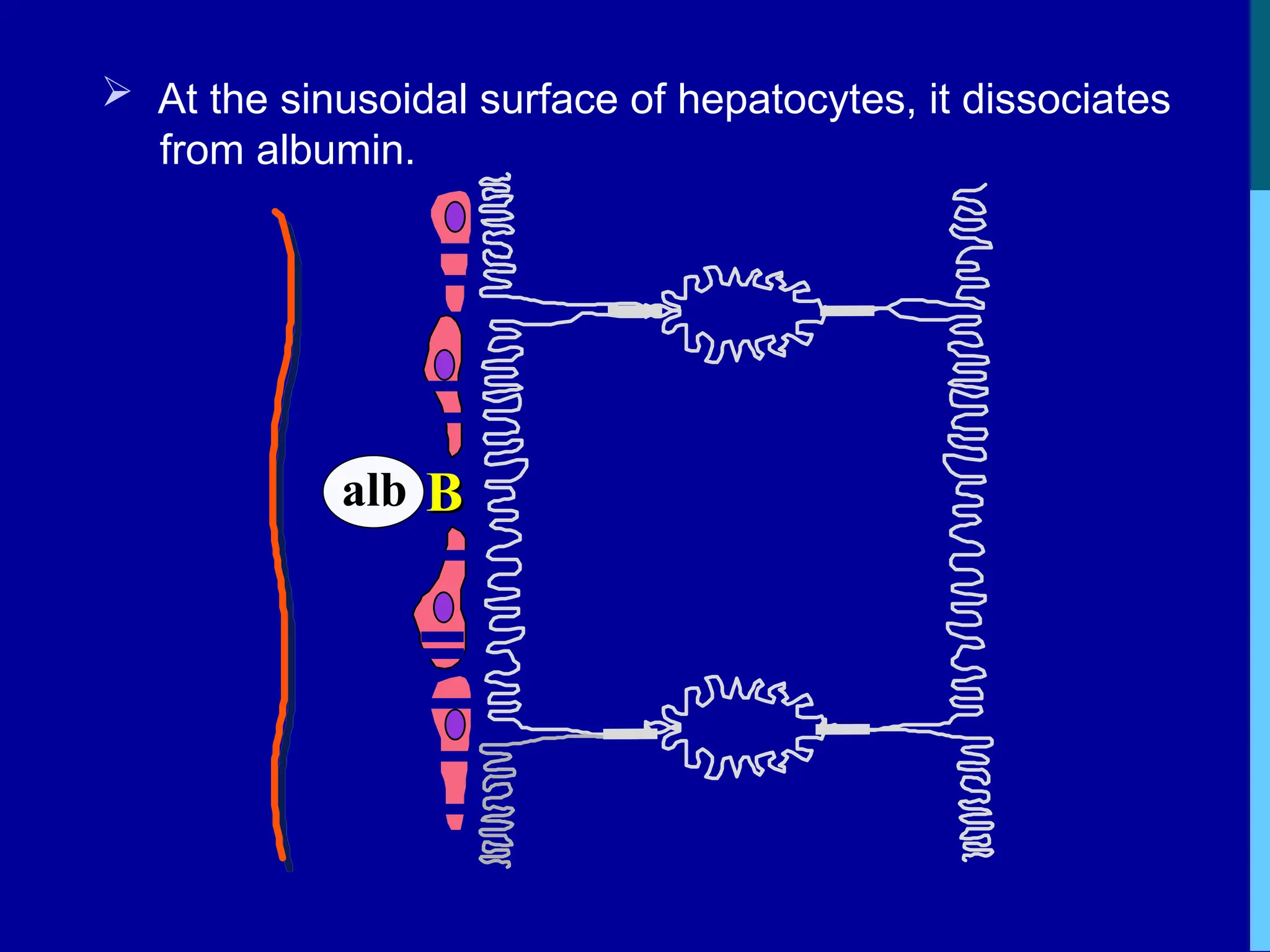
At thesinusoidal surface of hepatocytes, it dissociates
from albumin.
B
B
alb
15.
.
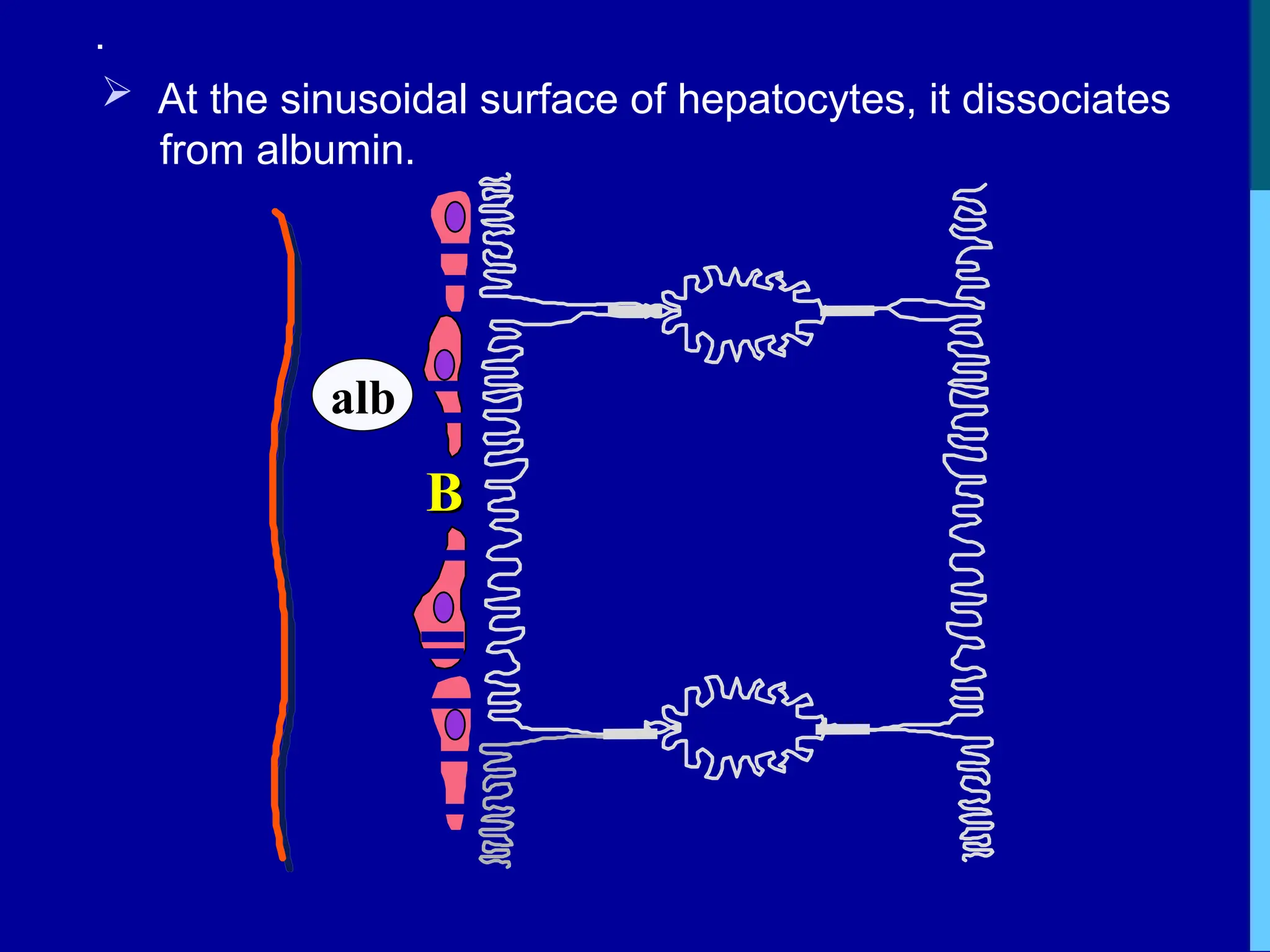
At thesinusoidal surface of hepatocytes, it dissociates
from albumin.
