Downloaded 34 times

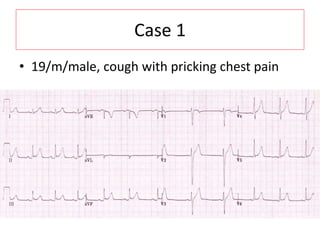
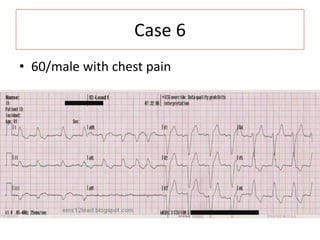

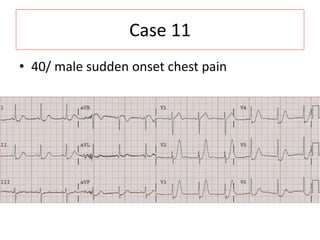

This document contains 12 ECG case studies with interpretations and discussions of important ECG findings: 1) Case 1 shows widespread ST elevation indicating diffuse subendocardial ischemia from severe 3 vessel disease. 2) Case 6 demonstrates T wave discordance, which is an important finding in the setting of left bundle branch block. 3) Case 11 shows de Winter T waves, which suggest an acute proximal LAD occlusion and are a high risk sign for anterior myocardial infarction.























































































