HYPERTENSION
Lecture for CI students
Senbeta Guteta (MD, MPH, Consultant Internist &Cardiologist)
Associate Professor, Division of Cardiology, Department of Internal Medicine,
AAU, Jan 2023
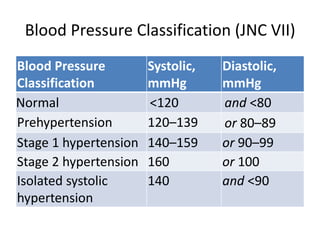
Definition of Hypertension
•A chronic medical condition in which BP is elevated
• Clinical definition: that level of BP at which
institution of therapy reduces BP–related morbidity
and mortality.
– based on the average of > 2 seated BP readings during
each of > 2 outpatient visits.
• Persistently elevated, systolic and/or diastolic blood
pressure of 140/90 mmHg or more in subjects aged
18 years and above.
5.
Epidemiology of HTN
•Global: ~22% of adults (2014)
• Sub Saharan Africa
• 40% (Highest prevalence).
• Patients are younger, more aggressive HTN, present late
and with complications.
• Ethiopia
• 20-30 % prevalence of raised BP (most studies, more
urban)
• National NCD STEPS survey (> 10,000 participants from all
regions): 16% prevalence of raised BP (men 15.7%,
women 16.5%)
6.
• Prevalence varieswith Age, Race, Education, Diet and
other factors
• Likelihood of hypertension increases with age
– >= 60 years age: prevalence is 65.4%.
• Both environmental and genetic factors may contribute
to regional & racial variations in BP & HTN prevalence
Epidemiology cont….
7.
Impact of hypertension
•9.4 million deaths in 2010 (from 17 million global CVD
deaths)
• Main driver of Cardiovascular Disease
• Kills twice as many women aged 60 and above in LMIC
compared to developed countries.
• Accounts for loss of 57 million disability adjusted life
years (DALYS).
• For every increase in 20 mmHg SBP or 10 mmHg DBP,
lifetime risk of heart disease DOUBLES.
• Hypertensive Heart Disease(HHD) is the second most
common CVD in major referral hospitals of Ethiopia.
8.
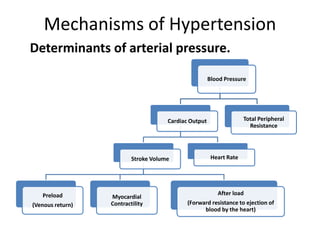
Mechanisms of Hypertension
Determinantsof arterial pressure.
Blood Pressure
Cardiac Output
Stroke Volume
Preload
(Venous return)
Myocardial
Contractility
After load
(Forward resistance to ejection of
blood by the heart)
Heart Rate
Total Peripheral
Resistance
9.
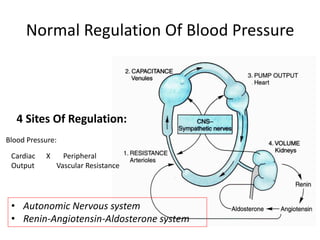
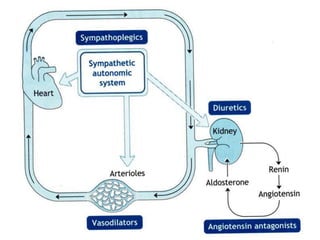
Normal Regulation OfBlood Pressure
4 Sites Of Regulation:
Blood Pressure:
Cardiac X Peripheral
Output Vascular Resistance
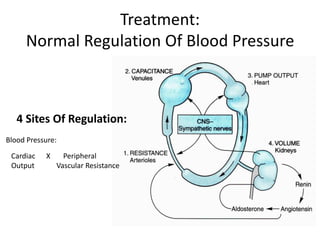
• Autonomic Nervous system
• Renin-Angiotensin-Aldosterone system
10.
Pathogenesis of Hypertension
•Cause of HTN is unknown in more than 90% of cases.
– But several factors can increase risk of developing HTN
• Where there is no specific cause, it is referred to as primary
or essential hypertension.
• Essential hypertension tends to develop gradually over many
years.
11.