B
B
alb
16.
.
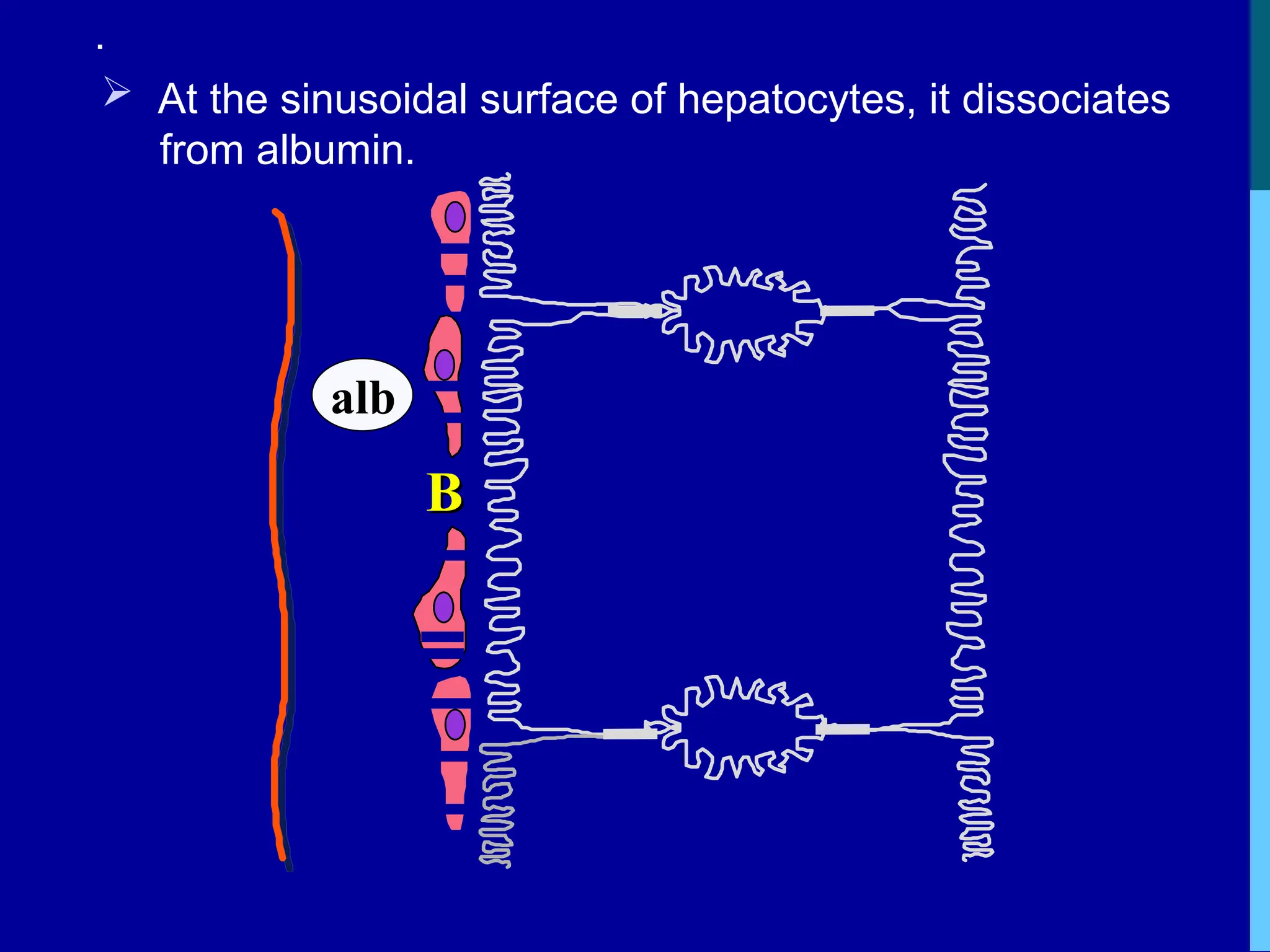
At thesinusoidal surface of hepatocytes, it dissociates
from albumin.
B
B
alb
17.
