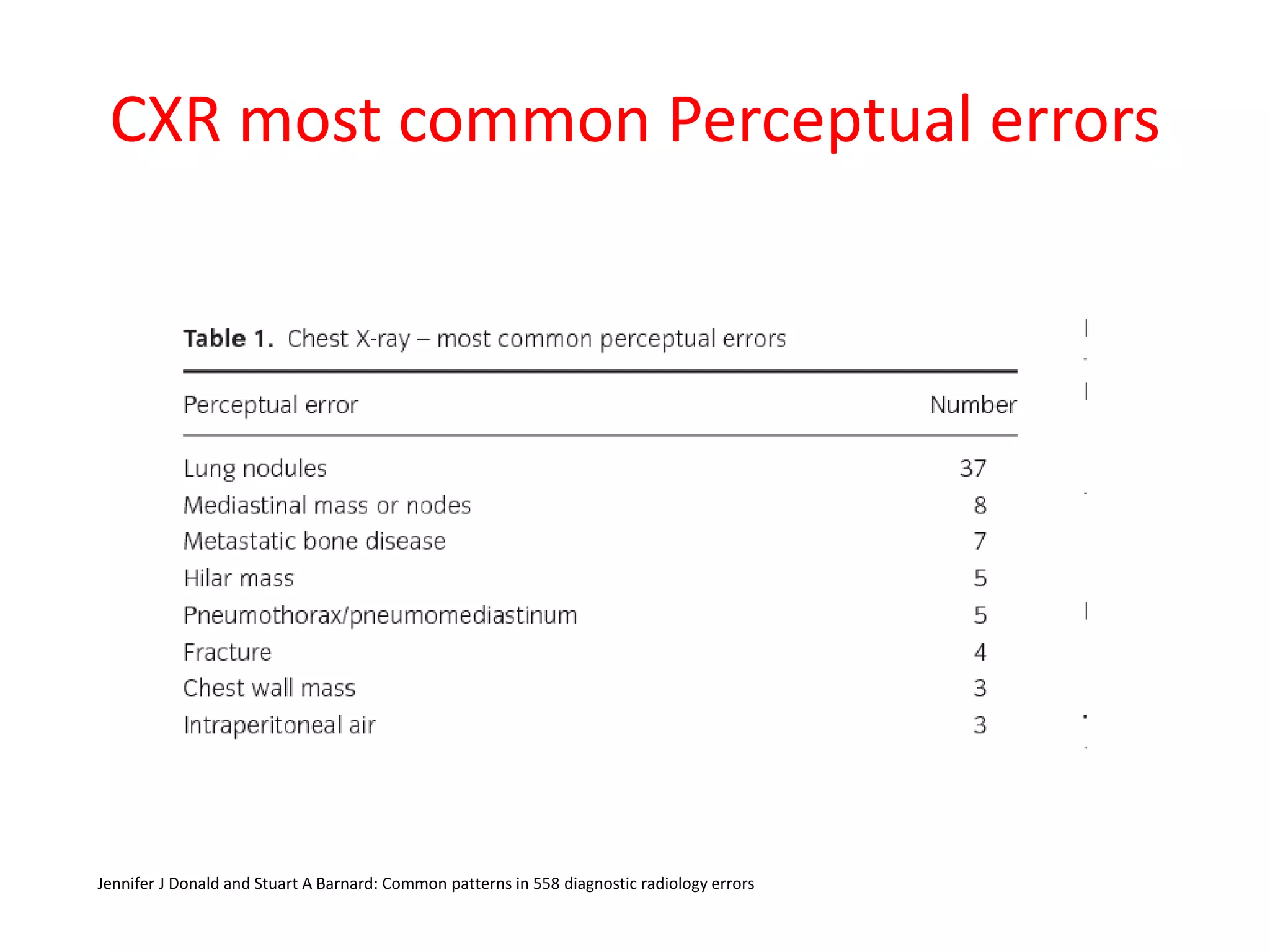
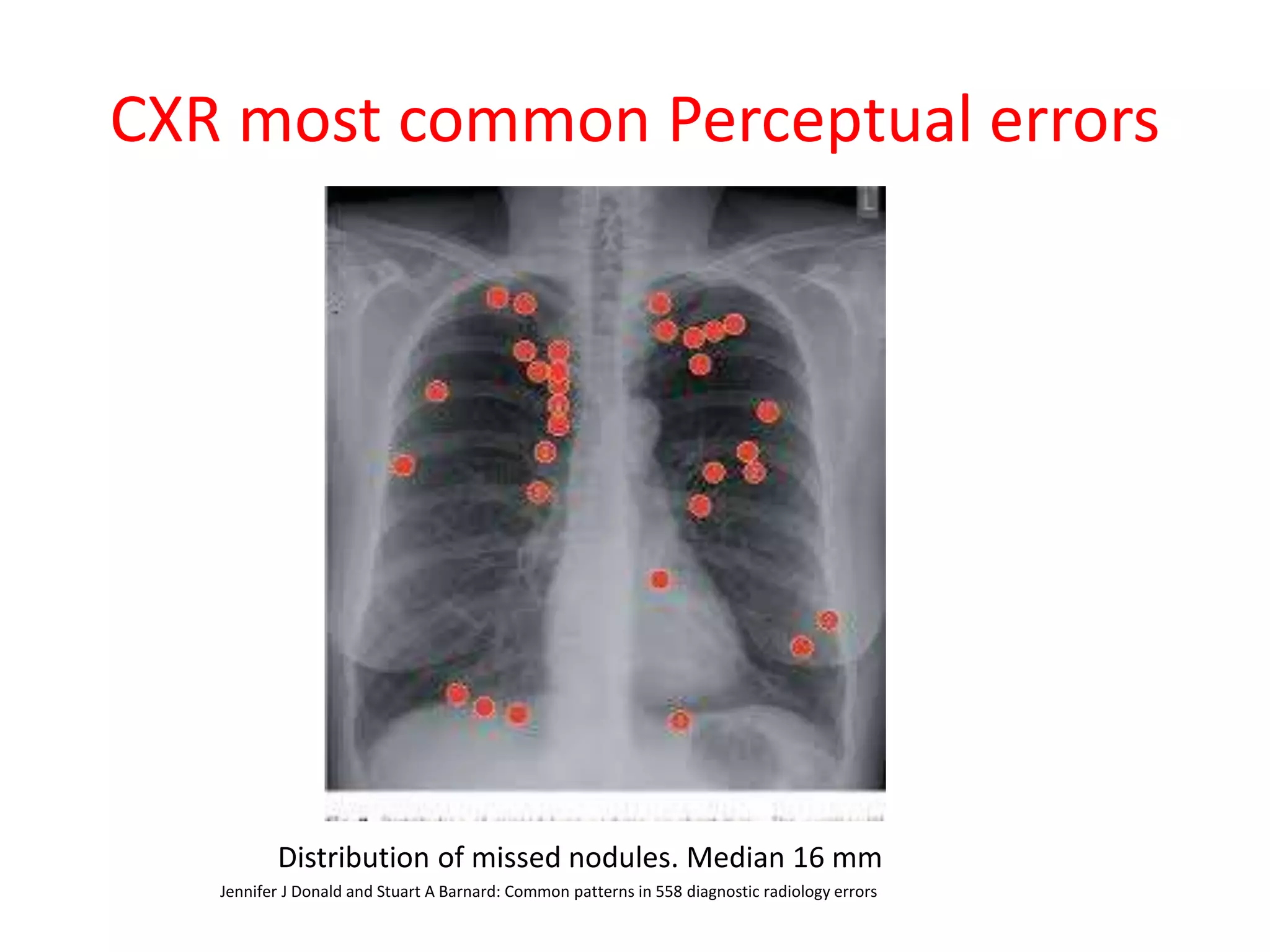
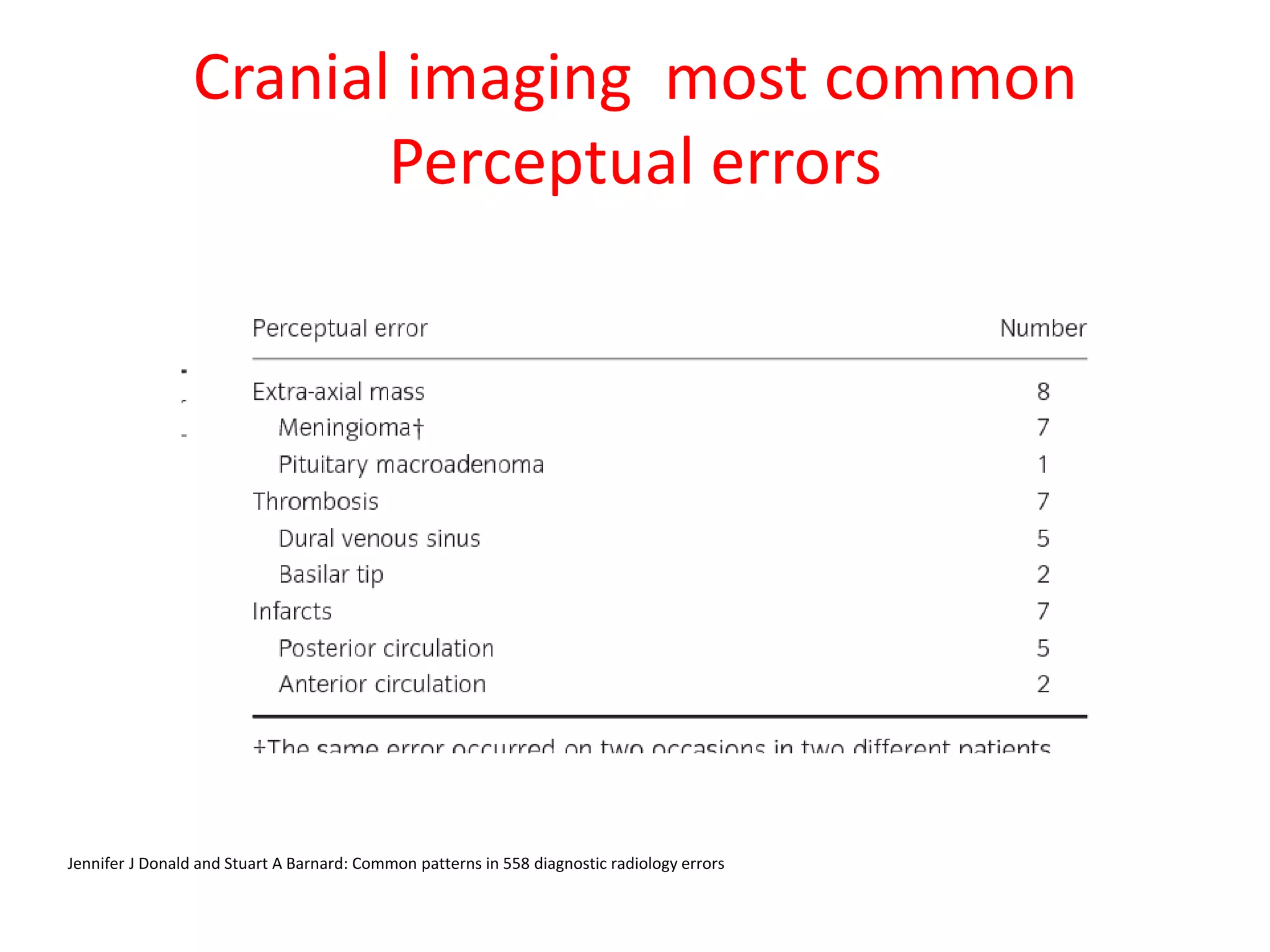