Pathogenesis of HTN….
•A specific cause found in ~ 5% of adults = secondary HTN
• Secondary HTN tends to appear suddenly and causes higher
BP than does primary hypertension.
• Causes of secondary HTN:
– Renal diseases
• Renal vascular; renal parenchymal; polycystic kidneys
– Adrenal disease
• Pheochromocytoma, Cushing’s and Conn’s syndromes, 11-
alpha-hydroxylase, 17 hydroxylase deficiency
12.
Pathogenesis of HTN…
OtherCauses of secondary hypertension:
– Thyroid (Hyper-and hypothyroidism)
– Coarctation of the aorta.
– Obstructive sleep apnoea
– Drugs: steroids; birth control pills; sympathomimetic drugs (eg.
Some cough remedies), cocaine, methamphetamine
13.
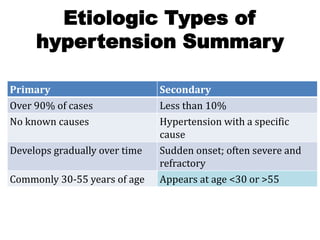
Etiologic Types of
hypertensionSummary
Primary Secondary
Over 90% of cases Less than 10%
No known causes Hypertension with a specific
cause
Develops gradually over time Sudden onset; often severe and
refractory
Commonly 30-55 years of age Appears at age <30 or >55
14.
Risk factors forHypertension
= Conditions which increase likelihood of developing HTN but
are not underlying causes.
Commonly identified risk factors for hypertension:
• Age: risk of hypertension increases with age
– More common in male through early middle age, or about age
45 years
– Women are more likely to have hypertension after age 55
• Race. Common among blacks, often developing at earlier age
– Serious complications, such as stroke, heart attack, and kidney
failure, also more common in blacks
15.
Risk factors forHypertension….
• Family history: HTN tends to run in families.
• Overweight or obesity: increased risk of HTN
• Physical inactivity.
– Lack of physical activity increases risk of HTN & overweight
16.
Risk factors forHypertension….
• Tobacco use
– Both active and passive smoking increase risk of hypertension
– Chemicals in tobacco can also damage lining of artery walls
• High dietary salt (sodium) consumption
17.
Risk factors forHypertension…..
• High/chronic alcohol consumption
• Stress
– High levels of stress can lead to a temporary increase in BP
– Stress related factors like eating more,
using tobacco or drinking alcohol
may increase risk
• Chronic medical conditions: Eg. kidney disease, sleep
apnea
18.
Etiologies
1. Essential orPrimary or idiopathic
hypertension: ~80–95%
2. Secondary hypertension: 5–20%
– a specific underlying disorder causing the
elevation of blood pressure can be identified
19.
What are thepathologic consequences
(complications) of hypertension?
20.
Pathologic Consequences …..Heart
• Heart disease is the most common cause of
death in hypertensive patients.
• Hypertensive heart disease
– Result of structural and functional adaptations
leading to:
• Left ventricular hypertrophy
• CHF
• Abnormalities of blood flow due to atherosclerotic
coronary artery disease and microvascular disease, and
• Cardiac arrhythmias (eg. Atrial fibrillation).
21.
Pathologic Consequences …..Brain
• Stroke
– 2nd most frequent cause of death in the world (5
million deaths each year)
– Additional 15 million persons with nonfatal strokes
– Elevated BP is the strongest risk factor for stroke.
– Incidence rises progressively with increasing BP levels,
particularly SBP in individuals >65 years
– Treatment of HTN decreases incidence of both
ischemic and hemorrhagic strokes.
• Impaired cognition and dementia in an aging
population
22.
Pathologic Conseq …..Brain
• Malignant hypertension
– encephalopathy : related to failure of autoregulation
of cerebral blood flow at the upper pressure limit,
resulting in vasodilation and hyperperfusion
– Signs and symptoms: severe headache, nausea and
vomiting (often of a projectile nature), focal
neurologic signs, and alterations in mental status.
– If Untreated, may progress to stupor, coma, seizures,
and death within hours
23.
Pathologic Conseq …..Kidney
• Kidney is both a target and a cause of hypertension.
