More Related Content
Similar to Extended roles
Similar to Extended roles (20)
Extended roles
- 1. RESEARCH ARTICLE
Extended Roles of Non‐physician Health Professionals
and Innovative Models of Care within Europe: Results
from a Web‐based Survey
Tanja Stamm PhD, MSc, MBA1* & Jackie Hill PhD, MPhil (Dist), RN, FRCN2
1
Department of Internal Medicine III, Division of Rheumatology, Medical University of Vienna, Vienna, Austria, and FH Campus Wien,
Department of Health, Division of Occupational Therapy, University of Applied Sciences, Vienna, Austria
2
Academic and Clinical Unit for Musculoskeletal Nursing (ACUMeN), Academic Section of Musculoskeletal Disease, Leeds Institute of
Molecular Medicine, Leeds, UK
Abstract
Background and objective. Due to the increasing prevalence of rheumatic diseases, extended roles of non‐physician
health professionals and innovative models of care may be important options in rheumatology in the future. Extended
roles have been pioneered in the UK, Canada, USA and Australia and been found to be effective and safe. However,
few data are available about mainland Europe, so the aim of this study was to explore the current status of the extended
roles undertaken by health professionals within Europe, and the corresponding models of care used.
Methods. Non‐physician health professionals from various European countries were asked to complete a web‐
based survey using convenience and snowball sampling techniques. Data analysis involved calculating descriptive
statistics and frequencies based on the countries where the participants currently worked.
Results. Of the 479 health professionals who filled in the survey, 430 (92%) indicated that they were performing
extended roles. Considerable differences between the 27 participating countries existed, in terms of which extended
roles and which innovative models of care were being used. Barriers to performing extended roles were cited as the
attitude of rheumatologists in all but eight countries, while attitudes of patients were less common barriers. Lack of
knowledge, education and educational opportunities were also experienced in several countries.
Conclusion. The present study produced the first data on extended roles for non‐physician health professionals
and corresponding innovative models of care in rheumatology within Europe. We recommend increasing
educational opportunities, as well as developing strategies to limit the barriers experienced. Copyright © 2011 John
Wiley & Sons, Ltd.
Keywords
Extended roles; occupational therapy; physical therapy; nursing; social work; psychology; rheumatology health professionals
*Correspondence
Tanja Stamm, Department of Internal Medicine III, Division of Rheumatology, Medical University of Vienna, Währinger Gürtel 18‐20, 1090
Vienna, Austria.
Email: tanja.stamm@meduniwien.ac.at
Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/msc.201
Introduction osteoarthritis (OA) affects 60–70% of the population
The prevalence of rheumatic diseases increases with age above the age of 65 years (Dahaghin et al., 2005a, b;
and with the increasing longevity of the population Kraus, 1997). At the present time, almost 80% of the
(World Health Organization, 2004). For example, population can expect to live through most of their
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
- 2. Extended Roles of Health Professionals in Europe Stamm and Hill
seventh decade of life, so the impact of OA is likely to extended roles and to develop recommendations/
increase even further in future (Kraus, 1997). Rheumatic guidelines for European HPs wishing to undertake
diseases affect not only body functions and structures, extended roles based on the survey results.
but also activities and the societal participation of the
individual (Stamm et al., 2009). Given the ever‐increasing
Methods
number of people affected by rheumatic diseases, as well
as their various needs, innovative models of care, such as Design
implementing extended roles for multidisciplinary, non‐ A 10‐minute, anonymous survey with a web‐based ques-
physician health professionals (HPs), may be an tionnaire was conducted. The survey was available for one
important option in future rheumatology care. Extended month (April 2010), with an extension period of 15 days.
roles can be defined as tasks which have not been
commonly undertaken by HPs, or a certain group of HPs,
Participants
to date and which require at least additional training or
education in addition to basic professional training. Sampling followed convenience and snowball sampling
Extended roles for HPs in rheumatology at present techniques. HPs from different disciplines, including
include consultant roles (defined as expert practice, nurses, occupational therapists, physiotherapists, psy-
leadership, education and research) (Humphreys et al., chologists and social workers, working in rheumatology,
2007), advanced clinical tasks specifically undertaken by from as many countries as possible, were invited to
nurses, such as examining the musculoskeletal system, participate and contacted via regular and co‐opted
assessing disease status, managing symptoms, recom- members of the European League Against Rheumatism
mending changes to or prescribing drug treatment and (EULAR) Standing Committee for Health Professionals
making referrals to other HPs (Hill et al., 2009; Miles in Rheumatology, the EULAR member organizations,
et al., 2006), administering intra‐articular injections individuals (if no member organization existed in a
(Meadows and Sheehan, 2005) and managing patient certain country) and participants of the EULAR HP
advice lines (McCabe et al., 2009; Thwaites, 2004). Teach‐the‐Teachers courses. In addition, each health
Further examples include triage recommendations for professional was asked to share the web link for this
patients with OA carried out by physiotherapists survey with colleagues and HPs from other countries
(MacKay et al., 2009) and triage by occupational therapists known to work in rheumatology.