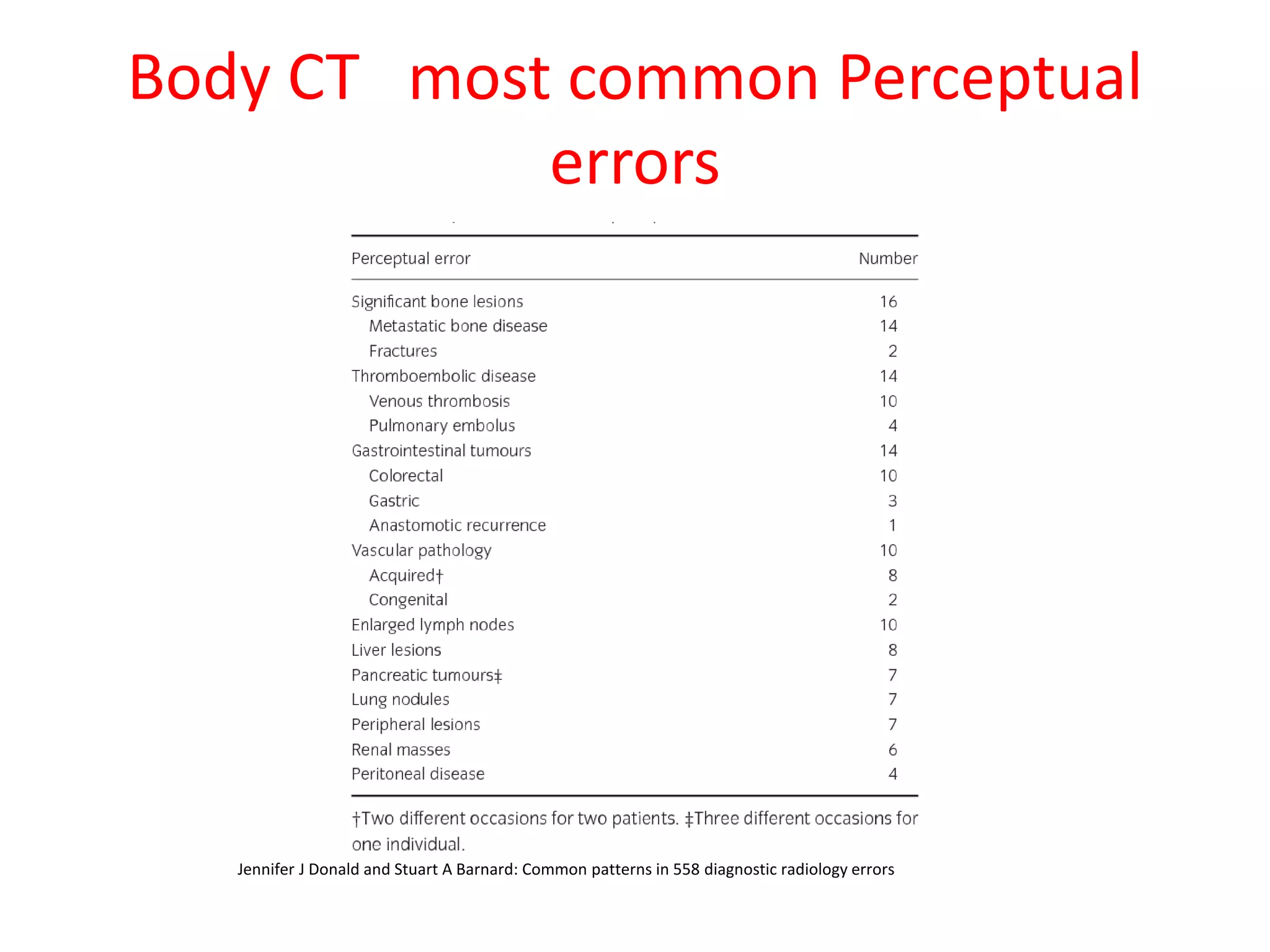
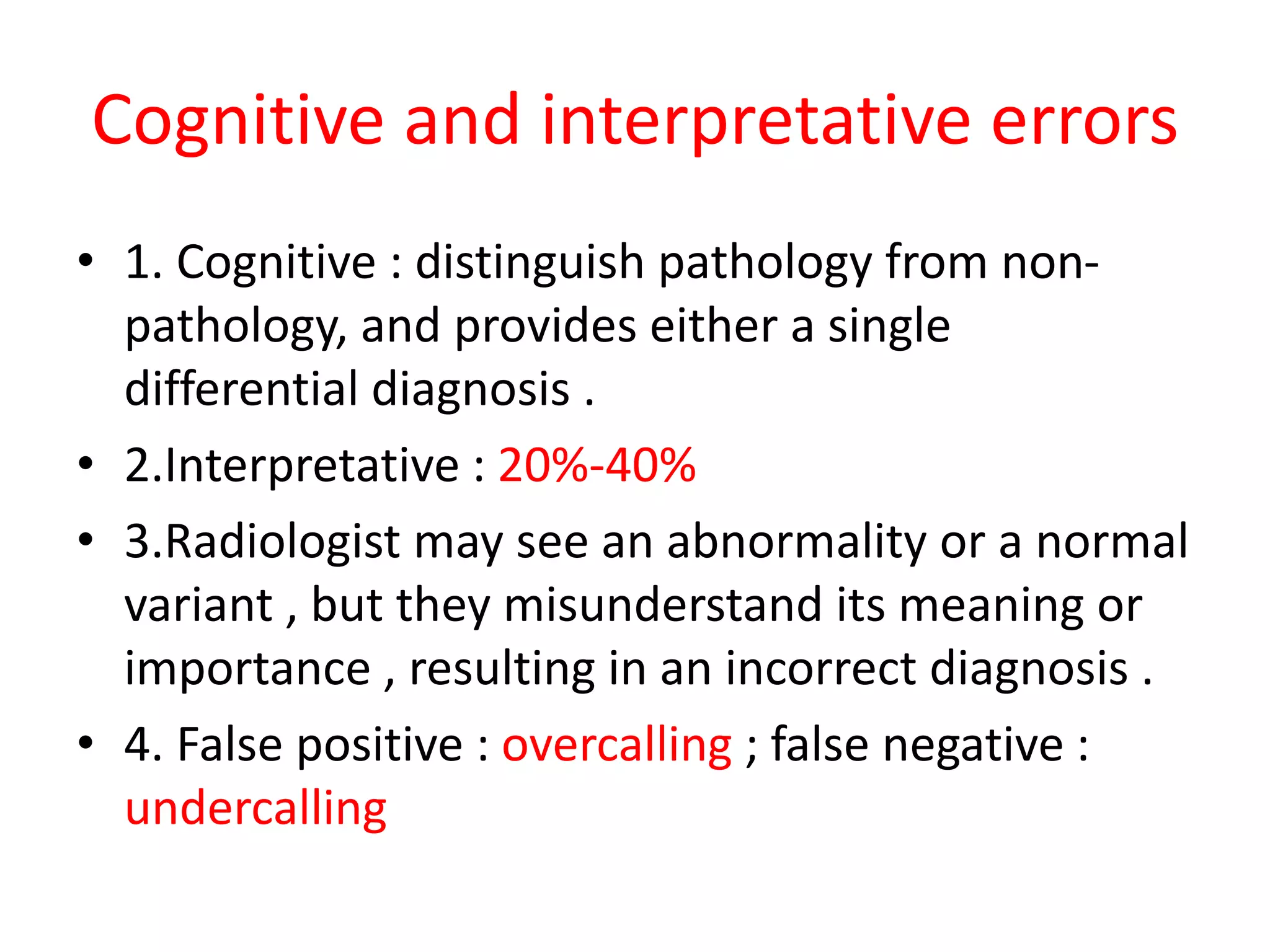