• Primary renal disease is most common etiology of 2ry HTN
• Hypertension is a risk factor for renal injury & ESRD
– Renal risk appears to be more closely related to systolic than
to diastolic blood pressure
– Black men are at greater risk than white men for developing
ESRD at every level of BP
24.
Pathologic Conseq….. PeripheralArteries
• Blood vessels may be a target organ for
atherosclerotic disease 2ry to long-standing elevated
BP (in addition to contributing to pathogenesis of
hypertension)
• C/F of PAD:
– Asymptomatic
– Intermittent claudication (classic symptom): aching pain in
the calves or buttocks while walking that is relieved by rest.
25.
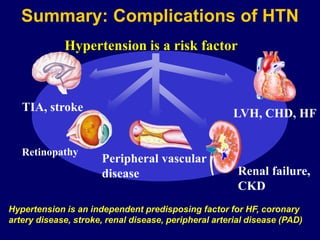
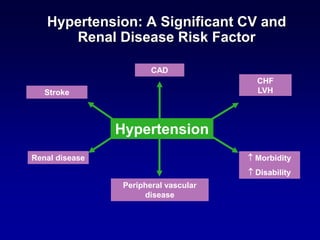
Renal failure,
CKD
Peripheral vascular
disease
Summary:Complications of HTN
LVH, CHD, HF
TIA, stroke
Hypertension is a risk factor
Hypertension is an independent predisposing factor for HF, coronary
artery disease, stroke, renal disease, peripheral arterial disease (PAD)
26.
Approach to thePatient: Hypertension
• Initial assessment: a complete history and
physical examination to:
– Confirm a diagnosis of hypertension,
– Screen for other CV disease risk factors
– Screen for 2ry causes of HTN
– Identify CV consequences of HTN & other
comorbidities
– Assess BP–related lifestyles, and
– Determine potential for intervention
27.
Approach….
• History
– Durationof HTN
– Previous therapies: responses and side effects
– Family history of hypertension and cardiovascular disease
– Dietary and psychosocial history
– Other risk factors: weight change, dyslipidemia, smoking,
diabetes, physical inactivity
– Evidence of 2ry HTN
• History of renal disease; change in appearance; muscle
weakness; spells of sweating, palpitations, tremor; erratic
sleep, snoring, daytime somnolence; symptoms of hypo- or
hyperthyroidism; use of agents that may increase BP
– Evidence of TOD: history of TIA, stroke, transient blindness;
angina, MI, CHF; sexual function, Other comorbidities
Approach…..
• Physical Examination
–Body habitus,: Wt, Ht
– BP
• both arms
• Supine, sitting, and standing positions to evaluate for
postural hypotension.
• BP at least once in lower extremity in patients in whom
HTN is discovered before age 30
– Heart rate
– Neck: thyroid gland, & signs of hypo- &
hyperthyroidism
30.
Approach…..
• Physical Examination
–Blood vessels : peripheral vessels, funduscopic
examination,
– Heart:
• Loud S2 due to closure of aortic valve
• S4 gallop attributed to atrial contraction against a
noncompliant LV
• LVH: enlarged, sustained & laterally displaced apical impulse
– Abdomen:
• bruit (particularly that lateralizes & extends throughout
systole into diastole) : renovascular hypertension
• Kidneys of patients with PKD may be palpable
– Evaluation for signs of CHF & neurologic examination.
Blood pressure measurement(Digital)
Measurement of Blood Pressure
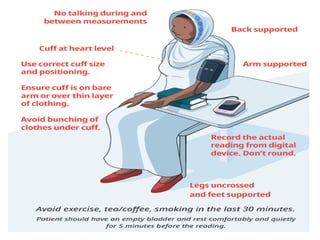
• Patient should sit quietly for 5 minutes before measurement
• Use correct size cuff and bladder
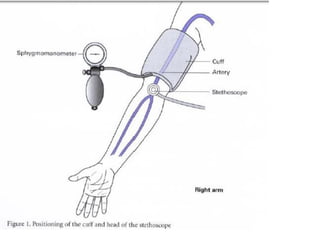
• Measure BP while patient is sitting on a chair with back support
and with arm supported at level of heart. Patient’s arm must be
relaxed.