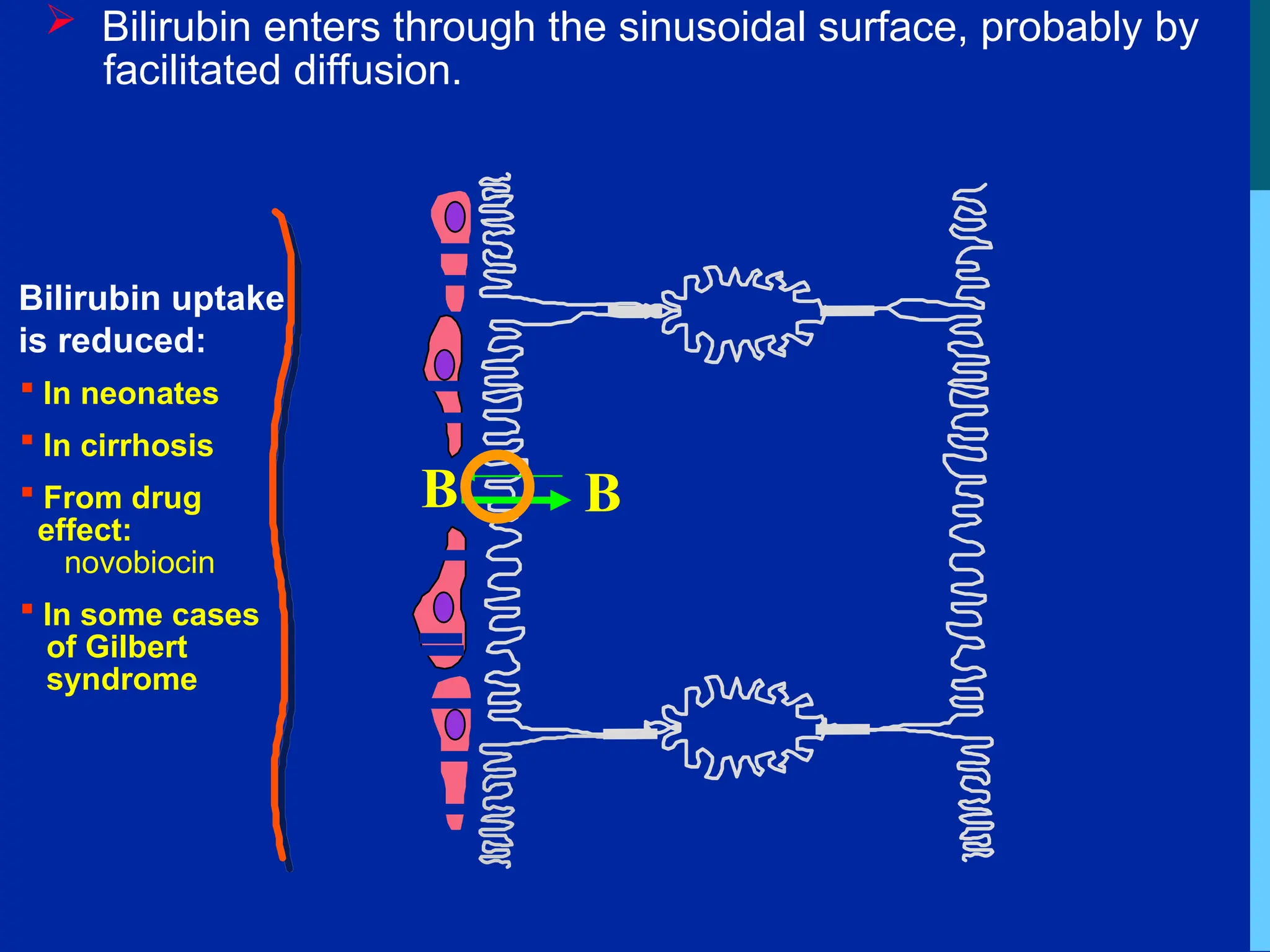
Bilirubin entersthrough the sinusoidal surface, probably by
facilitated diffusion.
B
B
Bilirubin uptake
is reduced:
In neonates
In cirrhosis
From drug
effect:
novobiocin
In some cases
of Gilbert