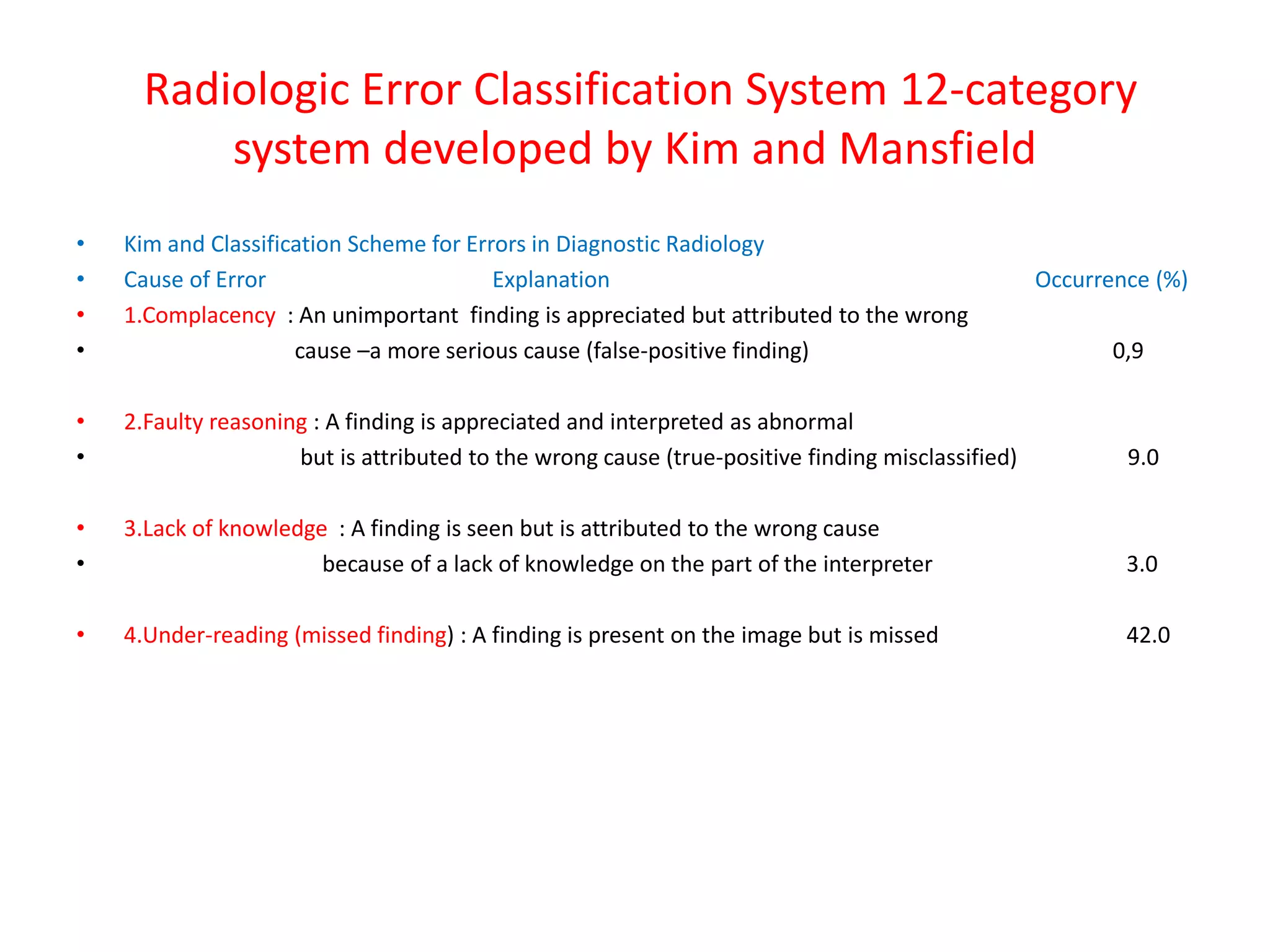
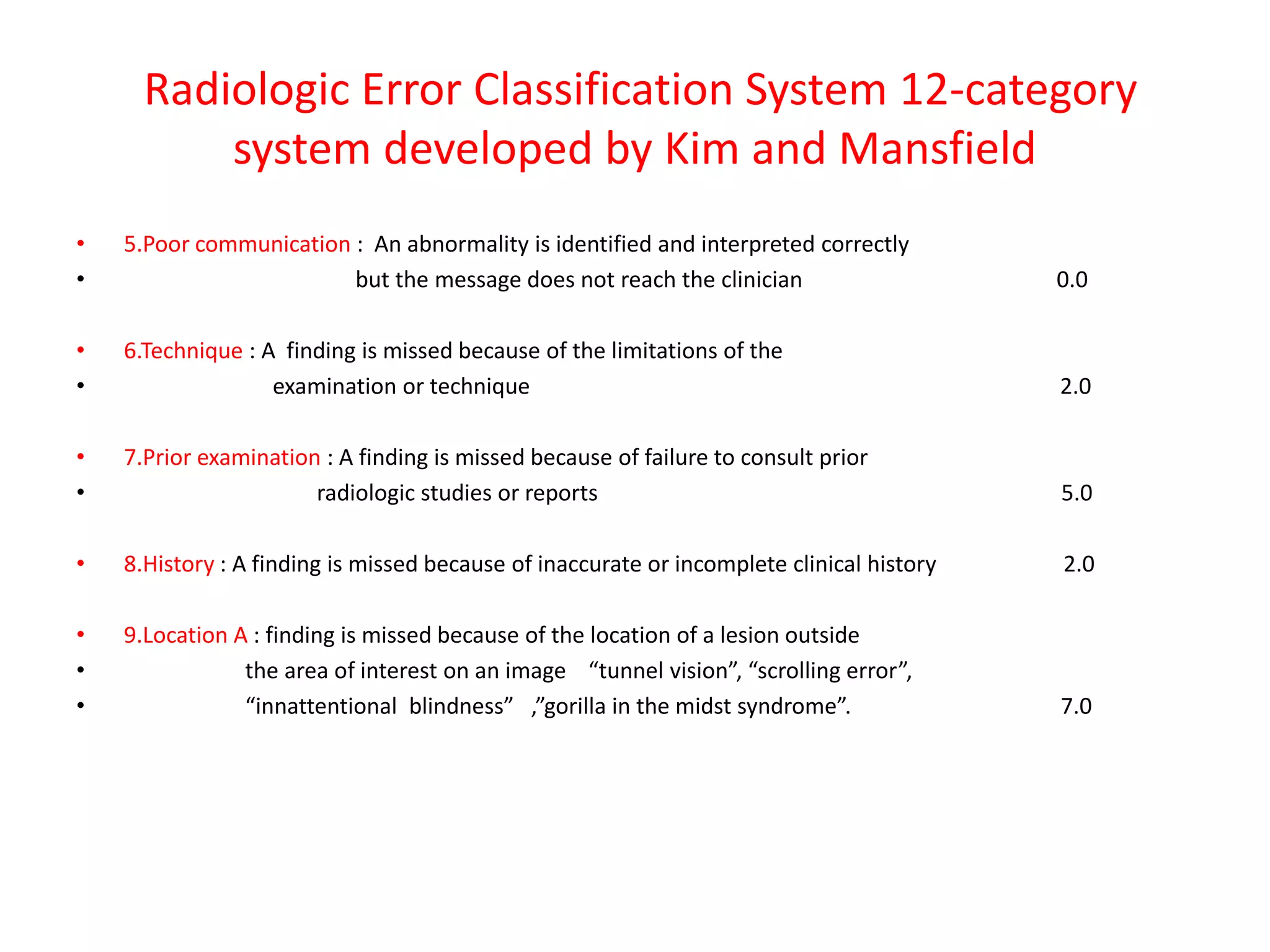
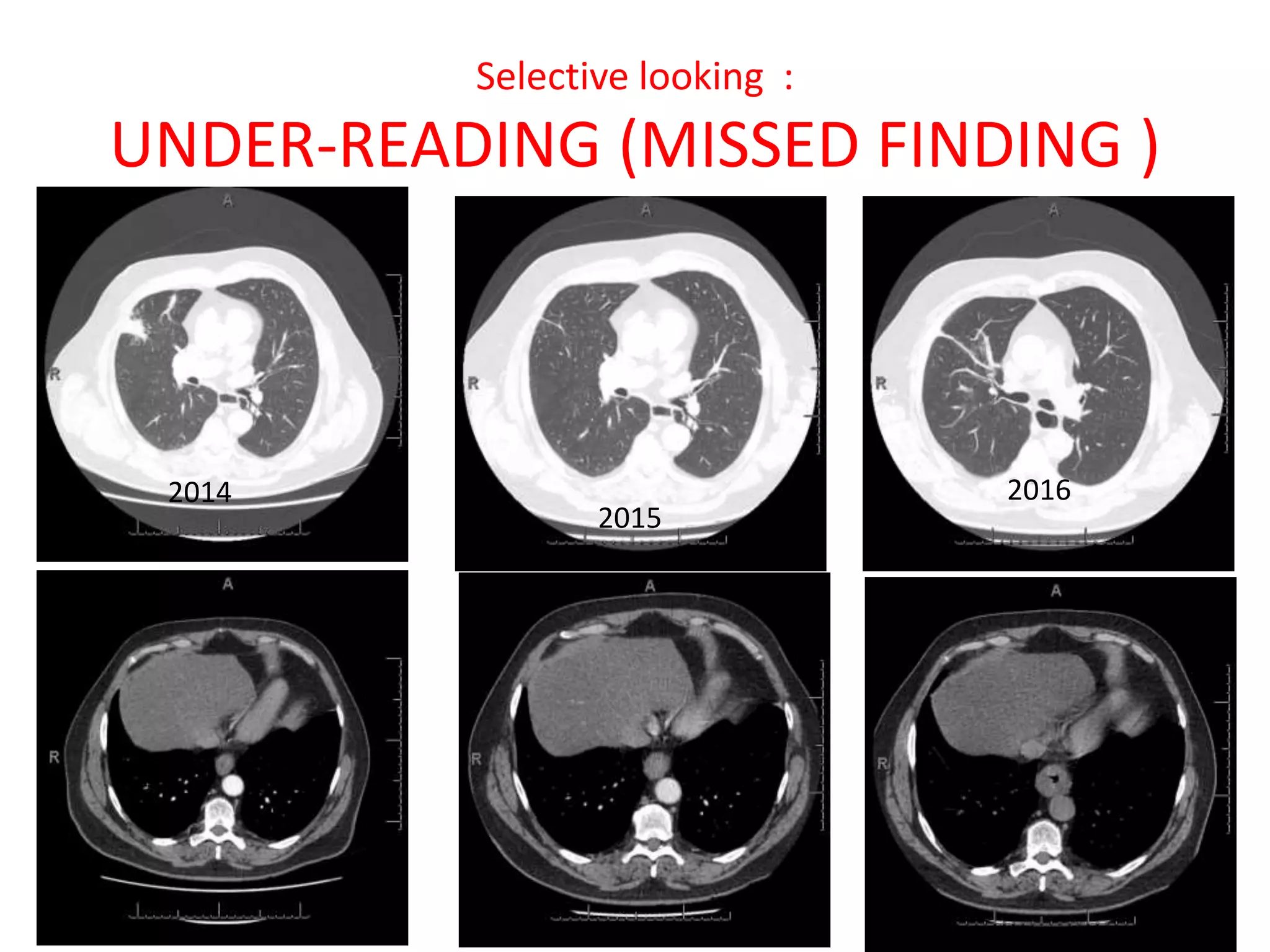
