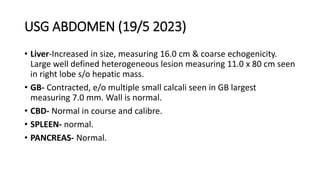
This case involves a 29-year-old female teacher presenting with right upper quadrant pain for 3 months and jaundice for 20 days. Investigations revealed elevated liver enzymes and bilirubin. Imaging showed a large hepatic mass and biopsies indicated metastatic adenocarcinoma. The second case is a 61-year-old female with recurrent abdominal pain and vomiting over 4 months. Imaging found an enlarged liver with a large heterogeneous mass. Biopsies were inconclusive but imaging suggested possible gallbladder carcinoma with metastases. Both patients underwent further endoscopic and imaging workup to characterize the liver lesions and evaluate for obstruction.