syndrome
18.
B
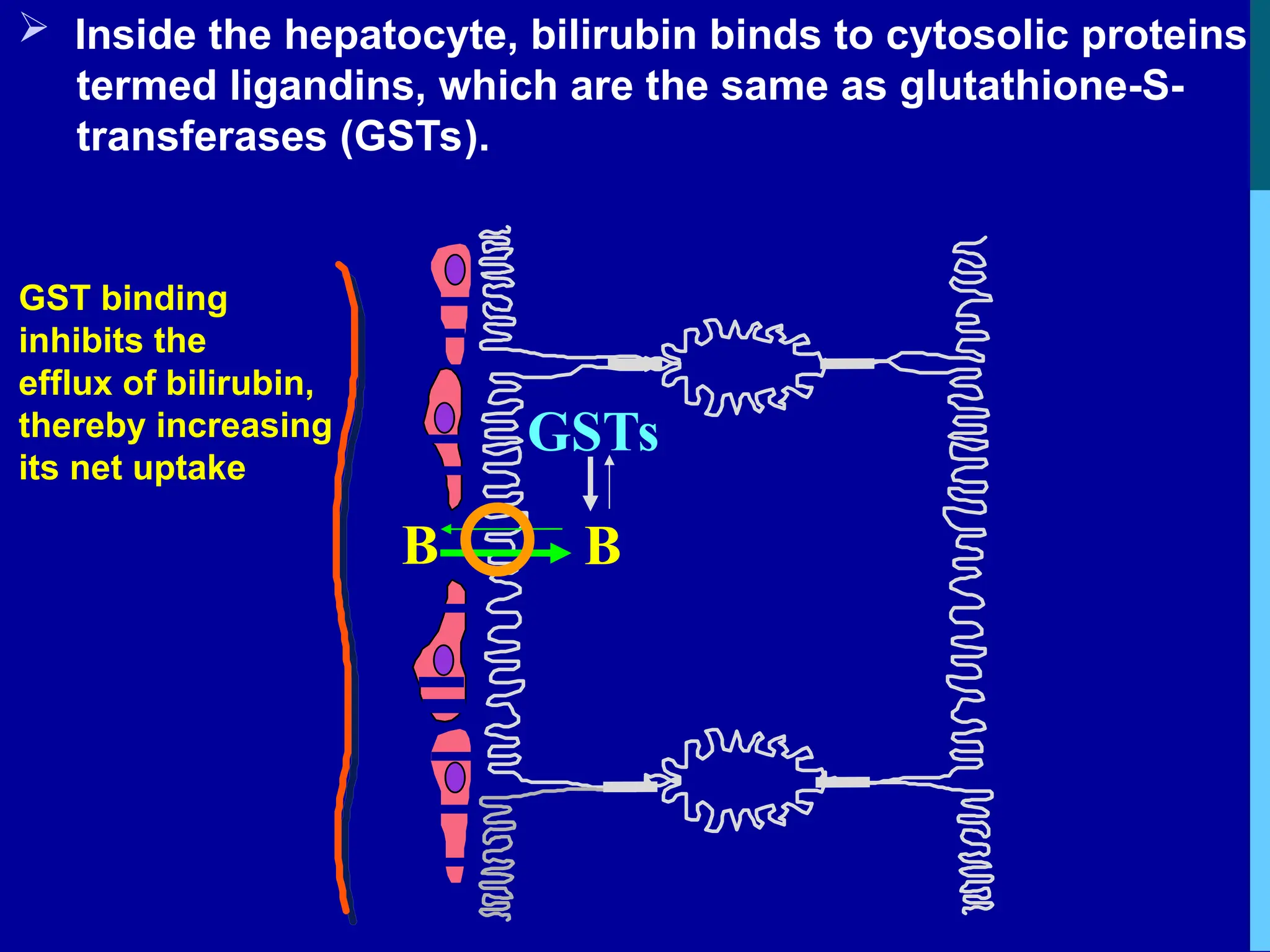
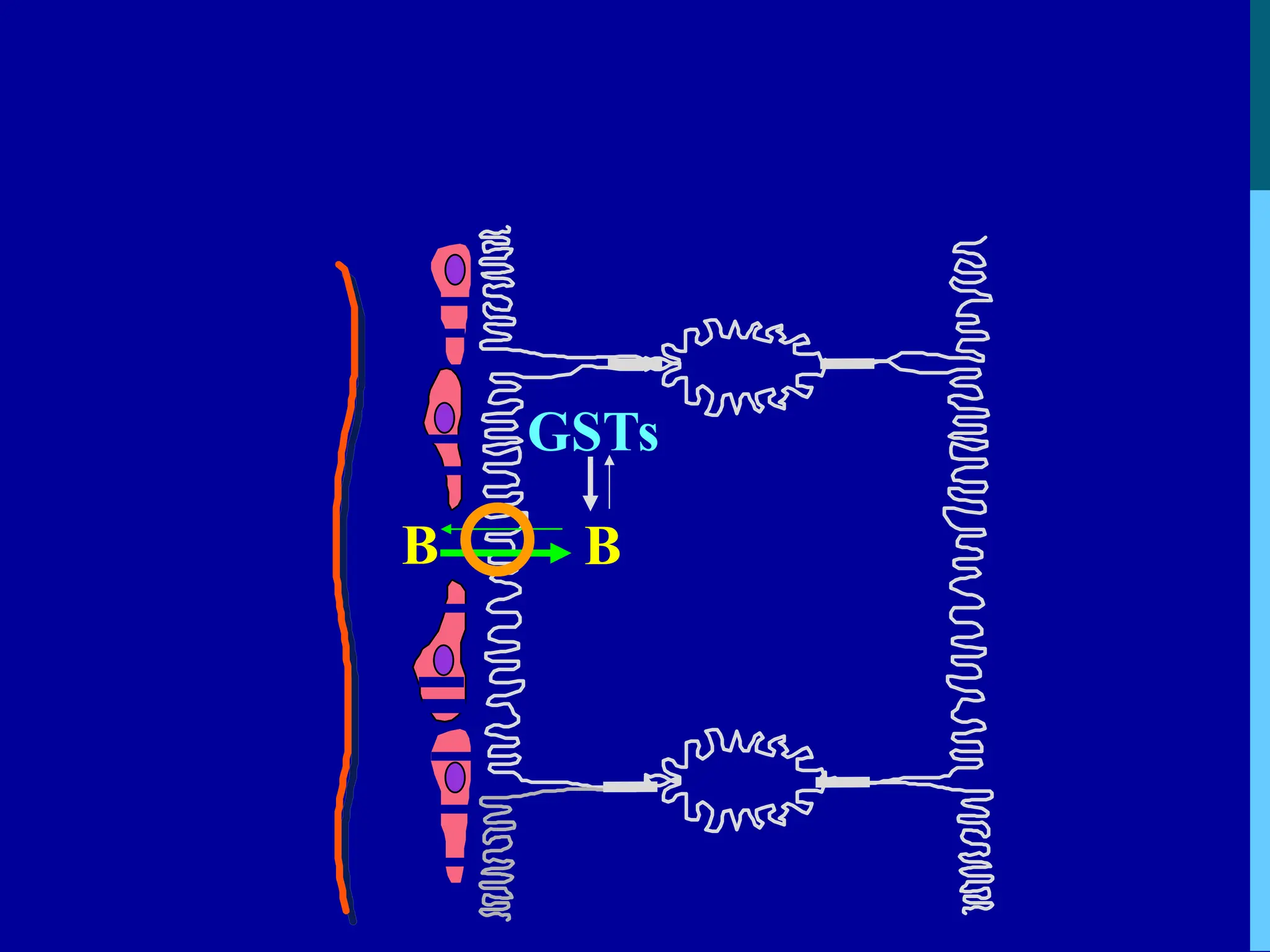
Inside thehepatocyte, bilirubin binds to cytosolic proteins
termed ligandins, which are the same as glutathione-S-
transferases (GSTs).
