A lipid profile measures levels of total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides to evaluate a patient's risk for heart disease. It is often ordered for patients with risk factors like family history of high cholesterol, obesity, diabetes or hypertension. High LDL and triglyceride levels and low HDL levels can indicate increased risk. A lipid profile provides a complete picture of lipids to guide treatment and prevention strategies.




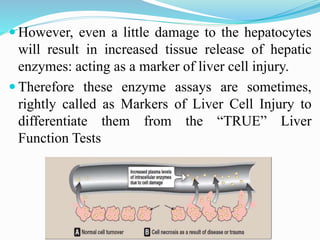
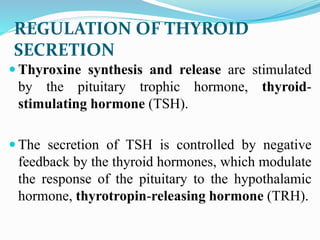
![TSH :
- The single most sensitive, specific and
reliable test of thyroid status .
- In primary hypothyroidism, [TSH] is
increased.
- In primary hyperthyroidism, [TSH] is
decrease or undetectable](https://image.slidesharecdn.com/finallecture-150516092748-lva1-app6892/85/Final-lecture-50-320.jpg)
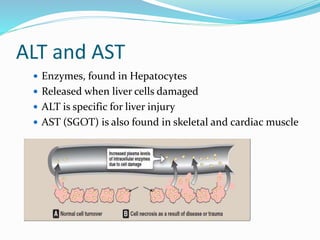
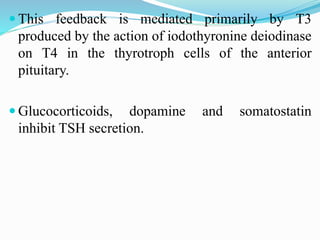
![Total T4 and Total T3 :
- More than 99% of T4 and T3 circulate
in plasma bound to protein
- Both [total T4] and [total T3] change if
[TBG] alters, e.g. in pregnancy
Free T4 and Free T3
Free thyroid hormone concentrations
are independent of changes in
the concentration of thyroid-hormone
binding proteins → more
reliable for diagnosis of thyroid
dysfunction](https://image.slidesharecdn.com/finallecture-150516092748-lva1-app6892/85/Final-lecture-51-320.jpg)
























































































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)