• Take 2 measurements at least 1-2 minutes apart
• BP in both arms should be measured at first visit and the arm
with the highest BP should be used for future measurements
• Elderly, diabetics and other patients complaining of symptoms
suggestive of postural hypotension (e.g. dizziness, unsteadiness
or fainting when changing posture) should also have their BP
measured while standing: to compare with sitting BP.
33.
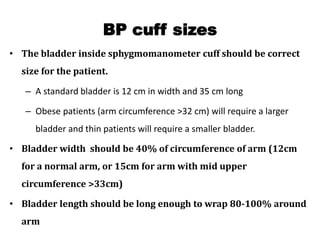
BP cuff sizes
•The bladder inside sphygmomanometer cuff should be correct
size for the patient.
– A standard bladder is 12 cm in width and 35 cm long
– Obese patients (arm circumference >32 cm) will require a larger
bladder and thin patients will require a smaller bladder.
• Bladder width should be 40% of circumference of arm (12cm
for a normal arm, or 15cm for arm with mid upper
circumference >33cm)
• Bladder length should be long enough to wrap 80-100% around
arm
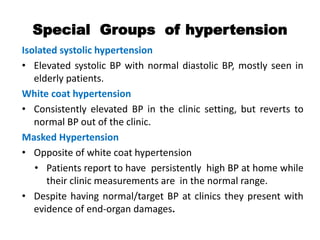
Special Groups ofhypertension
Isolated systolic hypertension
• Elevated systolic BP with normal diastolic BP, mostly seen in
elderly patients.
White coat hypertension
• Consistently elevated BP in the clinic setting, but reverts to
normal BP out of the clinic.
Masked Hypertension
• Opposite of white coat hypertension
• Patients report to have persistently high BP at home while
their clinic measurements are in the normal range.
• Despite having normal/target BP at clinics they present with
evidence of end-organ damages.
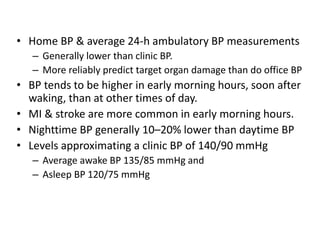
40.
• Home BP& average 24-h ambulatory BP measurements
– Generally lower than clinic BP.
– More reliably predict target organ damage than do office BP
• BP tends to be higher in early morning hours, soon after
waking, than at other times of day.
• MI & stroke are more common in early morning hours.
• Nighttime BP generally 10–20% lower than daytime BP
• Levels approximating a clinic BP of 140/90 mmHg
– Average awake BP 135/85 mmHg and
– Asleep BP 120/75 mmHg
41.
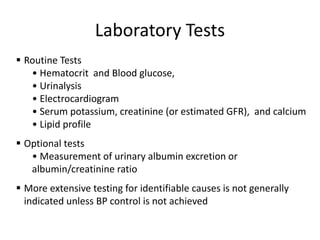
Laboratory Tests
▪ RoutineTests
• Hematocrit and Blood glucose,
• Urinalysis
• Electrocardiogram
• Serum potassium, creatinine (or estimated GFR), and calcium
• Lipid profile
▪ Optional tests
• Measurement of urinary albumin excretion or
albumin/creatinine ratio
▪ More extensive testing for identifiable causes is not generally
indicated unless BP control is not achieved
42.
Treatment:
Normal Regulation OfBlood Pressure
4 Sites Of Regulation:
Blood Pressure:
Cardiac X Peripheral
Output Vascular Resistance
43.
