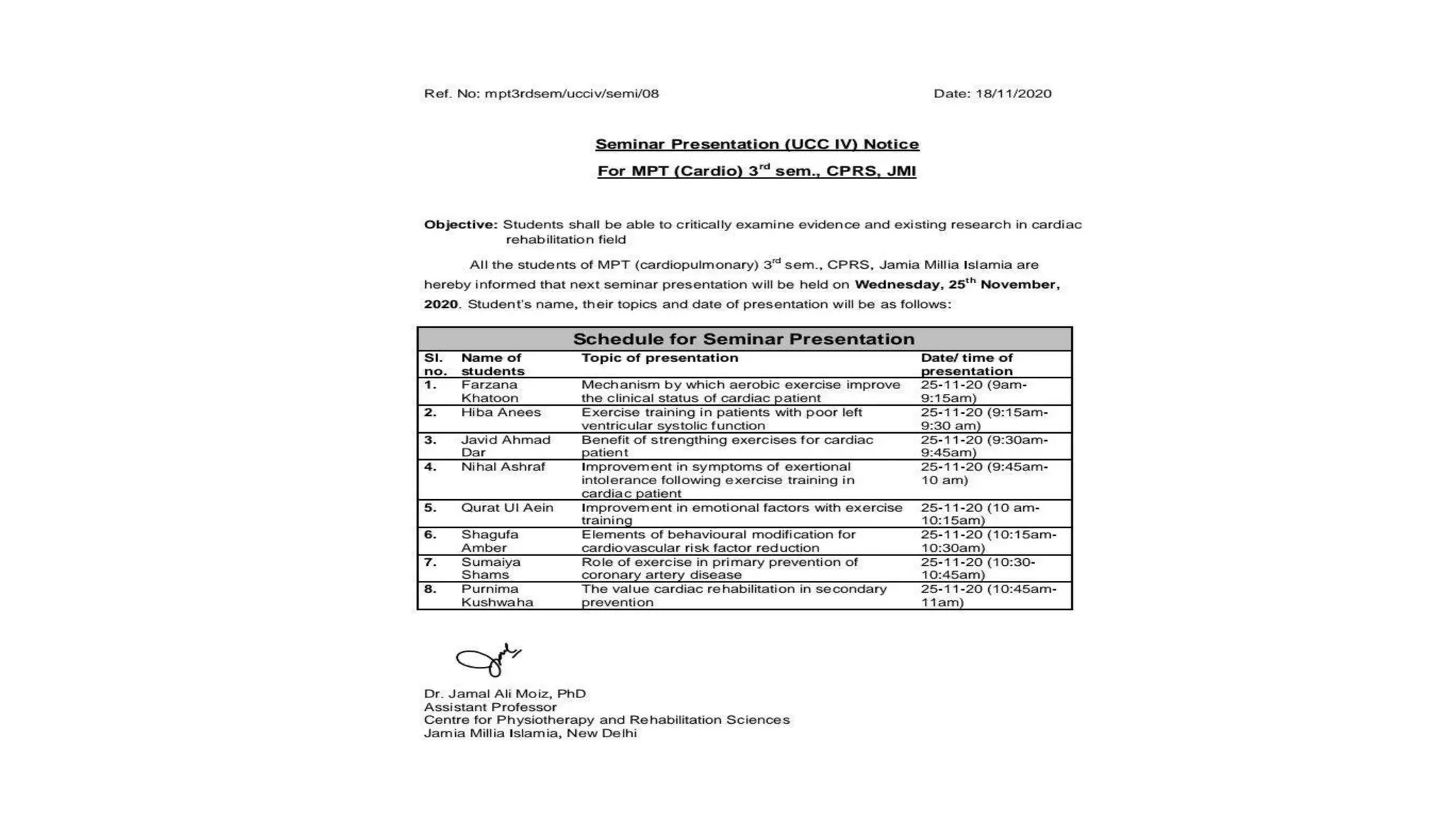
This document discusses 10 elements of behavioral modification for cardiovascular risk factor reduction. It outlines strategies for facilitating behavior change, including tailoring education to individual patient needs and characteristics, recognizing that knowledge alone is insufficient for change, promoting self-efficacy and control, assessing readiness to change, setting SMART goals, promoting independence through self-monitoring, providing feedback and rewards, creating environmental cues, engaging social support, and serving as a role model. The goal is to design sustainable programs that meet patients where they are and empower them to successfully adopt and maintain new health behaviors.