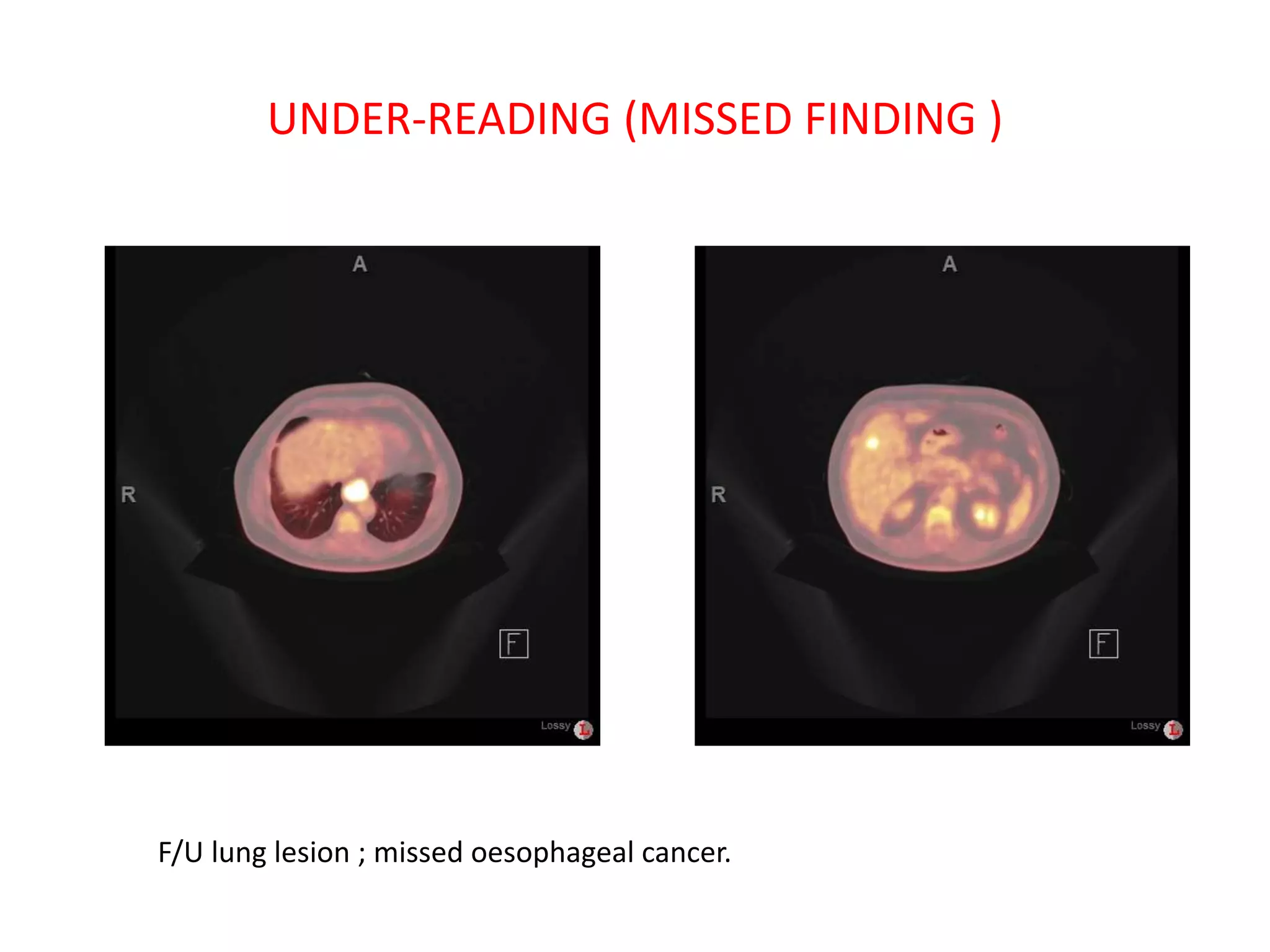
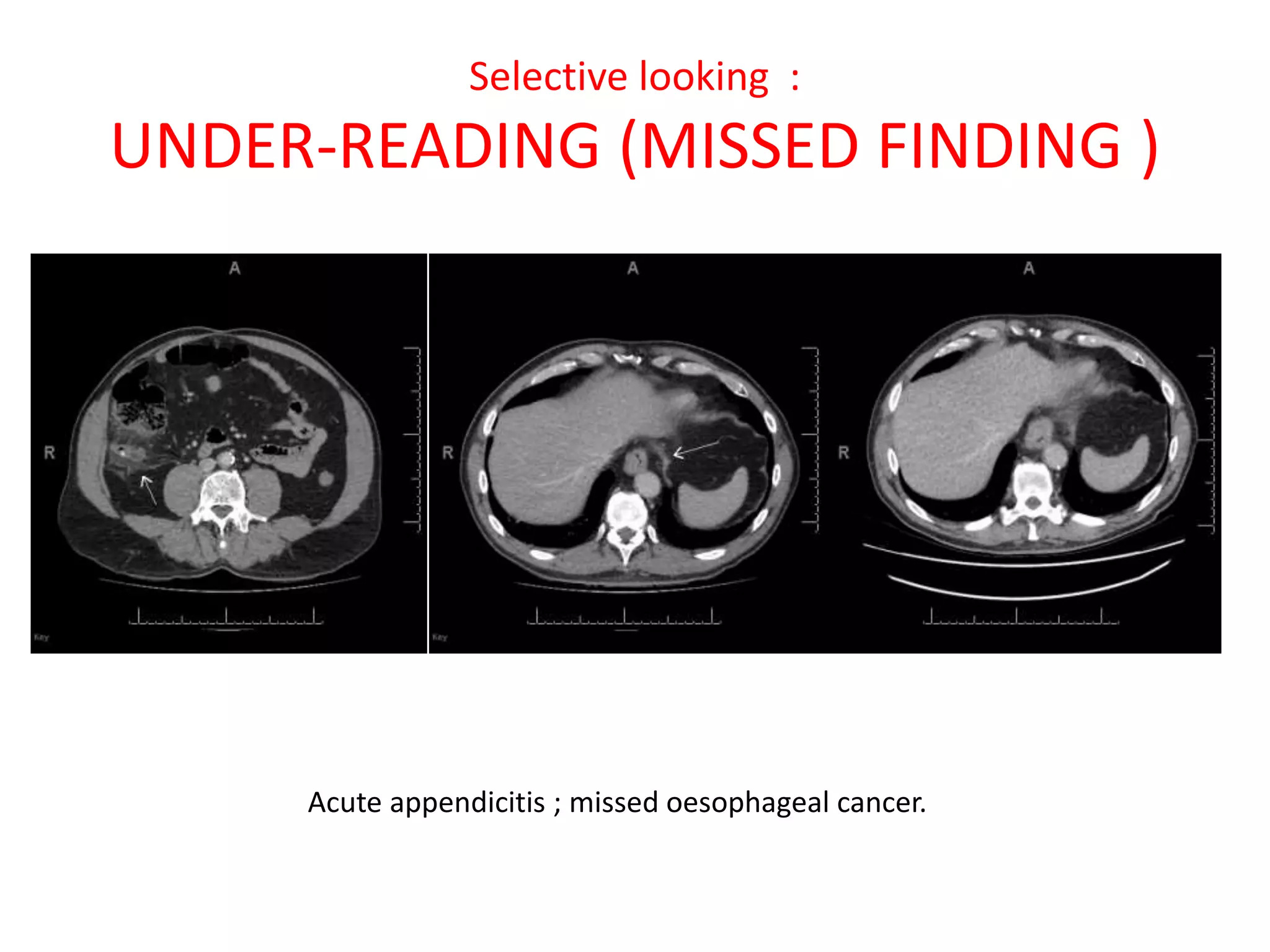