GSTs
B
GST binding
inhibits the
efflux of bilirubin,
thereby increasing
its net uptake
B
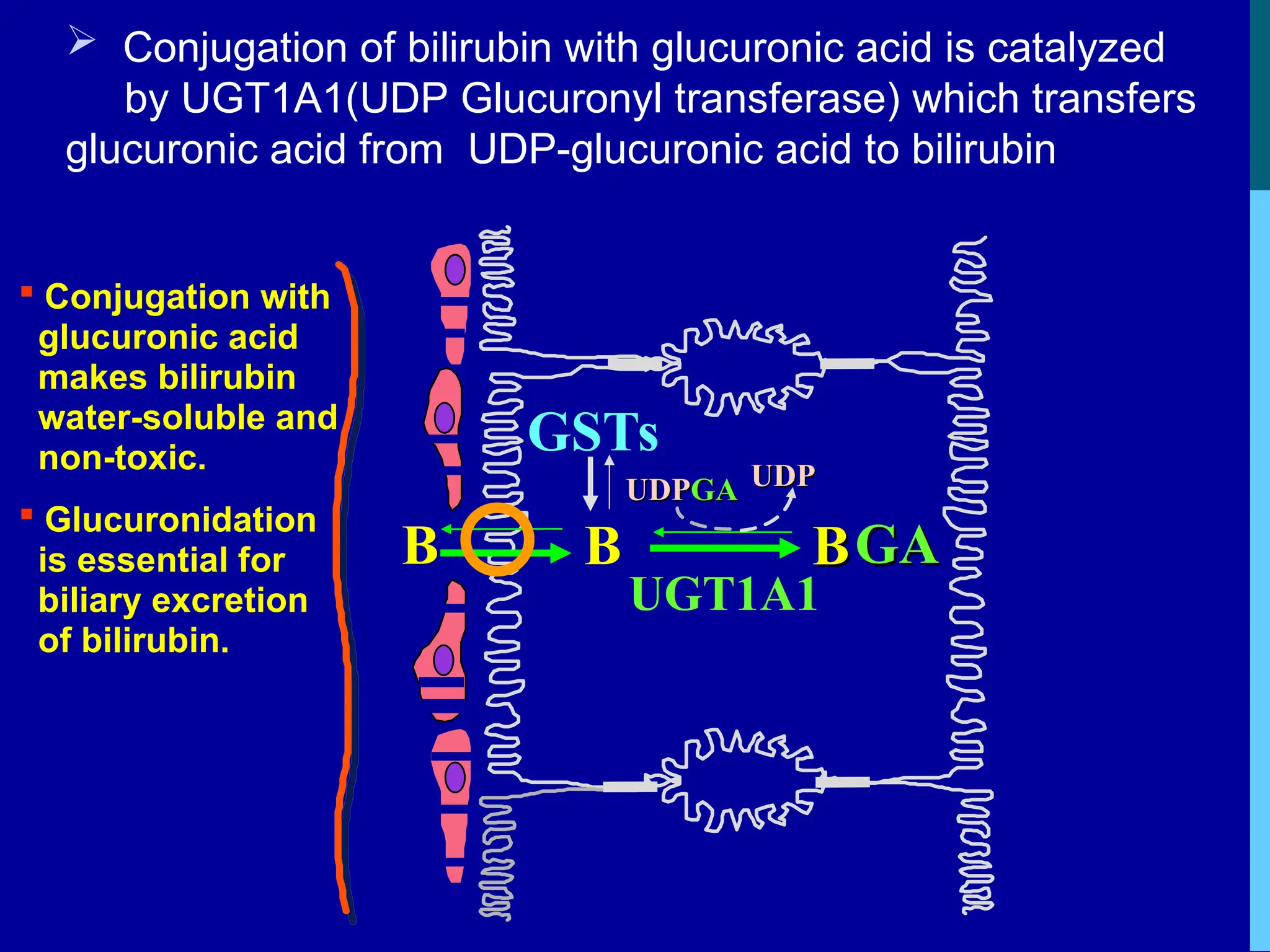
Conjugation ofbilirubin with glucuronic acid is catalyzed
by UGT1A1(UDP Glucuronyl transferase) which transfers
glucuronic acid from UDP-glucuronic acid to bilirubin
GSTs
UDP
UDPGA
GA UDP
UDP
B
BGA
GA
UGT1A1
B
Conjugation with
glucuronic acid
makes bilirubin
water-soluble and
non-toxic.
Glucuronidation
is essential for
biliary excretion
of bilirubin.
21.
Seceretion of conjugatedbilirubin
-“Cholebilirubin” in the bile
by liver hepatocytes is by active transport (which
needs energy)into bile canaliculi--- it’s a
rate limiting step, susceptible to impairment in liver
disease
-Color of bile is due to bilirubin
-Daily load of bilirubin: 250-300 mg in normal adults
22.
.
Conjugated” bilirubin iswater soluble.it is secreted
by the hepatocytes into the biliary canaliculi and
enters the gut
Converted to stercobilinogen (urobilinogen)
(colorless) by bacteria in the gut which is
excreted in feces-80% and
20% enters entero hepatic circulation ---enters
general circulation ----gets filtered in kidney and
excreted as urinary urobilinogen or re-excreted by
liver.
25.
HYPERBILIRUBINEMIA
Increased plasmaconcentrations of bilirubin (> 2 mg/dL)
occurs when
there is an imbalance between its production and excretion
Recognized clinically as jaundice
26.
Jaundice
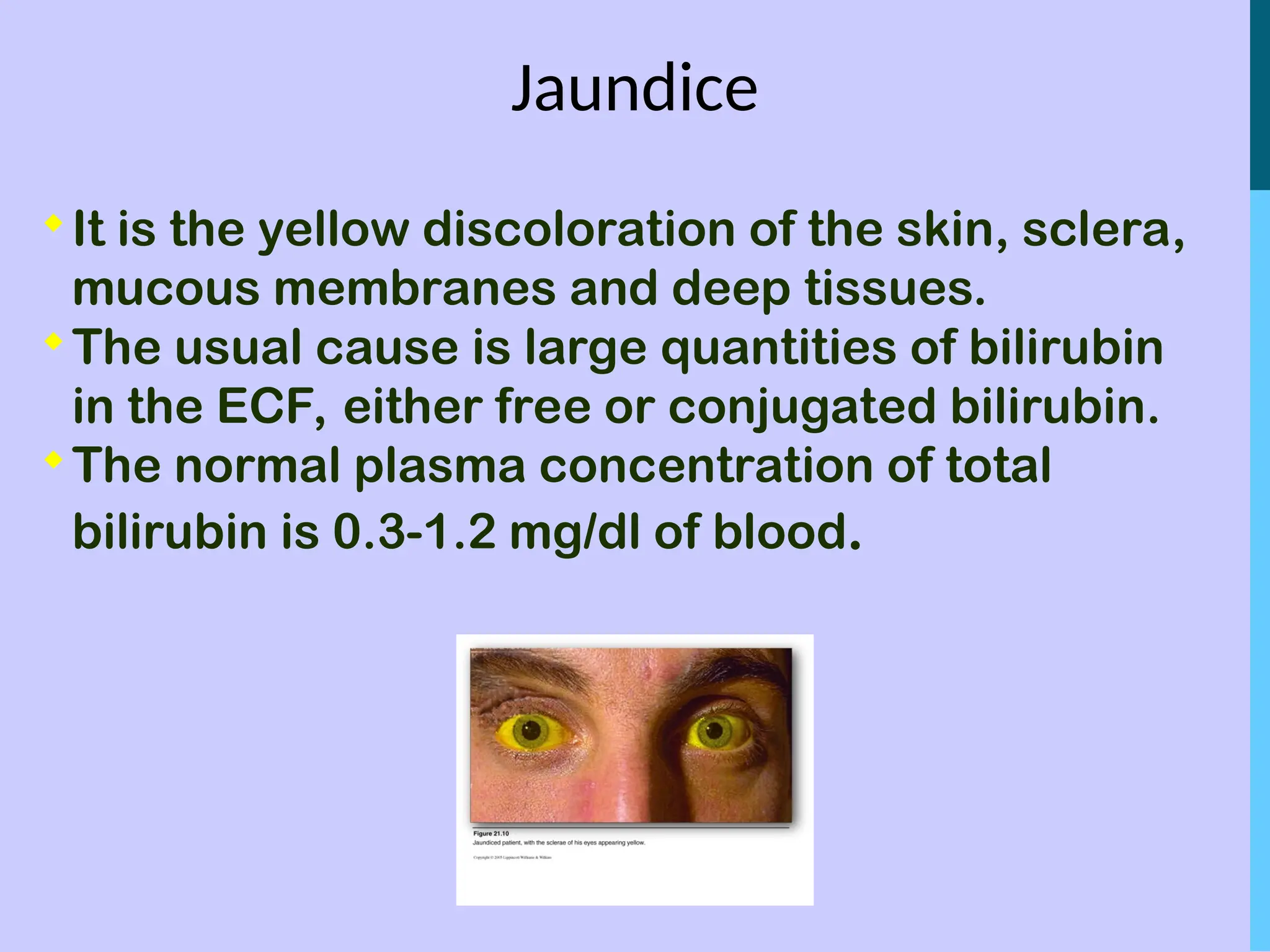
It is theyellow discoloration of the skin, sclera,
mucous membranes and deep tissues.