of whether or not patients require hospital admission in
emergency care settings (Cusick et al., 2009). Data gathering
Several studies have found extended HPs roles to be
The questionnaire was derived from the literature on the
effective and safe (Hill, 1986; Hill et al., 1994, 2009;
extended roles of HPs (Hill et al., 2009; Humphreys et al.,
MacKay et al., 2009; Ryan et al., 2006). The implemen-
2007). Pilot testing of the questionnaire was undertaken
tation of extended roles for HPs commonly occurs in
to ensure the relevance of the questions for the different
parallel with the development of innovative models of care,
countries. The questionnaire was translated from English
such as internet‐based care, telephone helplines and triage
into the following 11 languages: Czech, Estonian,
models to decrease the number of patients on waiting lists.
Finnish, French, German, Greek, Italian, Lithuanian,
The literature demonstrates that extended roles for
Polish, Portuguese and Spanish. These languages were
HPs and corresponding innovative models of care have
chosen, as we expected fewer health professionals of these
been pioneered in the UK, Canada, USA and Australia
nationalities to be familiar with English.
(Cusick et al., 2009; Hill et al., 2009; Humphreys et al.,
2007). However, there are no data on the current
Data analysis
situation in mainland Europe and no common
European perspective concerning the situation of HPs Data were transferred electronically from the web‐
performing extended roles. Therefore, the aims of this based questionnaire and corresponding database
study were to explore the current status of extended (http://www.surveymonkey.com) to a Microsoft Excel
roles undertaken by HPs within Europe, to gain an spreadsheet. Data analysis involved calculating descrip-
overview of the different models of care and clinical tive statistics and frequencies based on the countries
and research settings in which HPs undertake these where the participants currently worked.
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
- 3. Stamm and Hill Extended Roles of Health Professionals in Europe
Results physiotherapists and 45 (9%) occupational thera-
pists, these three groups comprised 92% of the
Participants
cohort. The remaining 8% were psychologists,
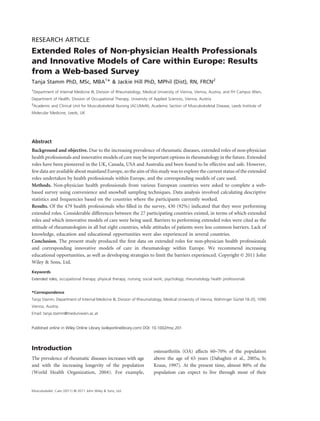
A total of 479 HPs from 27 countries participated in podiatrists, social workers and other professionals,
the survey (Figure 1); their demographic data are such as clinical pharmacists, medical secretaries and
shown in Table 1. Sixty‐one per cent of the all clinical study coordinators. No nutritionists com-
participants were nurses and, with the 103 (22%) pleted the survey.