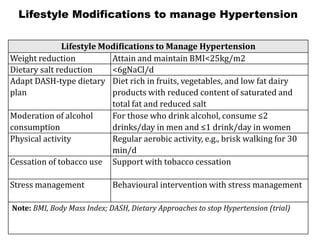
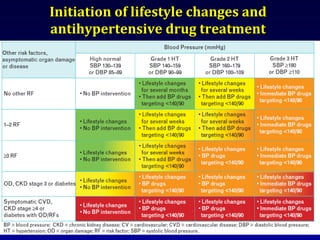
Lifestyle Modifications tomanage Hypertension
Lifestyle Modifications to Manage Hypertension
Weight reduction Attain and maintain BMI<25kg/m2
Dietary salt reduction <6gNaCl/d
Adapt DASH-type dietary
plan
Diet rich in fruits, vegetables, and low fat dairy
products with reduced content of saturated and
total fat and reduced salt
Moderation of alcohol
consumption
For those who drink alcohol, consume ≤2
drinks/day in men and ≤1 drink/day in women
Physical activity Regular aerobic activity, e.g., brisk walking for 30
min/d
Cessation of tobacco use Support with tobacco cessation
Stress management Behavioural intervention with stress management
Note: BMI, Body Mass Index; DASH, Dietary Approaches to stop Hypertension (trial)
44.
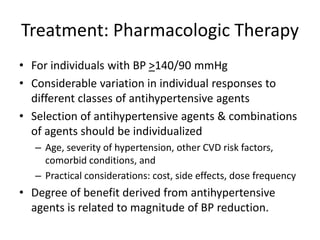
Treatment: Pharmacologic Therapy
•For individuals with BP >140/90 mmHg
• Considerable variation in individual responses to
different classes of antihypertensive agents
• Selection of antihypertensive agents & combinations
of agents should be individualized
– Age, severity of hypertension, other CVD risk factors,
comorbid conditions, and
– Practical considerations: cost, side effects, dose frequency
• Degree of benefit derived from antihypertensive
agents is related to magnitude of BP reduction.
45.
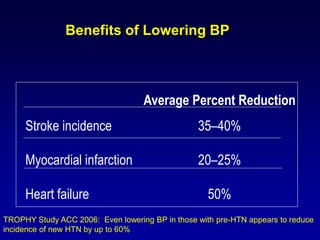
Benefits of LoweringBP
Average Percent Reduction
Stroke incidence 35–40%
Myocardial infarction 20–25%
Heart failure 50%
TROPHY Study ACC 2006: Even lowering BP in those with pre-HTN appears to reduce
incidence of new HTN by up to 60%
Antihypertensive medication
There arefive major classes of antihypertensive agents:
– A, Angiotensin Converting Enzyme Inhibitors (ACEIs) and Angiotensin
receptor blockers (ARBs);
– B, β-blockers (BBs);
– C, Calcium Channel Blockers (CCBs);
– D, Thiazide or thiazide-like diuretics; and
– Z, others (sympatholytics, α adrenergic blockers, centrally acting
alpha 2- agonists and direct arterial vasodilators.
This last class contains agents that are rarely used, or are obsolete,
and examples are as follows:
– Sympatholytics and alpha adrenergic blockers e.g. methyldopa and
prazocin
– Direct arterial vasodilators e.g. hydralazine
48.
First line classesof drugs
• Angiotensin Converting Enzyme Inhibitors (ACEIs) and
Angiotensin receptor blockers (ARBs)
• Calcium Channel Blockers (CCBs)
• Thiazide or thiazide-like diuretic
50.
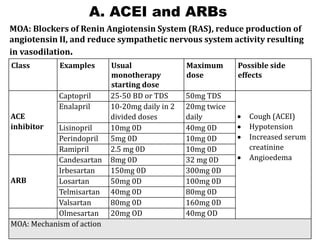
A. ACEI andARBs
MOA: Blockers of Renin Angiotensin System (RAS), reduce production of
angiotensin II, and reduce sympathetic nervous system activity resulting
in vasodilation.
Class Examples Usual
monotherapy
starting dose
Maximum
dose
Possible side
effects
ACE
inhibitor
Captopril 25-50 BD or TDS 50mg TDS
• Cough (ACEI)
• Hypotension
• Increased serum
creatinine
• Angioedema
Enalapril 10-20mg daily in 2
divided doses
20mg twice
daily
Lisinopril 10mg 0D 40mg 0D
Perindopril 5mg 0D 10mg 0D
Ramipril 2.5 mg 0D 10mg 0D
ARB
Candesartan 8mg 0D 32 mg 0D
Irbesartan 150mg 0D 300mg 0D
Losartan 50mg 0D 100mg 0D
Telmisartan 40mg 0D 80mg 0D
Valsartan 80mg 0D 160mg 0D
Olmesartan 20mg OD 40mg OD
MOA: Mechanism of action
51.