The usual cause is large quantities of bilirubin
in the ECF, either free or conjugated bilirubin.
The normal plasma concentration of total
bilirubin is 0.3-1.2 mg/dl of blood.
28.
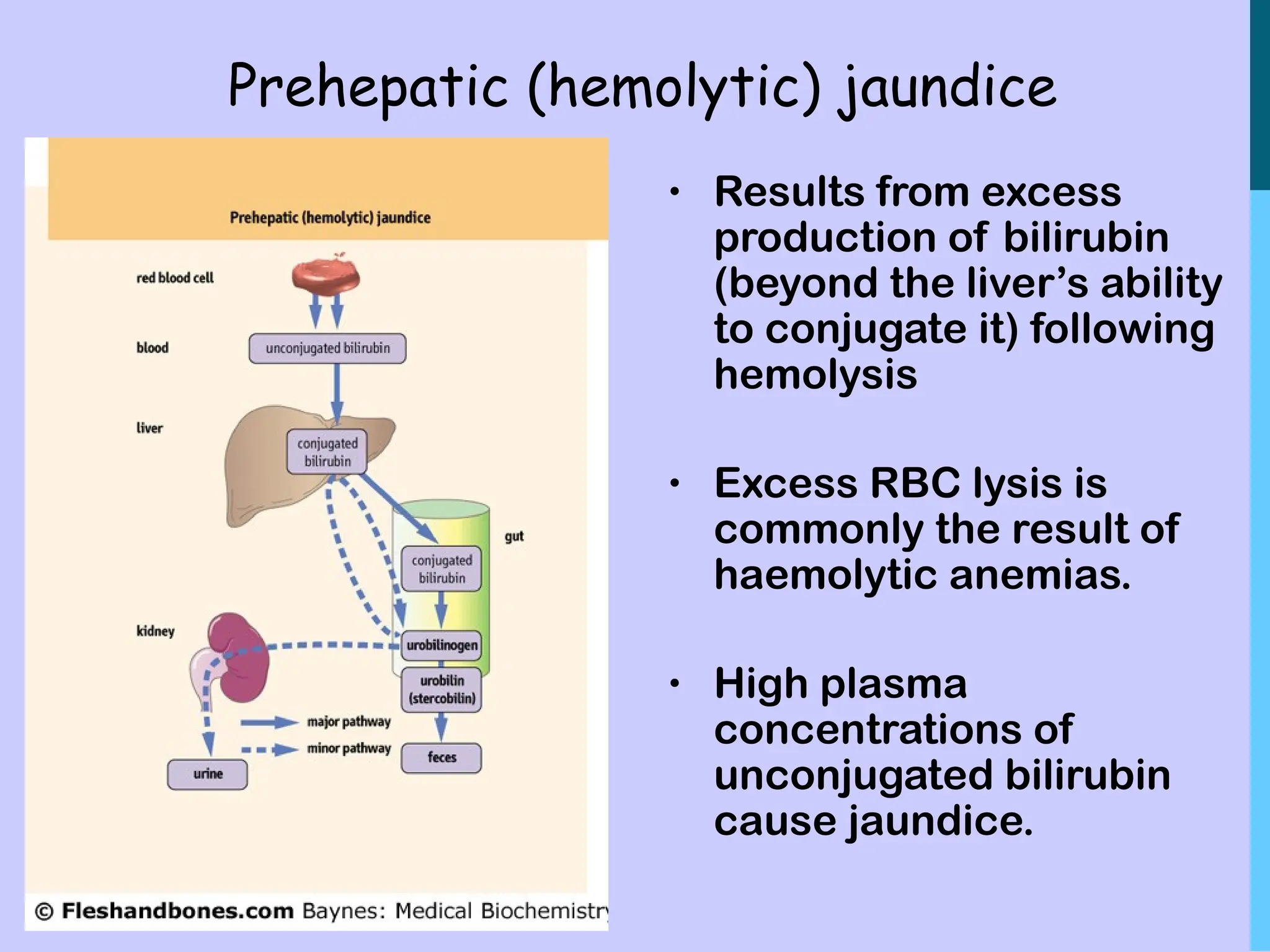
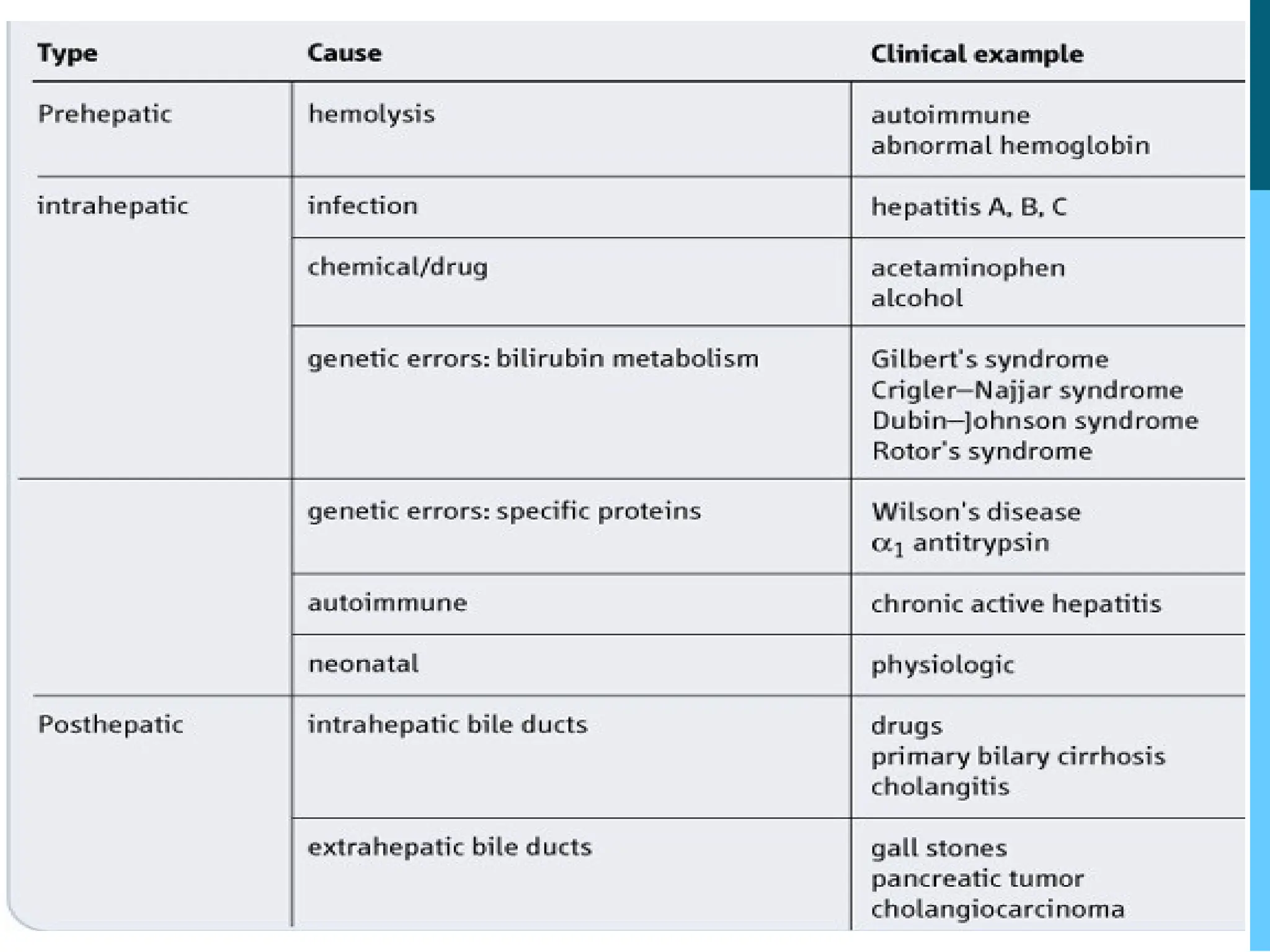
