1.WATER FLUORIDATION:
water cancontain1ppm.
Provides widespread penetration into
population without individual effort
and is effect and safe.
Most effective and cheap way to provide
fluoride supplementation.
SYSTEMIC ADMINISTRATION
6.
2.SALT FLUORIDATION:
The saltconsumption is variable between
families.
resulting in the risk of fluorosis when
consuption is in large amounts.
7.
3.MILK FLUORIDATION:
Administration offluoride by milk has an
advantage over water fluoridation that can be
targeted directly at segments of population deemed
to be at risk . Fluoridated milk distribution to
children is best done through an established or
existing system like school milk or milk for
kindergartens and nursery schools.
Self applied:
1.fluoride toothpaste- the fluoride
concentration is between 525-1450ppm.
2.mouthrinses- 0.2%NaF typically 10ml for 1
min.
3.gels-contain neutral NaF and acidulated
phosphate fluoride with concentration of
5000ppm and stannous fluoride which has
concentration of 1000ppm.
TOPICAL APPLICATION:
10.
PROFESSIONALLY APPLIED:
gels andfoams contain higher conc of fluoride about 5000-
12300ppm
applicated in dental office . usually twice a year.
which includes
2% sodium fluoride-knutsons technique- 4 visits procedure is
recommended foe ages 3,7,11,13 years.
8% stannous fluoride-muhlers technique – 2 visits that is 6-12
months interval
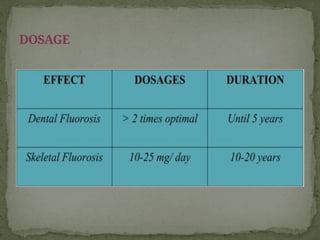
Fluoride is oftencalled double edged sword.
Inadequate ingestion of fluoride is associated with
dental caries and an excessive intake of fluoride
can leads to dental and skeletal fluorosis.
FLUORIDE TOXICITY:
13.
WHO,1963 has recommendedoptimum level of
fluoride in drinking water as 0.5-1.0ppm
The average daily intake of fluoride from all
source recommended for adults is 2.0-2.2mg
and in children 5-14 years it is 1.02mg which
leads to plasma levels of 0.008-0.08 ppm.
HOWSAFE IS SAFE?
14.
ACUTE TOXICITY:
excessiveingestion of fluoride over a short
period of time produces acute toxicity.
CHRONIC TOXICITY:
excessive ingestion of fluoride over a long
period of time produces chronic toxicity.
TYPES
15.
The speed andseverity of the response are dependent on
1.amount of ingestion
2.weight and age of the individual
SYMTOMS:
nausea
stomach irritant
abdominal cramps
vomiting
diarrhea , excess salivation
dehydration and thrist.
ACUTE TOXICITY:
16.
CERTAINLY LETHAL DOSE(CLD):
amountof drug likely to cause death.
adult=5-10gNaF taken at one time or 32-64mg
F/kg body weight
SAFETY TOLERATED DOSE(STD):
Maximum dose that can be given without toxicity
adult=1.2gNaF or 8-16mgF/kg body weight.
DOSAGE
17.
1.Should be aimedat reducing the amount of
fluoride available for absorption from GIT.
2.Vomiting should be induced
3.If calcium containing solutions are not available
as much as milk can be ingested should be given.
4.Patient should be transported to the hospital at
the earliest.
TREATMENT:
18.
Long term ingestionof small
amounts of fluoride leads to
fluorosis.
It is a disease caused by deposition
of fluorides in hard and soft tissues
of body.
CHRONIC TOXICITY:
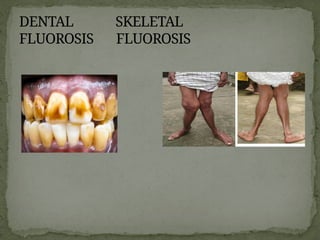
It is ahypoplasia or hypomineralisation of tooth
enamel or dentin produced by the chronic
ingestion of excessive amounts of fluoride during
the period of tooth development.
DENTAL FLUOROSIS
22.
CLINICAL FEATURES:
fluorosisoccurs symmetrically between the dental
arch.
the premolar is usually affected
followed by second molar, maxillary incisors, canine,
1st
molar and mandibular incisors.
23.
Ingestion of waterwith a fluoride conc .of 2-3
times greater than the recommended.
Causes white flecks and chacky opaque areas on
the enamel.
SEVERE FLUOROSIS:
ingestion of water with a fluoride conc. Of 4 times
greater than the recommended.
Causes brown pitted corroded appearance.
MILD FLUOROSIS:
bleaching andenamel micro abrasion-
techniques are conservative, and provide
highly satisfactory result without excessive
wear of sound tooth region.
composite resin and resin modified glass
ionomer are also used for treating discolored
area.
esthetic veneers and prosthetic crowns if
needed.
MANAGEMENT:
27.
fluoride isreadily incorporated into the crystalline
structure of bone, and will accumulate over time.
It is a bone and joint condition associated with
prolonged exposure to high conc. of fluoride.
fluoride increases bone density and causes changes
in the bone that leads to joint stiffness and pain.
SKELETAL FLUOROSIS:
28.
Defluoridation is definedas “the downward
adjustment of level of fluoride in drinking water
to optimum level”.
Several methods have been suggested from time to
time for defluoridation .the two basic methods
are:
1.ion exchange process and adsorption
2.nalgonda technique-addition of chemicals to
water during treatment.
DEFLUORIDATION:
29.
These are commerciallyproduced resin:
carbion: it is a cation exchange resin of good
durability and can be used on sodium and
hydrogen cycles.
defluoron 1: it is sulphonated saw dust
impregnated with2% alum solution.
defluoron 2: it is sulphonated coal using
aluminium solution.
ION EXCHANGE RESINS:
30.
It involves additionof aluminium salts, lime and
bleaching powder
Followed by rapid mixing, flocculation,
sedimentation , filtration and disinfection.
NALGONDA TECHNIQUE:
31.
rapid mix:provides thorough mixing of chemicals.
flocculation: gentle agitation. Combination of poly
hydroxy aluminium complex with fluoride and
polymeric aluminium hydroxides are formed (flocs).
sedimentation: permits settling of flocs loaded with
fluorides and other impurities.
filtration: rapid gravity sand filters.
disinfection: rechlorinated with bleaching powder
before distribution.
MECHANISM OF NALGONDA TECHNIQUE:
32.
no regenerationof media
no handling of caustic acids and alkalies
adaptable for domestic use
Simplicity of design, construction , operation and
maintenance
highly efficient removal of fluoride to desirable
levels
Little wastage of water
Needs minimum of mechanical and electrical
equipments
SALIENT FEATURES OF NALGONDA TECHNIQUE: