Hemocron Elite: A Comparative study of Anticoagulation Monitoring Tests in Transcatheter Aortic Valve Replacement (TAVR) Procedures

Measurement of the activated clotting time (ACT) during procedures guides maintenance of proper anticoagulation, thereby preventing thrombus formation and potential embolization leading to adverse clinical outcomes. Accurate monitoring of the level of anticoagulation can decrease embolic events and improve patient care. Our study compared the ACT results from two modern anticoagulation tests (Hemocron ACT+ and Hemocron ACT-LR) to assess for accuracy by surveying and analyzing activated clotting times in 45 patients undergoing Transcatheter Aortic Valve Replacement (TAVR) procedures utilizing both tests. We found a statistical significance difference existed between the two tests due to a p value less than 0.05 and conclude that there are possible patient benefits using the ACT-LR test in the operative setting.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hemocron Elite: A Comparative study of Anticoagulation Monitoring Tests in Transcatheter Aortic Valve Replacement (TAVR) Procedures
Similar to Hemocron Elite: A Comparative study of Anticoagulation Monitoring Tests in Transcatheter Aortic Valve Replacement (TAVR) Procedures (20)
More from Karounka Keita M.S. CCP/LP
More from Karounka Keita M.S. CCP/LP (9)
Recently uploaded
Recently uploaded (20)
Hemocron Elite: A Comparative study of Anticoagulation Monitoring Tests in Transcatheter Aortic Valve Replacement (TAVR) Procedures
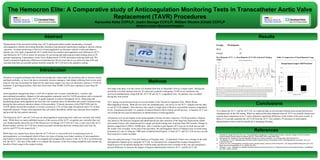
- 1. The Hemocron Elite: A Comparative study of Anticoagulation Monitoring Tests in Transcatheter Aortic Valve Replacement (TAVR) Procedures Karounka Keita CCP/LP, Justin Savage CCP/LP, William Nicotra (Chief) CCP/LP Medstar Union Memorial Hospital Methods Abstract Introduction Results Conclusions References I. Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence Based Clinical Practice Guidelines (8th Ed). Chest 2008;133(6 Suppl):299S-339S. II. Spyropoulos AC. Bridging of oral anticoagulation therapy for invasive procedures. Curr Hematol Rep. 2005;4(5):405-413. III. Van Mieghem, N. et al. Histopathology of Embolic Debris Captured During Transcatheter Aortic Valve Replacement. Circulation. 2013 Jun 4;127(22):2194-201. IV. Tremey, B. et al. “Anticoagulation monitoring during vascular surgery: accuracy of the Hemochron_ low range activated clotting time (ACT-LR).” British Journal of Anaesthesia. 97 (4). (2006): 453–459. V. Racioppi, L. et al. “Validation of a bedside activated clotting time test (Hemochron Jr II Signature) with low dose heparin therapy.” Anaesthesia. Apr; 64(4). (2009): 430-434. Table 1.Comparison of Total Heparin Usage Measurement of the activated clotting time (ACT) during procedures guides maintenance of proper anticoagulation, thereby preventing thrombus formation and potential embolization leading to adverse clinical outcomes. Accurate monitoring of the level of anticoagulation can decrease embolic events and improve patient care. Our study compared the ACT results from two modern anticoagulation tests (Hemocron ACT+ and Hemocron ACT-LR) to assess for accuracy by surveying and analyzing activated clotting times in 45 patients undergoing Transcatheter Aortic Valve Replacement (TAVR) procedures utilizing both tests. We found a statistical significance difference existed between the two tests due to a p value less than 0.05 and conclude that there are possible patient benefits using the ACT-LR test in the operative setting. To evaluate the ACT+ and the ACT-LR, we collected data on all activated clotting times using both devices simultaneously in the OR setting. When we analyzed the data obtained from all ACTs we actually found more contrast than comparison as our T-tests reflected a significant difference in the results of the tests overall. A delta of 53 seconds separated the ACT-LR from the ACT+ but yielded a 5% decrease in total heparin administration which could be beneficial to managing bleeding. Our study took place over the course of 6 months from July to December 2016 at a single center. During this period the activated clotting times for 45 consecutive patients undergoing TAVR at our institution was surveyed simultaneously using both the ACT-LR and ACT+ coagulation tests. No patients were excluded during this time period. ACT testing was performed using two recent models of the Hemocron Signature Elite: Whole Blood Microagulation System. Both devices were run simultaneously; one device to run ACT+ samples and the other to run ACT-LR samples. These devices only require a single drop of blood to successfully measure coagulation levels. Anesthesia provided 3 cc samples of arterial blood to allow testing on both devices. A baseline ACT was ran on both devices and recorded prior to administration of anticoagulation. All patients were given heparin as the anticoagulant of choice for their respective TAVR procedures. Heparin was dosed at 100 units per kilogram and administered just after insertion of the large bore deployment sheath and minutes before valve deployment for a target activated clotting time of greater than 300 seconds. Dosage in patients ranged from 5,000 to 10,000 units. After 3 minutes a post heparin ACT was run on both devices and the results were recorded. At the end of the procedure, the anticoagulant effects of Heparin were reversed using protamine at a rate of 10mg per 1000 units of administered heparin. A final ACT+ and ACT-LR test are run and their respective results recorded. Data was analyzed using T-Test and Analysis of Variance tests. To determine if there was a change in the total intraoperative heparin given using the ACT-LR we retrospectively compared the average intraoperative heparin given for all patients during this 6 month study and the previous 6 months of the year and calculated a percent difference to measure the impact of heparin administration between ACT+ and the ACT-LR. Advances in surgical technique and clinical knowledge have taken high risk procedures due to invasive access and high morbidity, to lower risk due to minimally invasive strategies. Individuals suffering from severe aortic stenosis who may be deemed too high risk for open-heart surgery now have an alternative option in TAVR for treatment. A growing procedure, there have been more than 50,000 TAVR cases reported in more than 40 countries.1 Anticoagulation management plays a vital role in patient care in many cardiothoracic, vascular, and interventional procedures. Heparin is the anticoagulant commonly used for TAVR procedures and is measured using the activated clotting time (ACT) to guide surgeons to achieve therapeutic levels. Measuring and maintaining proper anticoagulation prevents the risk of patient harm via thrombus and emboli formation both during the intra and post operative phases of the procedure.2 Clinical outcomes of the PARTNER trial for TAVR studies showed the incidence of strokes occurred in 5.5% of their high risk patients and 6.7% of their inoperable patients.3 Proper anticoagulation that can reduce thrombotic emboli may decrease these numbers and provide the best patient outcomes. The Hemocron ACT+ and ACT-LR tests are anticoagulation monitoring tools which are currently and widely used. While there are many published sources of the success of the ACT+ in patient care, currently there are very limited studies about the use of the Hemocron Low Range (ACT-LR) ACT test, a sister test to the ACT+. Recent studies with the ACT-LR have noted successful correlations between clotting times and Anti-Xa activity and PTT levels respectively.4, 5 While these two studies have shown that the ACT-LR test is a successful tool in measuring levels of anticoagulation, we investigated which of these two types of testing were better monitors of anticoagulation and found no current research that has investigated and compared the success of the ACT-LR to its predecessor test, the ACT+. The aim of this study is to compare the accuracy of the two testing modalities and examine the benefits of their usage in the surgical setting. Groups Participants Male 21 Female 24 Post Heparin ACT+ vs. Post Heparin ACT-LR Activated Clotting Times