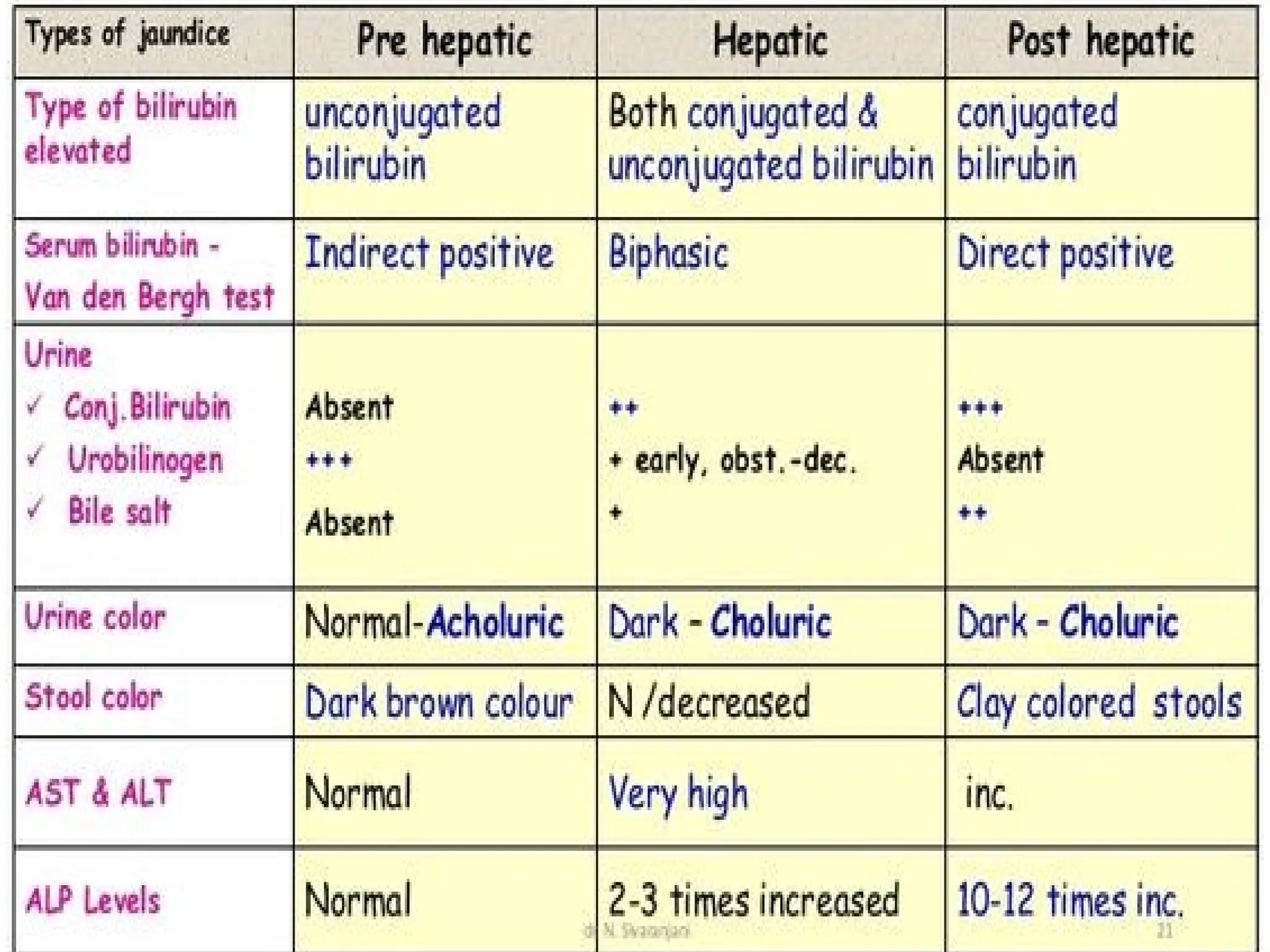
Prehepatic (hemolytic) jaundice
•Results from excess
production of bilirubin
(beyond the liver’s ability
to conjugate it) following
hemolysis
• Excess RBC lysis is
commonly the result of
haemolytic anemias.