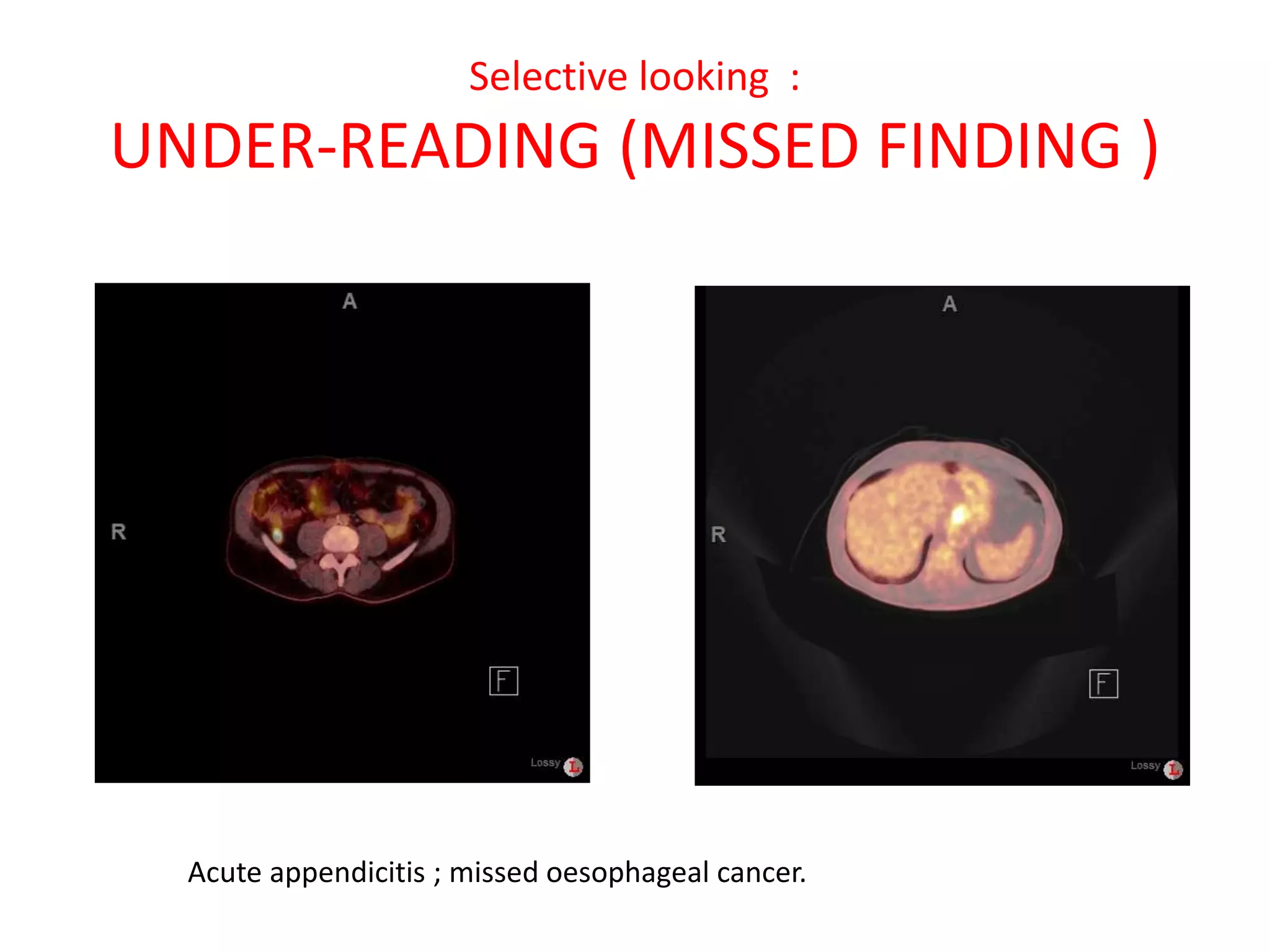
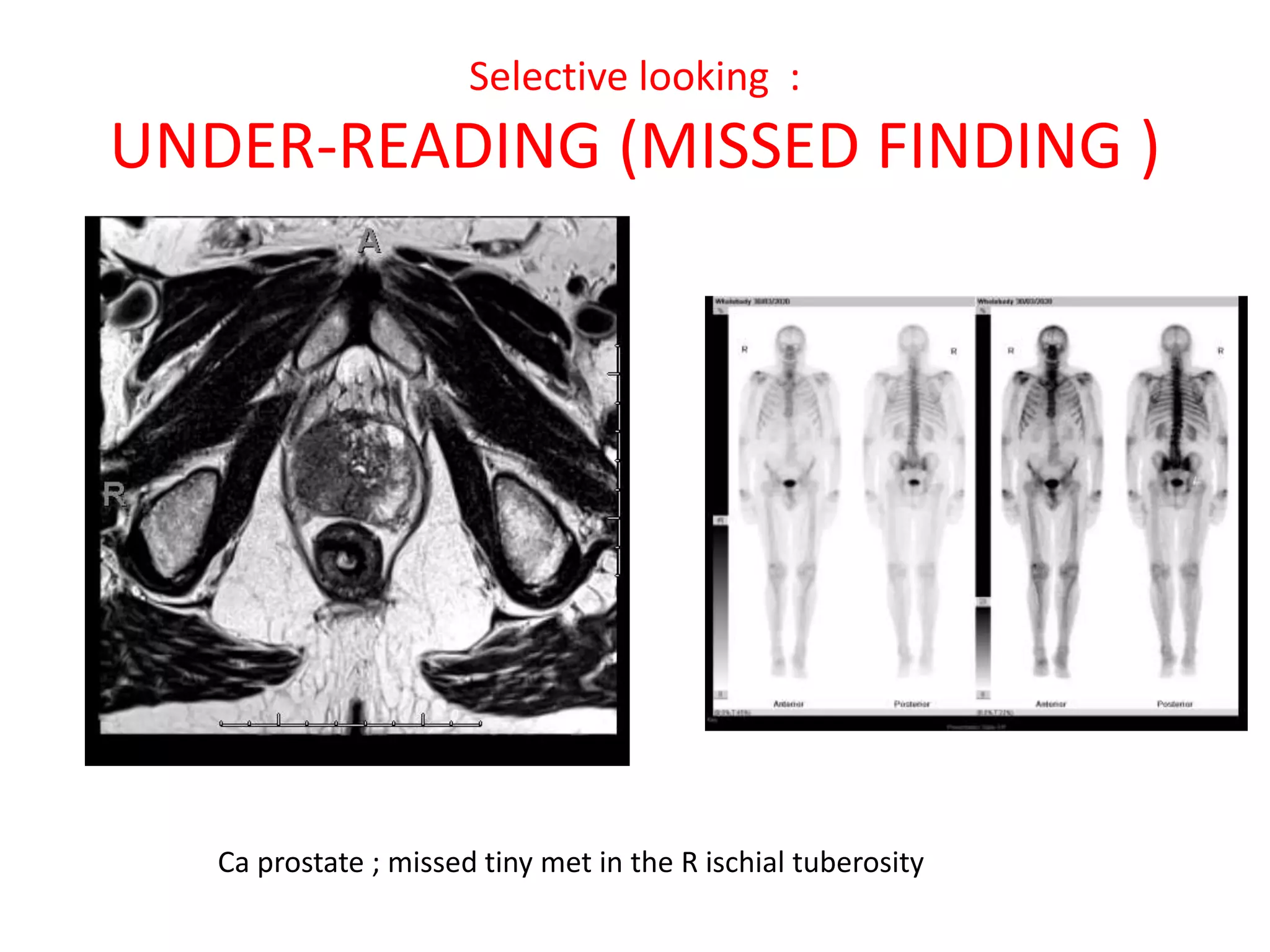
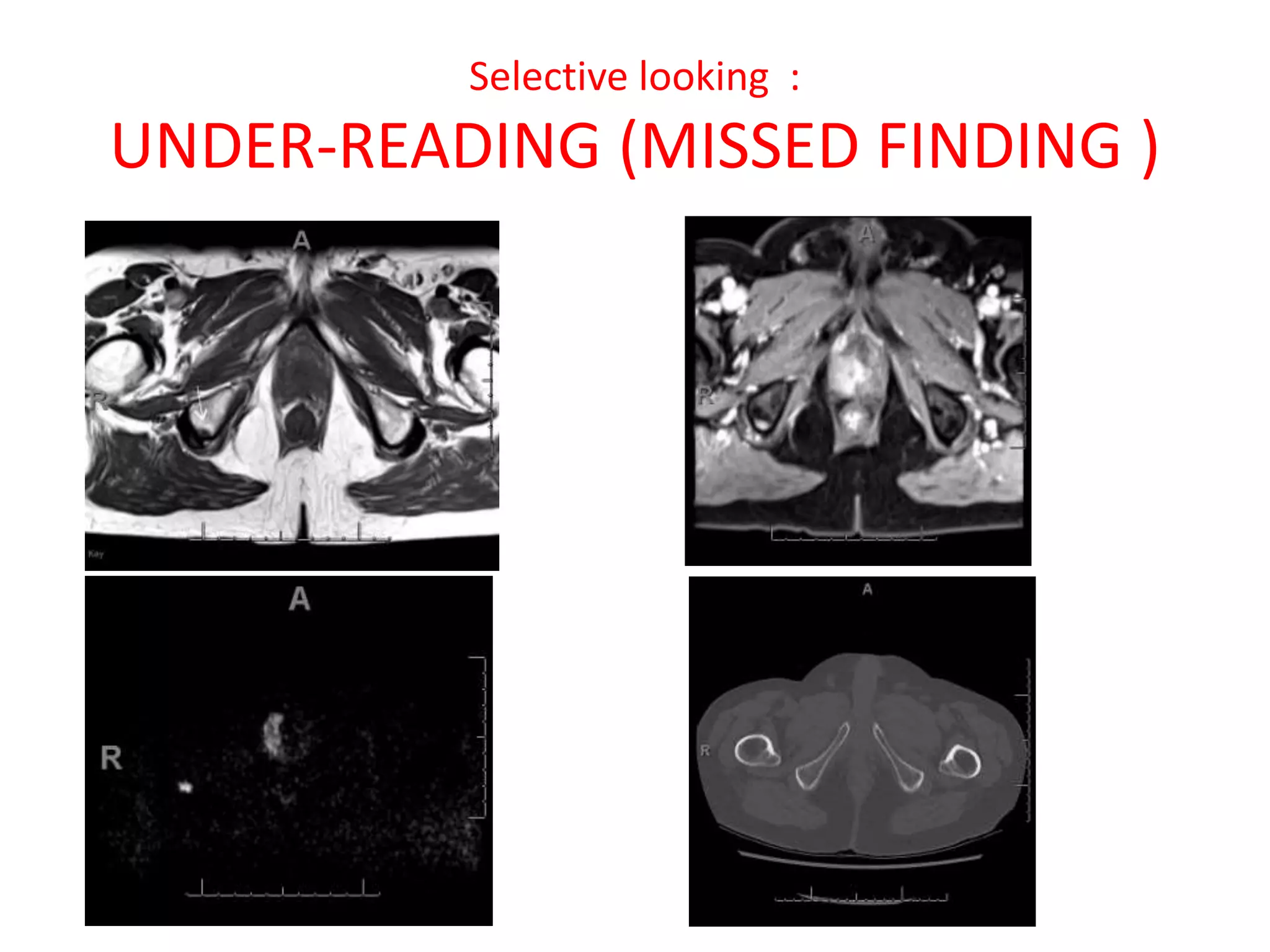
