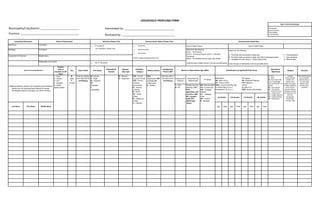
This document appears to be a household profiling form that collects information on household members, including their relationship to the head of household, demographics, medical history, education, religion, family planning methods, and other details. It collects names, gender, dates of birth, civil status, ethnicity, socioeconomic status, and other identifying information for each member. It also documents the household's water source, toilet facilities, and whether they are part of a National Household Targeting System for Poverty Reduction program. The form is used to classify members by age, health risks, and collect quarterly updates on household members and their information.