Introduction
Influenza virus isonly member of orthomyxovirus family
It is different from paramyxoviruses primarily in that the former have a segmented RNA genome
(usually 8 pieces), whereas the RNA genome of latter consists of a single piece
The term myxo refers to the observations that these viruses interact with mucins ( glycoproteins
on the surfaces of cells)
It causes influenza commonly called the flu. It also infects the respiratory tract of many birds,
animals and humans
3.
Important properties
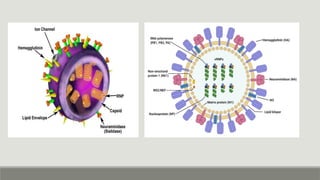
Segmented single-strandedRNA genome
Helical nuclear capsid
Outer lipoprotein envelope
Has RNA-dependent RNA polymerase that transcribes negative-polarity genome into mRNA
Two different types of spikes that act as antigens and also contributes in the different
antigenically strains depending upon the type of the antigens
These spikes or antigens are haemagglutinins and neuraminidase
5.
Types
Three distinct types
1.Influenza A
2. Influenza B
3. Influenza C
Depending upon antigens HA and NA
There are 16 antigenically distinct types of hemagglutinin
And 9 antigenically distinct types of neuraminidase
Replicative cycle
Viral hemagglutinininteracts with sialic acid receptors on the cell surface and virus absorbs to the cell
It enters in vesicles and uncoats within an endosome (facilitated by low pH within endosome
M2 protein form ion channel in virion to pass protons
This disrupts the envelope and frees the nucleocapsid to enter in cytoplasm and migrates to nucleus for
RAN transcribtion
Viral RNA polymerase transcribes genome into mRNA
Host nucleus contains methylated guanosine cap and it requires it
This is called “cap snatching”. It acts as primar. Capped viral mRNA then move to cytoplasm for translation
Proteins are formed in cytoplasm such as NA protein, matrix protein etc.
Assembly occurs and it releases from the host cell by budding
8.
Transmission & epidemiology
Thevirus is transmitted by airborne droplets
The ability of influenza A virus to cause epidemics is dependent upon antigenic changes in the
hemagglutinin and neuraminidase
Antigenic shifts variants appear infrequently, whereas antigenic drifts variants appear every year
The last major antigenic shift that caused a pandemic in humans was in 1968 when H3N2 emerged.
Influenza B virus only undergoes antigenic drift. Its antigenic changes are less dramatic and less
frequent then influenza A virus
It occurs usually between the months of December to February
Morbidity is very high in children younger tan 2 years
9.
Pathogenesis
The hemagglutinin bindsto cell surface receptors (sialic acid) to initiate infection of the cell
The neuraminidase cleaves the neuraminic acid to release progeny from the cell
It aldo degrades the protective layer of mucus in the respiratory tract which enhance the ability of
virus to invade respiratory epithelial cells
There are two types of antigenic changes:
•Antigenic shift (major change based on reassortment of segments of genome RNA)
•Antigenic drift (minor change based on mutation in genome RNA)
Matrix proteins:
•M1 protein (provides structural integrity)
•M2 protein (forms ion channel b/w interior of virus and the external milieu
10.
They have bothgroup-specific and type-specific antigens
Internal ribonucleoprotein in nucleocapsid is group-specific antigen hat distinguishes influenza
A, B, and C viruses
Hemagglutinin and neuraminidase are type-specific antigens located on the surface
Influenza virus causes inflammation of mucosa of upper respiratory tract sites i.e. nose and
pharynx and lower tract i.e. larynx, trachea and bronchi
Infection is limited to this area because the protease that cleaves hemagglutinin are located in
the respiratory tract
The systemic symptoms such as severe myalgias, are due to cytokines circulating in the blood
There is necrosis of superficial layer of the respiratory epithelium
11.
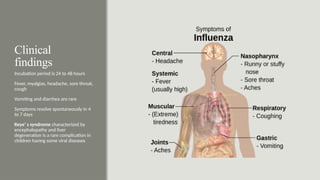
Clinical
findings
Incubation period is24 to 48 hours
Fever, myalgias, headache, sore throat,
cough
Vomiting and diarrhea are rare
Symptoms resolve spontaneously in 4
to 7 days
Reye’ s syndrome characterized by
encephalopathy and liver
degeneration is a rare complication in
children having some viral diseases
12.
Laboratory diagnosis
Polymerase chainreaction (PCR) for the detection of viral RNA
NAAT (nucleic acid amplification test) highly specific diagnoses influenza A and B
Enzyme-linked immunosorbent assay (ELISA) for viral proteins
FLU OIA and Quick Vue influenza test are based on detection of viral antigens using monoclonal antibodies
Third test (ZstatFlu) is based on detection of viral neuraminidase using a substrate of the enzyme that
changes color when cleaved by neuraminidase
Also diagnose by the presence of antibodies in patient’serum
Haemagglutination inhibition test
Complement fixation test
Direct fluorescent antibody
13.
Treatment
Neuraminidase inhibitors likeoseltivir (orally), zanamivir (inhaling), and peramivir
(intravenously)
Boloxavir inhibits endonuclease (cap snatching)
Amantadine (symmetrel) both for treatment and prevention but H3N2 are resistant to this, this
blocks the M2 protein ion channel
14.
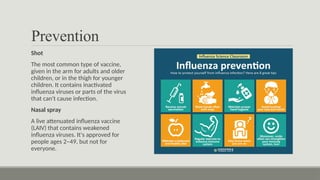
Prevention
Shot
The most commontype of vaccine,
given in the arm for adults and older
children, or in the thigh for younger
children. It contains inactivated
influenza viruses or parts of the virus
that can't cause infection.
Nasal spray
A live attenuated influenza vaccine
(LAIV) that contains weakened
influenza viruses. It's approved for
people ages 2–49, but not for
everyone.