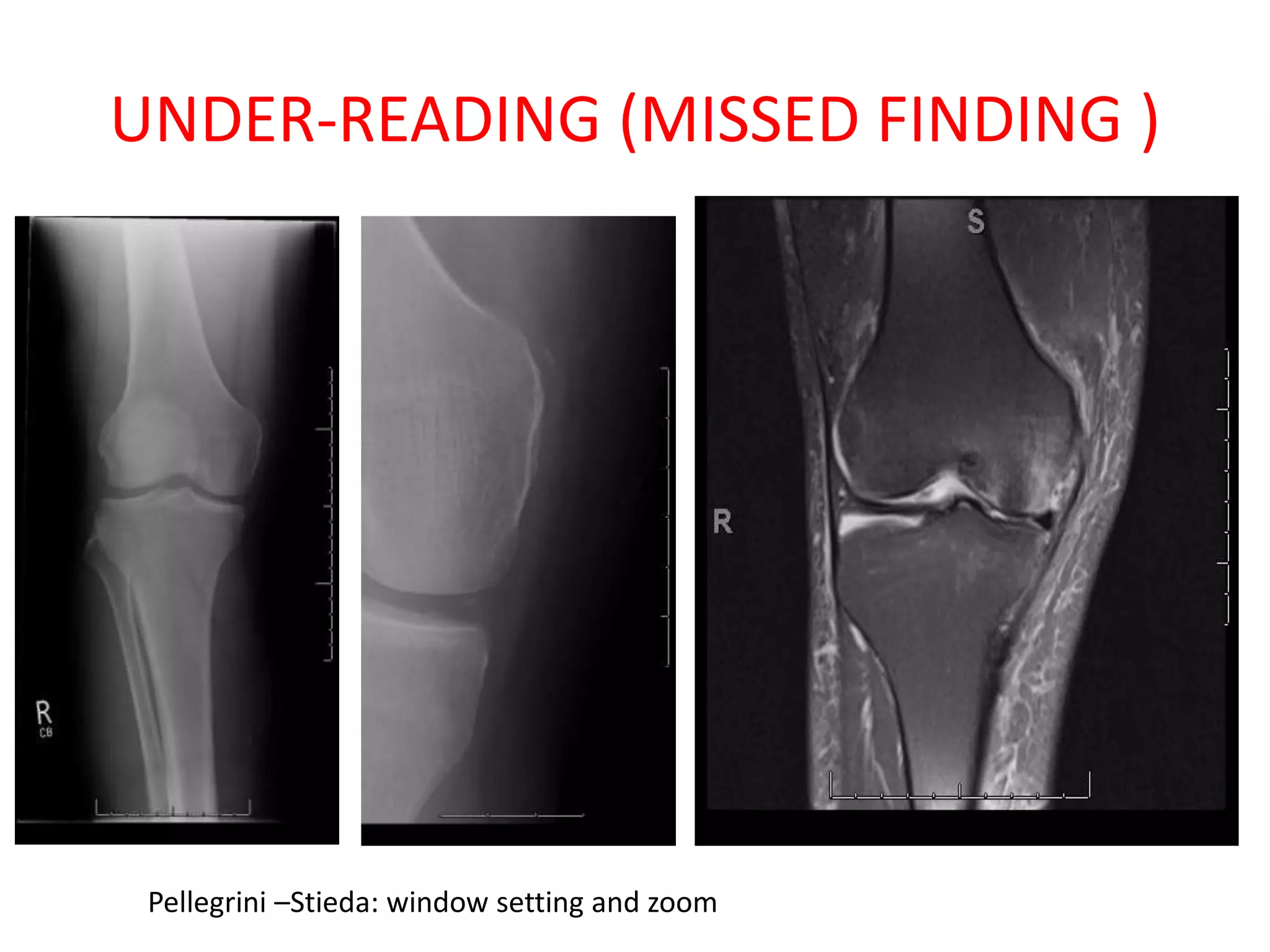
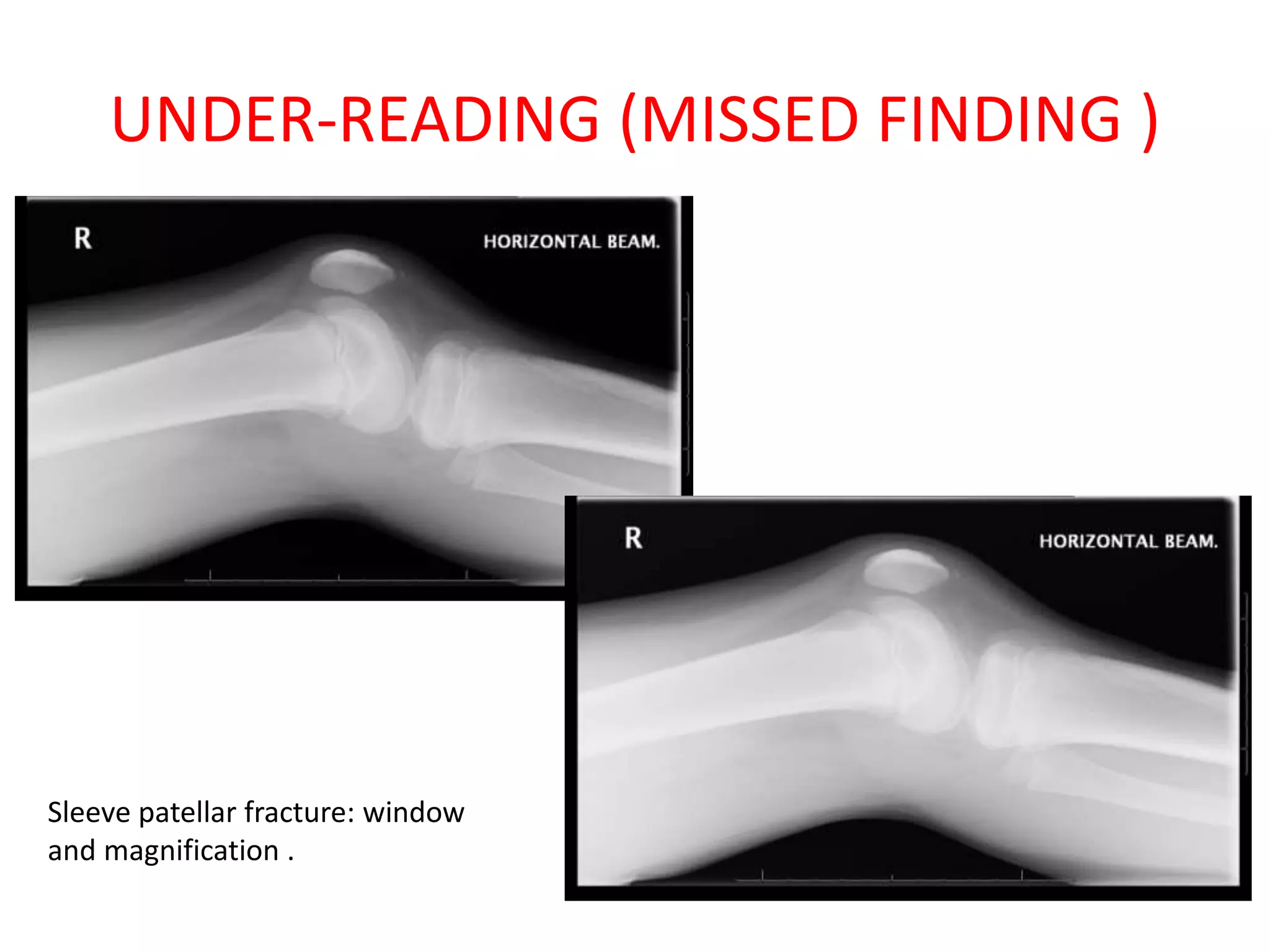
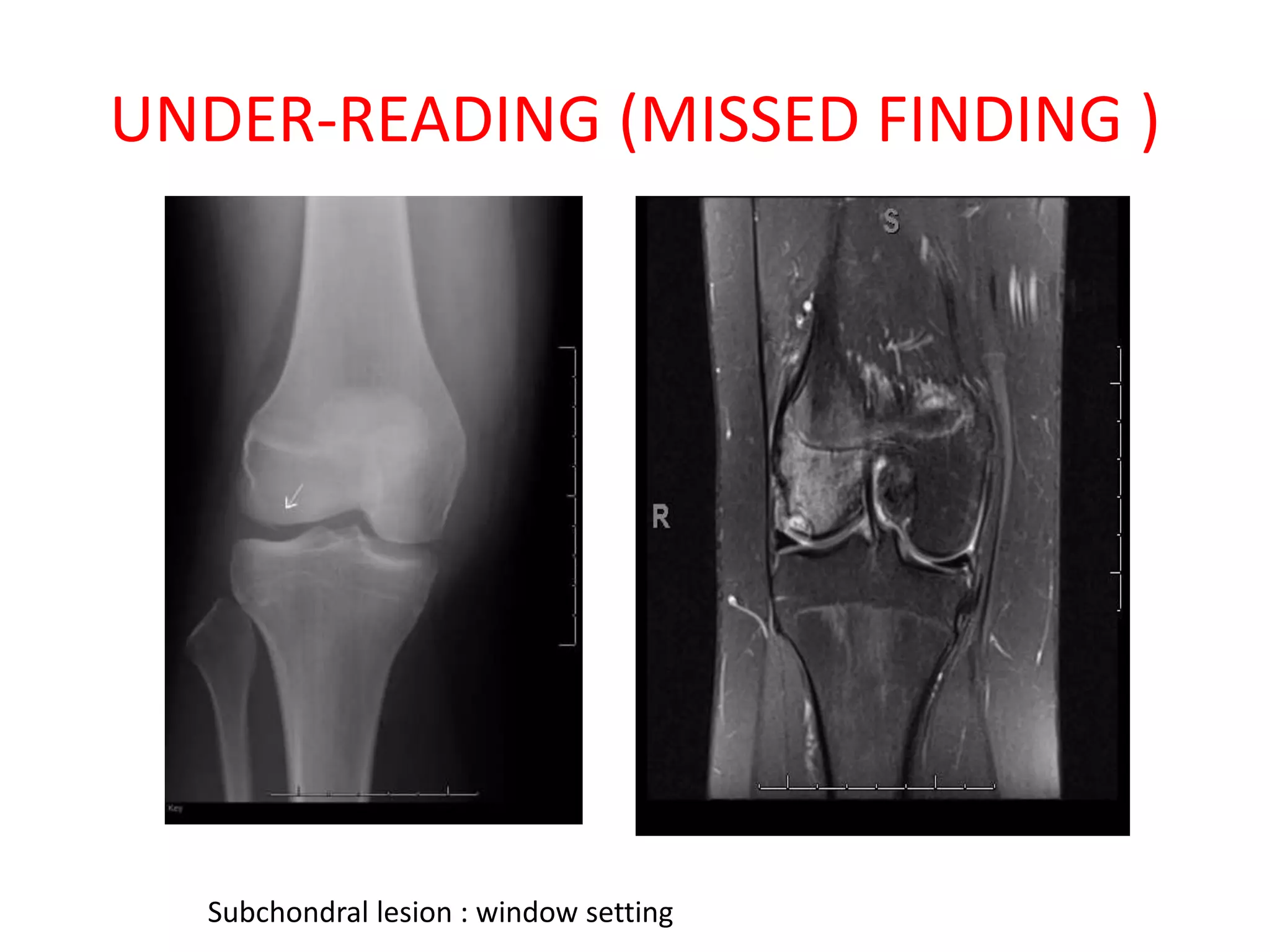