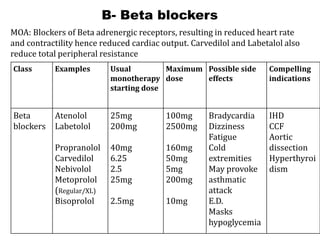
B- Beta blockers
ClassExamples Usual
monotherapy
starting dose
Maximum
dose
Possible side
effects
Compelling
indications
Beta
blockers
Atenolol
Labetolol
Propranolol
Carvedilol
Nebivolol
Metoprolol
(Regular/XL)
Bisoprolol
25mg
200mg
40mg
6.25
2.5
25mg
2.5mg
100mg
2500mg
160mg
50mg
5mg
200mg
10mg
Bradycardia
Dizziness
Fatigue
Cold
extremities
May provoke
asthmatic
attack
E.D.
Masks
hypoglycemia
IHD
CCF
Aortic
dissection
Hyperthyroi
dism
MOA: Blockers of Beta adrenergic receptors, resulting in reduced heart rate
and contractility hence reduced cardiac output. Carvedilol and Labetalol also
reduce total peripheral resistance
52.
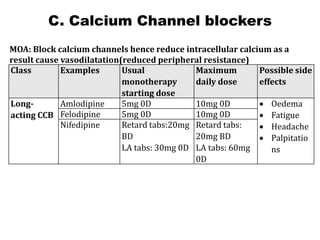
C. Calcium Channelblockers
MOA: Block calcium channels hence reduce intracellular calcium as a
result cause vasodilatation(reduced peripheral resistance)
Class Examples Usual
monotherapy
starting dose
Maximum
daily dose
Possible side
effects
Long-
acting CCB
Amlodipine 5mg 0D 10mg 0D • Oedema
• Fatigue
• Headache
• Palpitatio
ns
Felodipine 5mg 0D 10mg 0D
Nifedipine Retard tabs:20mg
BD
LA tabs: 30mg 0D
Retard tabs:
20mg BD
LA tabs: 60mg
0D
53.
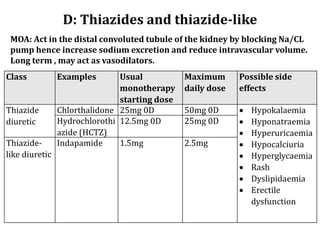
D: Thiazides andthiazide-like
MOA: Act in the distal convoluted tubule of the kidney by blocking Na/CL
pump hence increase sodium excretion and reduce intravascular volume.
Long term , may act as vasodilators.
Class Examples Usual
monotherapy
starting dose
Maximum
daily dose
Possible side
effects
Thiazide
diuretic
Chlorthalidone 25mg 0D 50mg 0D • Hypokalaemia
• Hyponatraemia
• Hyperuricaemia
• Hypocalciuria
• Hyperglycaemia
• Rash
• Dyslipidaemia
• Erectile
dysfunction
Hydrochlorothi
azide (HCTZ)
12.5mg 0D 25mg 0D
Thiazide-
like diuretic
Indapamide 1.5mg 2.5mg
54.
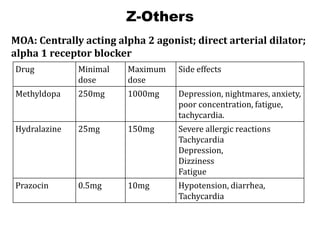
Z-Others
Drug Minimal
dose
Maximum
dose
Side effects
Methyldopa250mg 1000mg Depression, nightmares, anxiety,
poor concentration, fatigue,
tachycardia.
