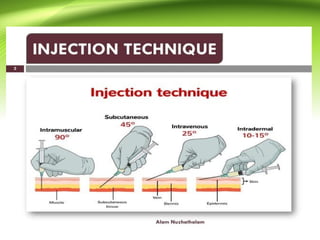
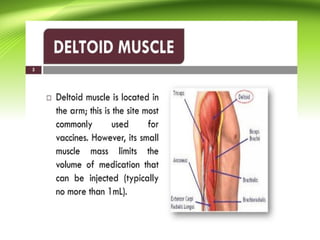
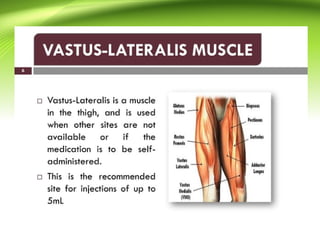
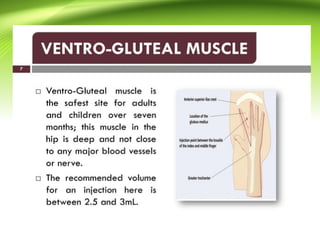
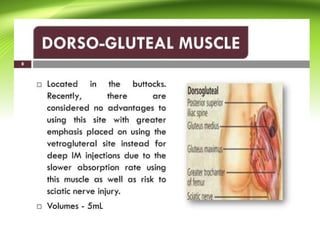
Intramuscular injection (IM) is installing medications into the depth of specifically selected muscles. The bulky muscles have good vascularity, and therefore the injected drug quickly reaches the systemic circulation and thereafter into the specific region of action, bypassing the first-pass metabolism. It is one of the most common medical procedures to be performed annually. This activity outlines and highlights the role of the interprofessional team in improving care for patients who undergo an intramuscular injection. This activity also summarizes the anatomic landmarks, safety precautionary checklists, the recommended procedural steps, and the complications to be aware of following the procedure. Objectives: Identify the safe anatomical landmarks for intramuscular injection. Describe the technique of intramuscular injections. Summarize the potential complications of intramuscular injection. Review interprofessional team strategies for improving care coordination and communication to advance intramuscular injection and improve outcomes. Access free multiple choice questions on this topic. Go to: Introduction Intramuscular injection (IM) is installing medications into the depth of specifically selected muscles.[1] The bulky muscles have good vascularity, and therefore the injected drug quickly reaches the systemic circulation and thereafter into the specific region of action, bypassing the first-pass metabolism.[2] It is one of the most common medical procedures to be performed annually.[3] However, there is still a lack of adherence to recommended guidelines and an algorithm for giving IM among health professionals worldwide.[2] Drugs may be given intramuscularly both for prophylactic (around 5% for immunization) as well as curative purposes (accounting for more than 95% of IM injections).[2] The most common medications given by IM route include: Antibiotics- penicillin G benzathine penicillin, streptomycin Biologicals- immunoglobins, vaccines, and toxoids Hormonal agents- testosterone, medroxyprogesterone[2] Any nonirritant and soluble drugs may be given IM during an emergency scenario. Go to: Anatomy and Physiology Anatomical Landmarks There are specific landmarks to be considered while giving IM injections to avoid any neurovascular complications. The specific landmarks for the most commonly used sites are discussed below. Dorsogluteal Region 5 to 7.5 cm below the iliac crest Upper outer quadrant within the buttocks[4] Ventrogluteal Region The heel of the opposing hand is placed in the greater trochanter, the index finger in the anterior superior iliac spine, and the middle finger below the iliac crest - the drug is injected into the triangle formed by the index, middle finger, and the iliac crest Deltoid 2.5 to 5 cm below the acromion process Vastus Lateralis The middle third of the line joining the greater trochanter of the femur and the lateral femoral condyle of the knee