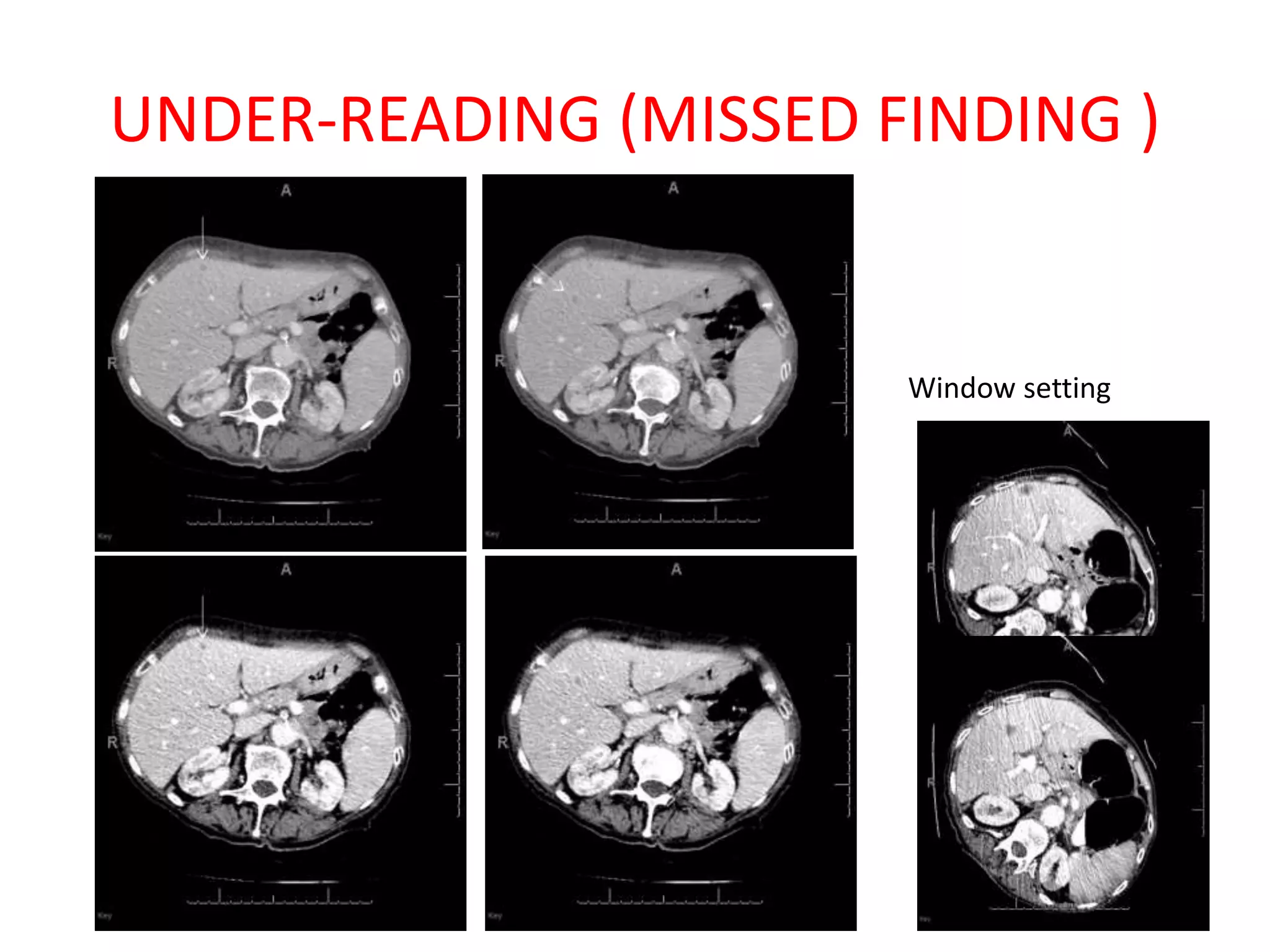
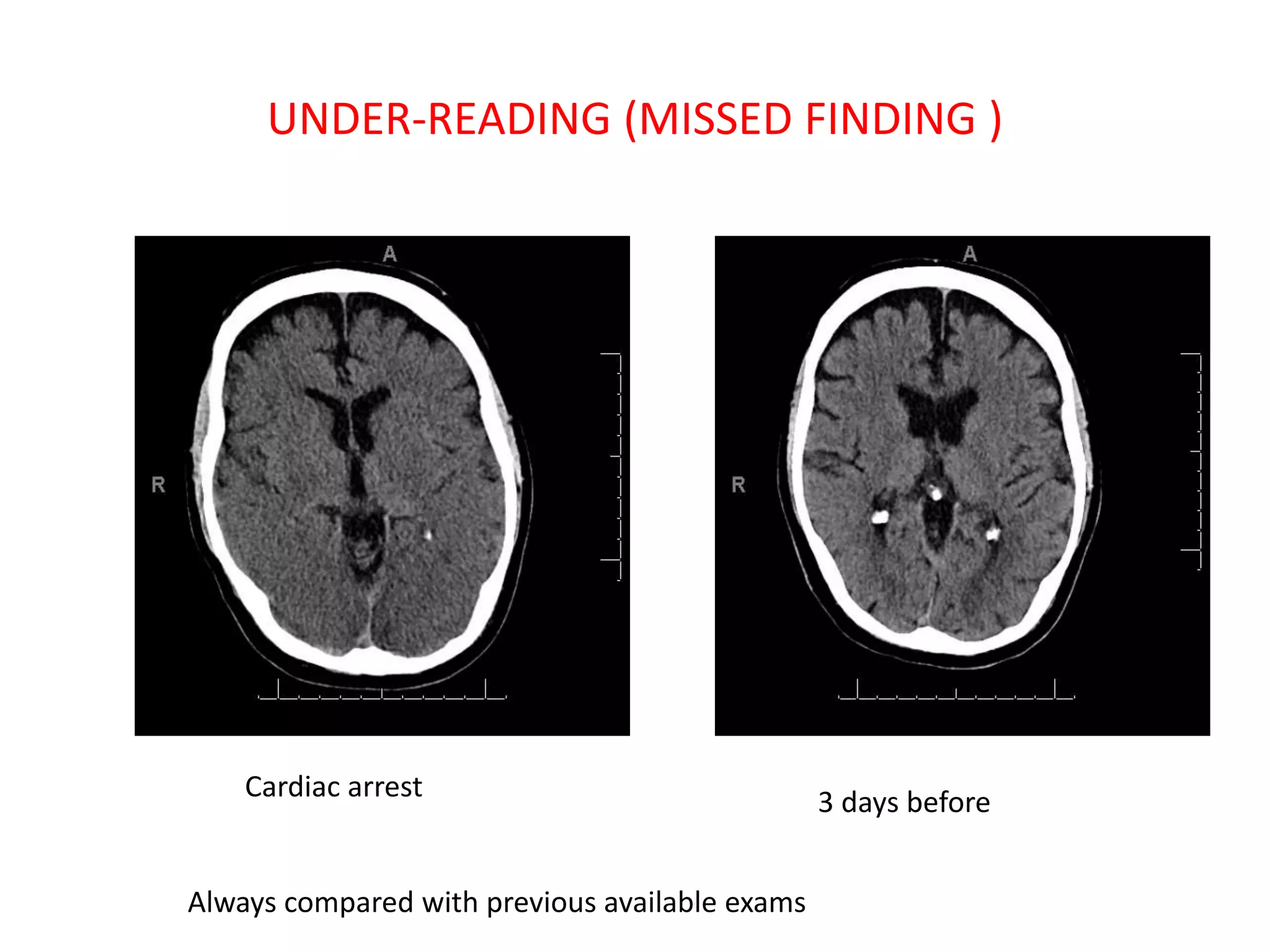