Hydralazine 25mg 150mg Severe allergic reactions
Tachycardia
Depression,
Dizziness
Fatigue
Prazocin 0.5mg 10mg Hypotension, diarrhea,
Tachycardia
MOA: Centrally acting alpha 2 agonist; direct arterial dilator;
alpha 1 receptor blocker
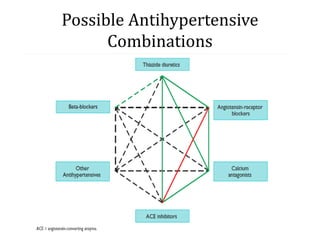
Preferred Combinations
• CalciumChannel blockers and ACE inhibitors
• Calcium channel Blockers and Thiazide diuretics
• ACE inhibitors and Thiazide diuretics
58.
Combinations that shouldbe
avoided
•An ACEI and ARB should never be used together in the same
patient because the combination causes severe hyperkalemia.
•Different antihypertensive medications from same class
should not be combined because they would cause severe
side effects with no additional benefits.
59.
Blood Pressure Goalsof
Antihypertensive Therapy
• < 140 mmHg SBP & < 90 mmHg DBP
• More aggressive BP targets for BP control
(e.g., office or clinic BP< 130/80 mmHg)
– diabetes, coronary heart disease, chronic kidney
disease, or additional CVD risk factors
60.
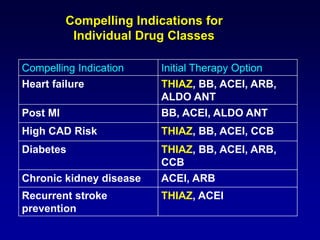
Compelling Indications for
IndividualDrug Classes
Compelling Indication Initial Therapy Option
Heart failure THIAZ, BB, ACEI, ARB,
ALDO ANT
Post MI BB, ACEI, ALDO ANT
High CAD Risk THIAZ, BB, ACEI, CCB
Diabetes THIAZ, BB, ACEI, ARB,
CCB
Chronic kidney disease ACEI, ARB
Recurrent stroke
prevention
THIAZ, ACEI
61.
Resistant hypertension
• Failureto achieve goal BP despite adherence to an appropriate
three-drug regimen including a diuretic in adequate doses and
after exclusion of false hypertension
• Contributors to resistant hypertension:
– Inadequate treatment
– Extracellular volume expansion:
➢because of renal insufficiency, sodium retention due to
treatment with vasodilators, high-salt diet, or insufficient
dosing of diuretic
– Poor compliance
– Secondary hypertension
– White coat hypertension
62.
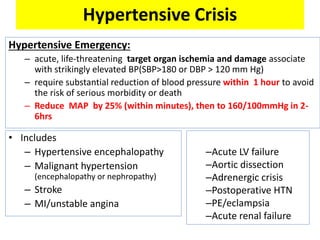
Hypertensive Crisis
Hypertensive Emergency:
–acute, life-threatening target organ ischemia and damage associate
with strikingly elevated BP(SBP>180 or DBP > 120 mm Hg)
– require substantial reduction of blood pressure within 1 hour to avoid
the risk of serious morbidity or death
– Reduce MAP by 25% (within minutes), then to 160/100mmHg in 2-
6hrs
• Includes
– Hypertensive encephalopathy
– Malignant hypertension
(encephalopathy or nephropathy)
– Stroke
– MI/unstable angina
–Acute LV failure
–Aortic dissection
–Adrenergic crisis
–Postoperative HTN
–PE/eclampsia
–Acute renal failure
63.
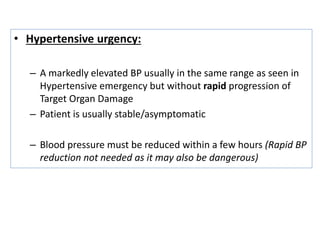
• Hypertensive urgency:
–A markedly elevated BP usually in the same range as seen in
Hypertensive emergency but without rapid progression of
Target Organ Damage
– Patient is usually stable/asymptomatic
– Blood pressure must be reduced within a few hours (Rapid BP
reduction not needed as it may also be dangerous)














































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