• High plasma
concentrations of
unconjugated bilirubin
cause jaundice.
29.
Intrahepatic jaundice
• Inhepatocellular (or intrahepatic) jaundice, there
is dysfunction of the hepatic cells. The liver loses
the ability to conjugate bilirubin, but in cases
where it also may become cirrhotic,
it compresses the intra-hepatic portions of the
biliary tree to cause a degree of obstruction-
Impaired uptake, conjugation, and secretion of
bilirubin
• This leads to both unconjugated and
conjugated bilirubin in the blood,
accompanied by other abnormalities in
biochemical markers of liver function
30.
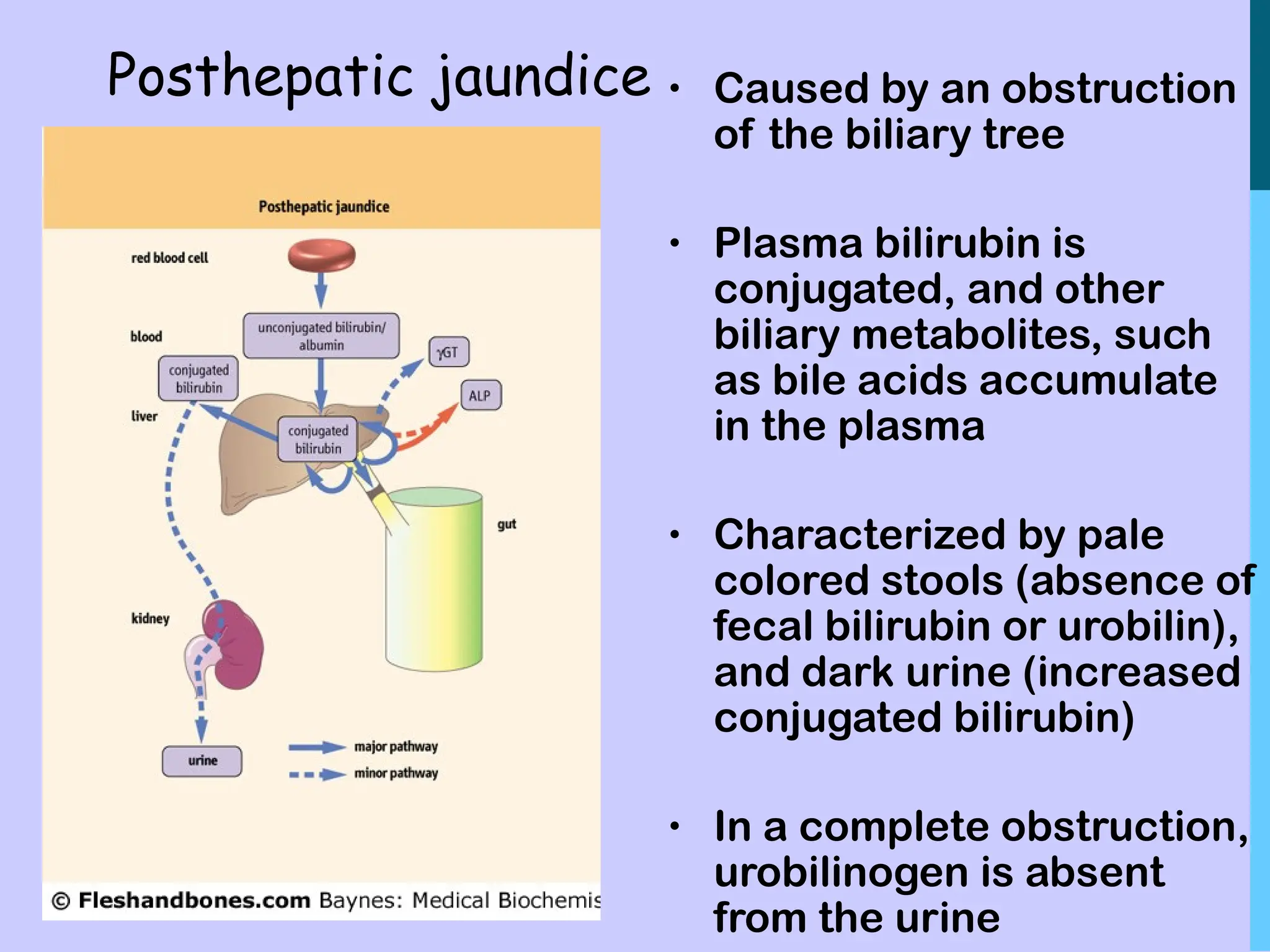
Posthepatic jaundice •Caused by an obstruction
of the biliary tree
• Plasma bilirubin is
conjugated, and other
biliary metabolites, such
as bile acids accumulate
in the plasma
• Characterized by pale
colored stools (absence of
fecal bilirubin or urobilin),
and dark urine (increased
conjugated bilirubin)
• In a complete obstruction,
urobilinogen is absent
from the urine
32.
TYPES OF BILIRUBININ SERUM
Direct bilirubin or“Conjugated”-is water soluble
and reacts rapidly with reagents.
Indirect bilirubin or Unconjugated-is lipid soluble
and reacts slowly with reagents.
Total bilirubin = Direct bilirubin + Indirect
bilirubin
Knowing level of each type of bilirubin has
diagnostic importance