Number of participants
United Kingdom 120
Turkey 2
Switzerland 62
Sweden 8
Spain 27
Slovenia 6
Slovakia 5
Serbia 18
Romania 1
Portugal 28
Poland 5
Norway 40
Netherlands 9
Malta 3
Luxembourg 1
Lithuania 12
Latvia 1
Ireland 1
Greece 1
France 2
Finland 19
Estonia 29
Denmark 3
Czech Republic 41
Cyprus 4
Belgium 11
Austria 8
0 20 40 60 80 100 120 140
Figure 1 Distribution of the survey participants by country. The bars indicate the total number of participants per country. Countries are
listed from bottom to top in alphabetical order
Table 1. Demographic data of the survey participants
Total Age group (in years) Clinical experience (in years) Research experience (in years)
20–30 31–40 41–50 Over 0–1 2–10 11–20 More 0–1 2–10 11–20 More
50 than 20 than 20
Nurse 294(61%) 34 66 104 90 13 116 106 49 108 133 27 5
Occupational therapist 45 (9%) 7 10 13 15 2 21 11 11 27 10 4 2
Psychologist 13 (3%) 5 6 2 – 4 4 5 – 7 4 2 –
Podiatrist 6 (1%) 2 2 1 1 – 5 – 1 4 2 – –
Physiotherapist 103 (22%) 15 30 35 23 2 36 30 34 62 26 2 3
Social worker 5 (1%) – 1 – 4 1 1 3 – 3 1 1 –
Other 13 (3%) 3 4 2 3 3 4 4 2 4 8 – 1
Total 479 63 115 155 136 25 187 159 97 215 184 36 11
(13%) (24%) (32%) (28%) (5%) (39%) (33%) (20%) (45%) (38%) (8%) (2%)
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
- 4. Table 2. Extended roles performed by health professionals within Europe. If one participant in a certain country marked a specific task, this is marked with a ■ in the table in the column relating to this
country
If you are performing extended
roles in the rheumatology
setting in which you are
currently working, please
indicate these by ticking the Czech
Extended Roles of Health Professionals in Europe
boxes below. Austria Belgium Cyprus Republic Denmark Estonia Finland France Greece Ireland Latvia Lithuania Luxembourg Malta Netherlands Norway Poland Portugal Romania Serbia Slovakia Slovenia Spain Sweden Switzerland Turkey UK
Work as a consultant/ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
advanced practitioner
Manage your own caseload ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
independently
Triage ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Assess disease status and ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
activity
Examine the musculoskeletal ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
system
Formulate and carry out a ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
plan of disease management
Manage disease symptoms ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Recommend changes of drug ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
treatment
Prescribe medications by ■ ■ ■ ■ ■ ■ ■
protocols
Prescribe medications ■ ■ ■ ■
independently
Give intra‐articular injections ■ ■ ■ ■ ■ ■
Making referrals to other ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
health professionals
Make referrals to physicians, e.g. ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
orthopaedic surgeon
Admit patients to hospital ■ ■ ■ ■ ■ ■ ■ ■ ■
wards
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
Stamm and Hill
- 5. Discharge patients from your ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
care
Recommendations for further ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
and other treatment options
Address psychological ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Stamm and Hill
problems
Address social problems ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Order investigations such as ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
X‐rays and blood tests
Assess the patients’ knowledge ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
of their disease
Lead/teach patient education ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
courses
Design patient education ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
materials
Manage patient telephone ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
advice lines
Supervise health professionals ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
from different disciplines,
including physicians
and medical students
Teach health professionals from ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
different disciplines,
including physicians and
medical students
Manage clinical trials ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Work as a research assistant ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lead clinical trials/research ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Undertake independent ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
research
Assessment other than typical ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
for your profession
If one participant in a certain country marked a specific task, this is marked with a ■ in the table in the column relating to this country.
Extended Roles of Health Professionals in Europe
- 6. Table 3. Innovative models of care and research settings in which the survey participants worked
If you do work in an extended role,
please specify the model of care in
which you are currently performing
the extended roles you identified in Czech
the previous question. Austria Belgium Cyprus Republic Denmark Estonia Finland France Greece Ireland Latvia Lithuania Luxembourg Malta Netherlands Norway Poland Portugal Romania Serbia Slovakia Slovenia Spain Sweden Switzerland Turkey UK
Traditional medical setting ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
(physician prescribes)
Multi/interdisciplinary rheumatology/ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Extended Roles of Health Professionals in Europe
rehabilitation team, with physician
being the team leader
Multi/interdisciplinary rheumatology/ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
rehabilitation team, with non‐physicians
as the team leader
Academic/research setting, with the ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
physician as the team leader
Academic/research setting with different ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
professionals, with non‐physicians as the
team leader
Community/primary care setting, with the ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
physician as the team leader
Community/primary care setting, with ■ ■ ■ ■ ■ ■
non‐physicians as the team leader
Telephone helpline ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Internet‐based helpline ■ ■ ■ ■ ■
Internet‐based care ■ ■ ■
Clinic led by nurse or other health ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
professional
Private practice ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
If one participant in a certain country marked a specific task, this is marked with a ■ in the table in the column relating to this country.
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
Stamm and Hill
- 7. Stamm and Hill
Table 4. Barriers experienced by health professionals that keep them from performing extended roles in a certain country
Whether or not you work in extended
roles, are there any barriers that keep
you or your colleagues from performing Czech
extended roles in your centre? Austria Belgium Cyprus Republic Denmark Estonia Finland France Greece Ireland Latvia Lithuania Luxembourg Malta Netherlands Norway Poland Portugal Romania Serbia Slovakia Slovenia Spain Sweden Switzerland Turkey UK
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
Lack of knowledge ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of education ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of educational opportunities ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Legal constraints ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Attitude of rheumatologists ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Attitude of colleagues or other ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
health professionals
Attitude of patients ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of support from colleagues ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of information during basic ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
training
Lack of role models ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of time ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
Lack of funding ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ ■
No need for extended roles ■ ■ ■ ■ ■
If one participant in a certain country marked a specific task, this is marked with a ■ in the table in the column relating to this country.
