1. info@audiology.asn.au 43 Audiology Now 63
EMILY JEFFREYS
Tim Raynor Audiology,
Warrnambool, Victoria
HISTORY
A 3.5year old boy was referred to our
clinic in January 2015 by the local
speech therapist, who had concerns
regarding speech and language delays.
The child presented with his mother
who did not have any major concerns
regarding her child's hearing. VIHSP
screening was reported as being
passed. The child did however have
major risk factors associated with
pregnancy and birth.
• Born at 31 weeks
• Birth weight 1.8kg
• Special care nursery for 39 days
• Oxygen for 10 days
• IV antibiotics
• Jaundice under lights for 4-5 days
however no blood transfusion.
The child had otherwise been well
since then and his physical
development was on track.
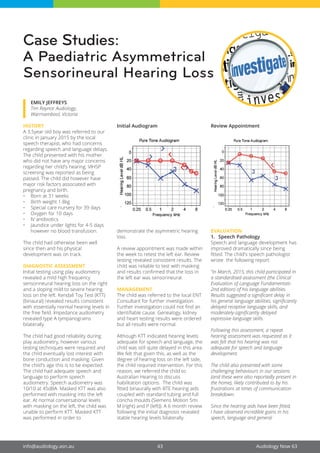
DIAGNOSTIC ASSESSMENT
Initial testing using play audiometry
revealed a mild high frequency
sensorineural hearing loss on the right
and a sloping mild to severe hearing
loss on the left. Kendall Toy Test (KTT)
(binaural) revealed results consistent
with essentially normal hearing levels in
the free field. Impedance audiometry
revealed type A tympanograms
bilaterally.
The child had good reliability during
play audiometry, however various
testing techniques were required and
the child eventually lost interest with
bone conduction and masking. Given
the child's age this is to be expected.
The child had adequate speech and
language to perform speech
audiometry. Speech audiometry was
10/10 at 45dBA. Masked KTT was also
performed with masking into the left
ear. At normal conversational levels
with masking on the left, the child was
unable to perform KTT. Masked KTT
was performed in order to
Initial Audiogram
demonstrate the asymmetric hearing
loss.
A review appointment was made within
the week to retest the left ear. Review
testing revealed consistent results. The
child was reliable to test with masking
and results confirmed that the loss in
the left ear was sensorineural.
MANAGEMENT
The child was referred to the local ENT
Consultant for further investigation.
Further investigation could not find an
identifiable cause. Genealogy, kidney
and heart testing results were ordered
but all results were normal.
Although KTT indicated hearing levels
adequate for speech and language, the
child was still quite delayed in this area.
We felt that given this, as well as the
degree of hearing loss on the left side,
the child required intervention. For this
reason, we referred the child to
Australian Hearing to discuss
habilitation options. The child was
fitted binaurally with BTE hearing aids
coupled with standard tubing and full
concha moulds (Siemens Motion 5mi
M (right) and P (left)). A 6 month review
following the initial diagnosis revealed
stable hearing levels bilaterally.
Review Appointment
EVALUATION
1. Speech Pathology
Speech and language development has
improved dramatically since being
fitted. The child's speech pathologist
wrote the following report:
“In March, 2015, this child participated in
a standardised assessment (the Clinical
Evaluation of Language Fundamentals-
2nd edition) of his language abilities.
Results suggested a significant delay in
his general language abilities, significantly
delayed receptive language skills, and
moderately-significantly delayed
expressive language skills.
Following this assessment, a repeat
hearing assessment was requested as it
was felt that his hearing was not
adequate for speech and language
development.
The child also presented with some
challenging behaviours in our sessions
(and these were also reportedly present in
the home), likely contributed to by his
frustrations at times of communication
breakdown.
Since the hearing aids have been fitted,
I have observed incredible gains in his
speech, language and general
Case Studies:
A Paediatric Asymmetrical
Sensorineural Hearing Loss
audiologynow63 19/3/16 8:24 PM Page 43
2. Audiology Now 63 44 www.audiology.asn.au
participation. He has gone from using
1-2 word phrases 7-8 months ago to
becoming quite proficient in using
Colourful Semantics to piece together 4-6
word phrases independently His attitude
towards speech pathology is much more
positive, and his turn-taking, sharing, and
joint attention has improved markedly.
His speech sound production is also now
largely age-appropriate. “
2. Audiology
The child continued to attend our clinic
for on-going assessment and continuity
of care. My concern as the first clinician
to see the child was to ensure positive
long term outcomes, particularly for
speech and language.
His mother reports that she is delighted
with his progress and improvements. In
addition, he is now more confident,
outgoing and happy at home and at
kinder or on play dates. His mother is
delighted that he has accepted the aids
readily and wears them at all times. She
does not have any problems with aid
management.
The P.E.A.C.H test was administered as
a formal tool to gauge the parents'
view of aided progress. The Parent's
Evaluation of Aural/Oral Performance
of Children (P.E.A.C.H) asks 13
questions using a five point scale to
build a picture of the child's functional
performance in everyday life situations
(http://outcomes.nal.gov.au). Results
show a very positive approach to
hearing aids and mother reports he
wears the aids at all times. The overall
score of his listening behavior across a
range of hearing and communication
scenarios was 90.9%. The score for
quiet situations was 95.83% and for
more challenging noisy situations was
85%, which are very positive and
encouraging scores.
Australian Hearing has been
responsible for all technical aspects of
the aid fitting and for this reason
formal aid evaluation results (aided
testing, REM) are not reported here.
OUTCOME
The overall outcome of this study can
be summarized in a single line, by the
speech pathologist: This child is much
more confident now and he continues to
blow me away each week. As the initial
clinician it has been a rewarding and
positive experience for me to observe
the changes in auditory
responsiveness, hear him talk more
fluently and listen to the stories told
by his mother.
For sale
Acoustical
Design Booth
Large sound proof booth (approx. 3.7 x 3.4)
suitable for VROA. Currently dismantled into
transportable panels. Any offer considered.
Currently in Bella Vista, NSW. Own transport
must be organised.
Phone Lindsay Reinhardt on
0414 463 311
Above/ Emily testing a child at her clinic. This is a publicity picture and NOT the child
reported on in this article.
audiologynow63 20/3/16 9:42 PM Page 44