Downloaded 17 times
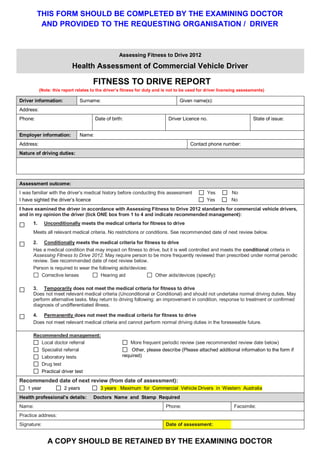
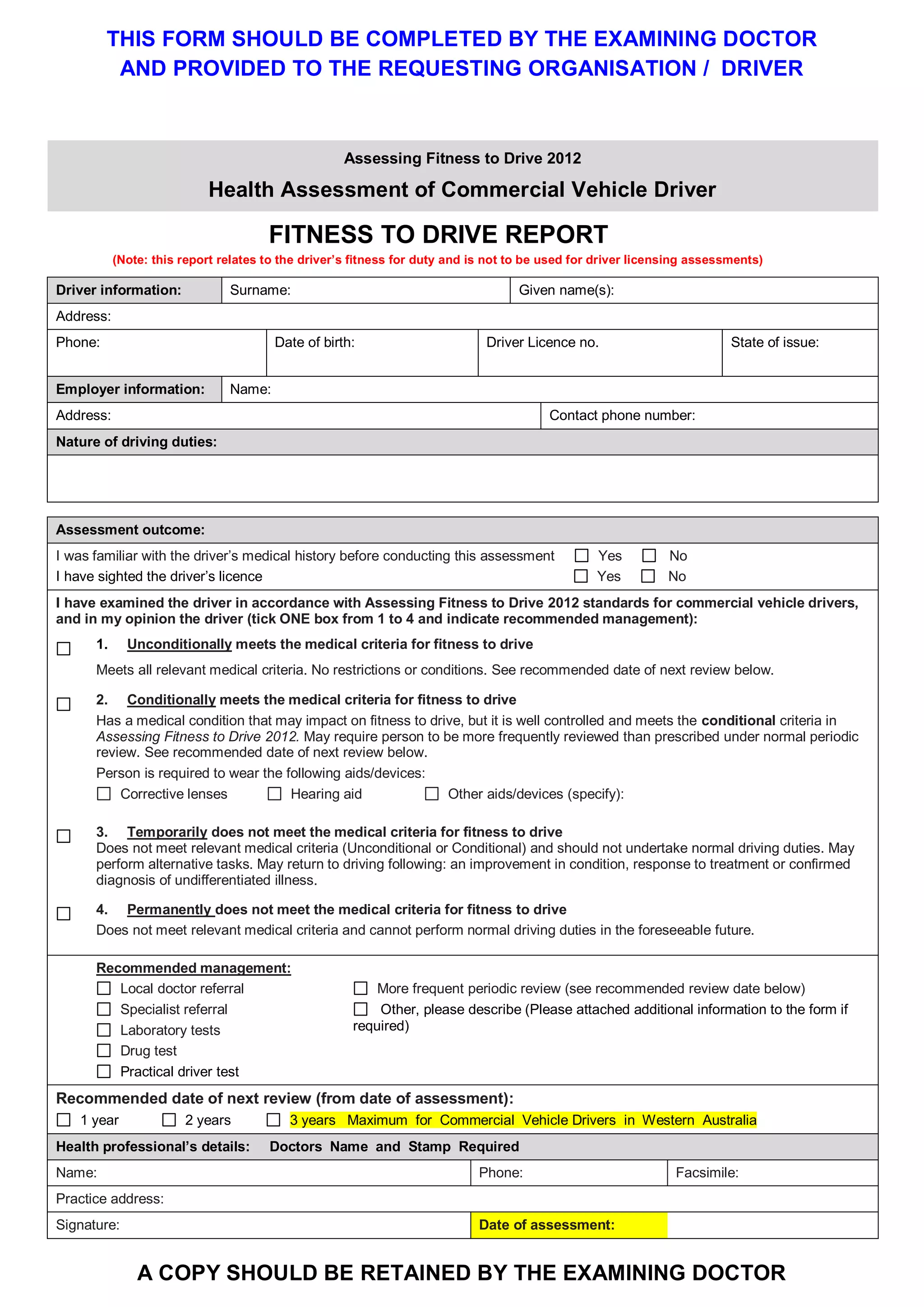

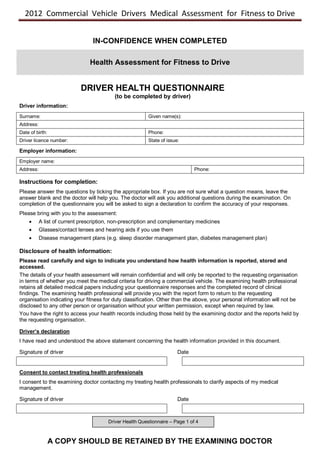





This document provides guidance for doctors conducting medical assessments of commercial vehicle drivers. It includes forms for doctors to complete as part of the assessment, including a driver health questionnaire, clinical assessment record, and fitness to drive report. The driver health questionnaire is used to screen for any medical conditions that could impact driving safety. The clinical assessment record guides the doctor in conducting and documenting the physical examination. It concludes with the doctor providing an opinion on the driver's medical fitness to drive on the fitness to drive report form.





















