Extended Roles of Health Professionals in Europe
- 8. Extended Roles of Health Professionals in Europe Stamm and Hill
Status of performance of extended roles Advantages of performing extended roles
in Europe
An open question inviting participants to cite the
In the survey, 430 (90%) HPs said that they were potential advantages of performing extended roles was
currently performing extended roles. The performance answered by 272 (57%) participants. Their responses
of extended roles in the 27 responding countries is
included three main areas: (i) advantages for the
described in Table 2. The only country in which all
patient (e.g. the provision of more holistic care,
extended roles described in the survey were performed
seamless care, a multidisciplinary perspective in care,
by HPs was the UK. The tasks ‘design patient
education materials’ (all countries, but two), ‘assess easier and timely access to care); (ii) advantages for the
disease status and activity’ and ‘lead/teach patient healthcare system/institution (e.g. more cost‐effective
education courses’ (all countries, but three) were those care due to shorter access time and fewer professionals
most frequently marked as being performed by HPs in involved); and (iii) advantages for the professionals
all responding countries. who performed extended roles (e.g. more challenging
Educational courses were the most important workload, increased self‐confidence, self‐development
additional training requested to fulfil the extended and knowledge, as well as career progression).
roles (42% of all participants), followed by informal
training in the workplace (32%) and formal training in Discussion
the workplace (28%). Seventy‐three (15%) participants
This was the first survey of its kind, focusing on the
with a Masters degree and 13 (3%) with a PhD degree
extended roles of HPs and corresponding innovative
thought that their degree was necessary for performing
models of care in rheumatology within Europe. The
extended roles.
data collected have enabled a comparison to be made
between different countries. Ninety per cent of HPs
Models of care
were performing extended roles, with the three
Innovative models of care and research settings (e.g. commonest activities including design patient educa-
with non‐physicians as leaders, and telephone‐ or tion materials, assess disease status and activity, and
internet‐based care) were used in all countries lead/teach patient education courses. No HPs from
(Table 3), except for Greece, Ireland, Latvia, Romania Germany completed the survey and all those who
and Turkey. completed the survey from Italy were physicians (these
datasets were deleted). In order to establish equal
Barriers experienced by HPs to keep them opportunities for patients with rheumatic diseases
from performing extended roles within Europe, such as access to care and treatment,
we suggest that innovative models of care, together
An overview of the barriers experienced by HPs in with extended roles for HPs, should be introduced and
regard to performing extended roles is shown in promoted in all European countries.
Table 4. A considerable number of HPs (249; 53%) Several HPs in our survey indicated that they needed
indicated that they had experienced barriers. In Estonia additional training to perform extended roles. Educa-
and Switzerland, all of the barriers described in the tional courses were the most often sought additional
questionnaire had been experienced. Legal constraints training. It is therefore essential to introduce educa-
had been experienced in all but seven countries and tional courses, such as the EULAR Teach‐the‐Teachers
most often been experienced in Austria (by 63% of the course, to HPs in countries where extended roles and
participants), Switzerland (55%) and Portugal (43%), innovative models of care are rarely used. In addition,
compared with just 9% of participants in the UK. enabling HPs to achieve higher qualifications may
Interestingly, the attitudes of rheumatologists had influence whether they engage in extended roles and
been experienced as barriers to performing extended the introduction of innovative models of care.
roles in all but eight countries, while the attitudes of HPs throughout Europe experienced barriers to
patients were cited as being a barrier in nine countries. performing extended roles, so the use of innovative
Lack of knowledge, education and educational oppor- models of care may be limited. The main barriers
tunities were also perceived as barriers in several recorded included legal constraints, the attitudes of
countries. rheumatologists and patients, knowledge and educational
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.
- 9. Stamm and Hill Extended Roles of Health Professionals in Europe
opportunities. The German‐speaking region of Europe, Dahaghin S, Bierma‐Zeinstra SM, Reijman M, Pols HA,
particularly Austria, is an area where legal constraints Hazes JM, Koes BW (2005b). Prevalence and determi-
might prevent HPs from performing extended roles and nants of one month hand pain and hand related
this could have been the reason why innovative models of disability in the elderly (Rotterdam study). Annals of
the Rheumatic Diseases 64: 99–104.
care were also hardly used there.
Hill J (1986). Patient evaluation of a rheumatology
The potential use of innovative models of care may
nursing clinic. Nursing Times 82: 42–3.
depend on the professional and educational status of
Hill J, Bird HA, Harmer R, Wright V, Lawton C (1994). An
non‐physician HPs in a certain country. Innovative evaluation of the effectiveness, safety and acceptability of a
models of care include multi/interdisciplinary teams in nurse practitioner in a rheumatology outpatient clinic.
which all participating HPs have an equal professional British Journal of Rheumatology 33: 283–8.
status, so that either a physician or a non‐physician can Hill J, Lewis M, Bird H (2009). Do OA patients gain
be the team leader, compared with traditional settings, additional benefit from care from a clinical nurse
in which always physicians were/are the team leaders. specialist? A randomized clinical trial. Rheumatology
The results from this survey could be applied in several 48: 658–64.
ways – for example, for lobbying for extended roles Humphreys A, Johnson S, Richardson J, Stenhouse E,
in those countries in which this does not currently Watkins M (2007). A systematic review and meta‐
synthesis: Evaluating the effectiveness of nurse, midwife/
occur, using the inter‐country comparisons. Comparing
allied health professional consultants. Journal of Clinical
European with US data might be an interesting future
Nursing 16: 1792–808.
challenge for defining extended roles and models of care
Kraus VB (1997). Pathogenesis and treatment of osteoar-
in terms of the different social and healthcare systems. thritis. The Medical Clinics of North America 81: 85–112.
Starting a common world‐wide discussion on the MacKay C, Davis AM, Mahomed N, Badley EM (2009).
extended roles of non‐physician HPs may enable HPs Expanding roles in orthopaedic care: A comparison of
to extend their current roles in countries where this is not physiotherapist and orthopaedic surgeon recommenda-
yet common practice. Further, educational needs could tions for triage. Journal of Evaluation in Clinical
be identified in several countries, as well as barriers which Practice 15: 178–83.
could be addressed within international organizations McCabe C, McDowell J, Cushnaghan J, Butts S, Hewlett S
such as EULAR. (2009). Rheumatology telephone helplines: An activity
analysis. Rheumatology 39: 1390–5.
Meadows A, Sheehan NJ (2005). Prescribing and injecting:
Acknowledgements
The expanding role of the rheumatology nurse.
We would like to thank all participants of the survey, the Musculoskeletal Care 3: 176–8.
translators Elzbieta Bobiatynska, Walter Grassi, Jana Miles K, Seitio O, McGilvray M (2006). Nurse prescribing
Korandova, Katti Korve, Marja‐Leena Kukkurainen, in low‐resource settings: Professional considerations.
Maria Matheou, Serge Perrot, Ruta Sargautyte, Pereira International Nursing Review 53: 290–6.
de Silva and Jenny de la Torre, who translated the survey Ryan S, Hassell AB, Lewis M, Farrell A (2006). Impact of a
rheumatology expert nurse on the wellbeing of patients
into the different languages, and the EULAR secretariat
attending a drug monitoring clinic. Journal of Advanced
(Anja Schönbächler and Caroline Pasche) for their help
Nursing 53: 277–86.
and support in the present project, and EULAR for partly
Stamm T, Van der Giesen F, Thorstensson C, Steen E,
funding this project. Birrell F, Bauernfeind B, Marshall N, Prodinger B,
Machold K, Smolen J, Kloppenburg M (2009). Patient
REFERENCES perspective of hand osteoarthritis in relation to
concepts covered by instruments measuring function-
Cusick A, Johnson L, Bissett M (2009). Occupational
ing: A qualitative European multicentre study. Annals
therapy in emergency departments: Australian practice.
of the Rheumatic Diseases 68: 1453–60.
Journal of Evaluation in Clinical Practice 15: 257–65.
Thwaites C (2004). Rheumatology telephone advice lines.
Dahaghin S, Bierma‐Zeinstra SM, Ginai AZ, Pols HA,
Musculoskeletal Care 2: 120–6.
Hazes JM, Koes BW (2005a). Prevalence and pattern of
World Health Organization (2004). The World Health
radiographic hand osteoarthritis and association with
Report 2004. Available at http://www.who.int/whr/
pain and disability (the Rotterdam study). Annals of the
2004/en/ (Accessed 20 August 2010).
Rheumatic Diseases 64: 682–7.
Musculoskelet. Care (2011) © 2011 John Wiley & Sons, Ltd.