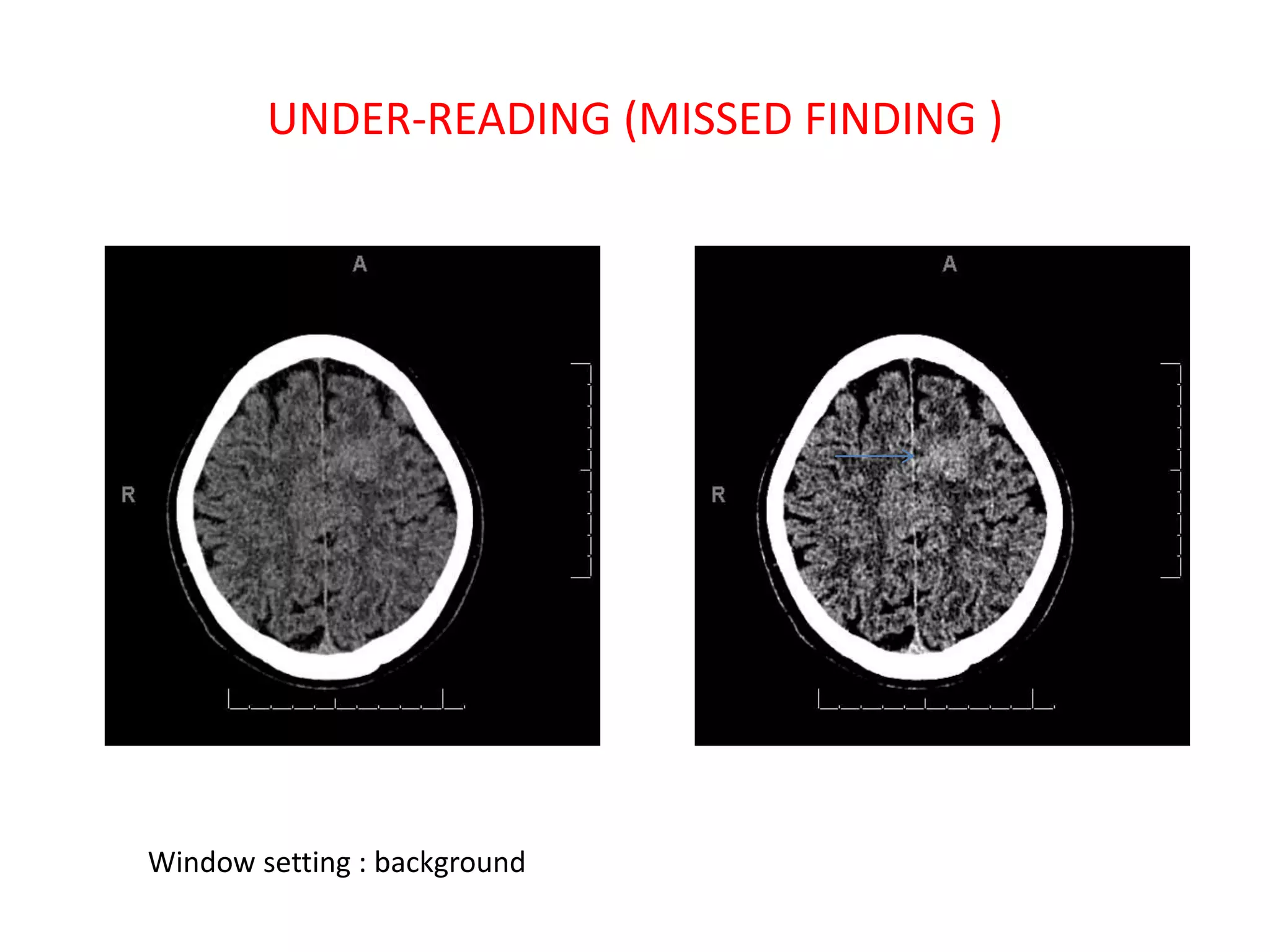
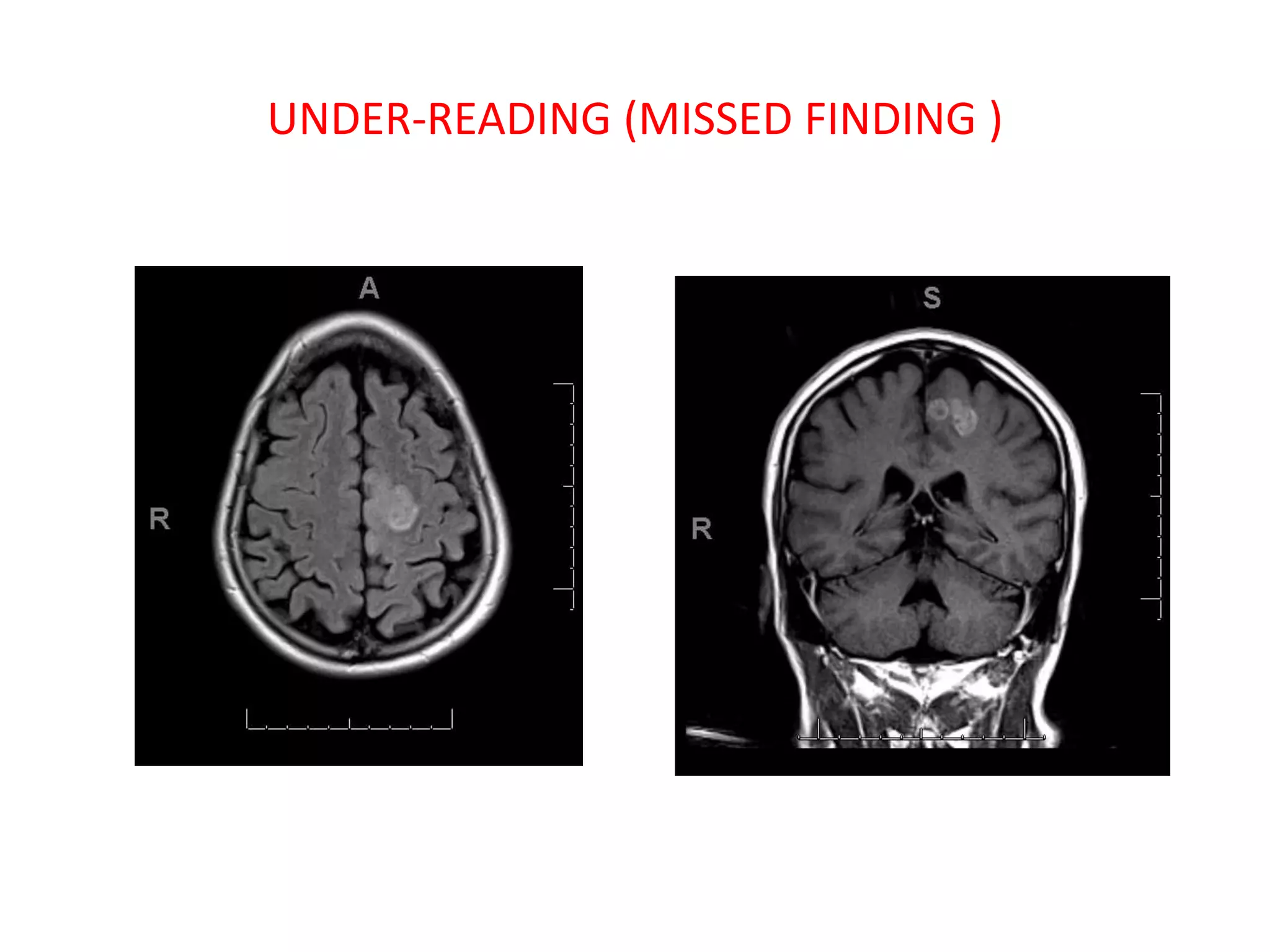
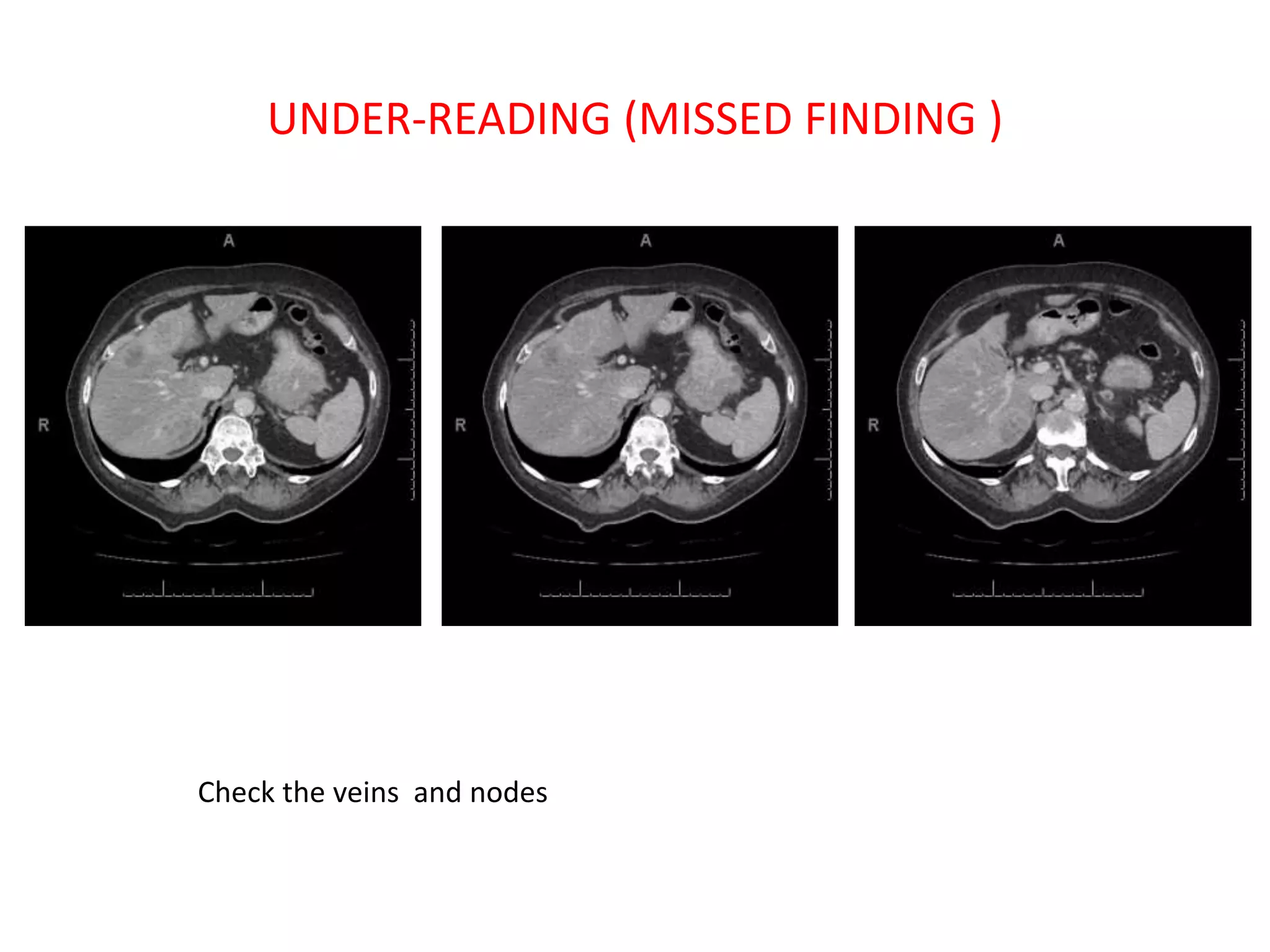
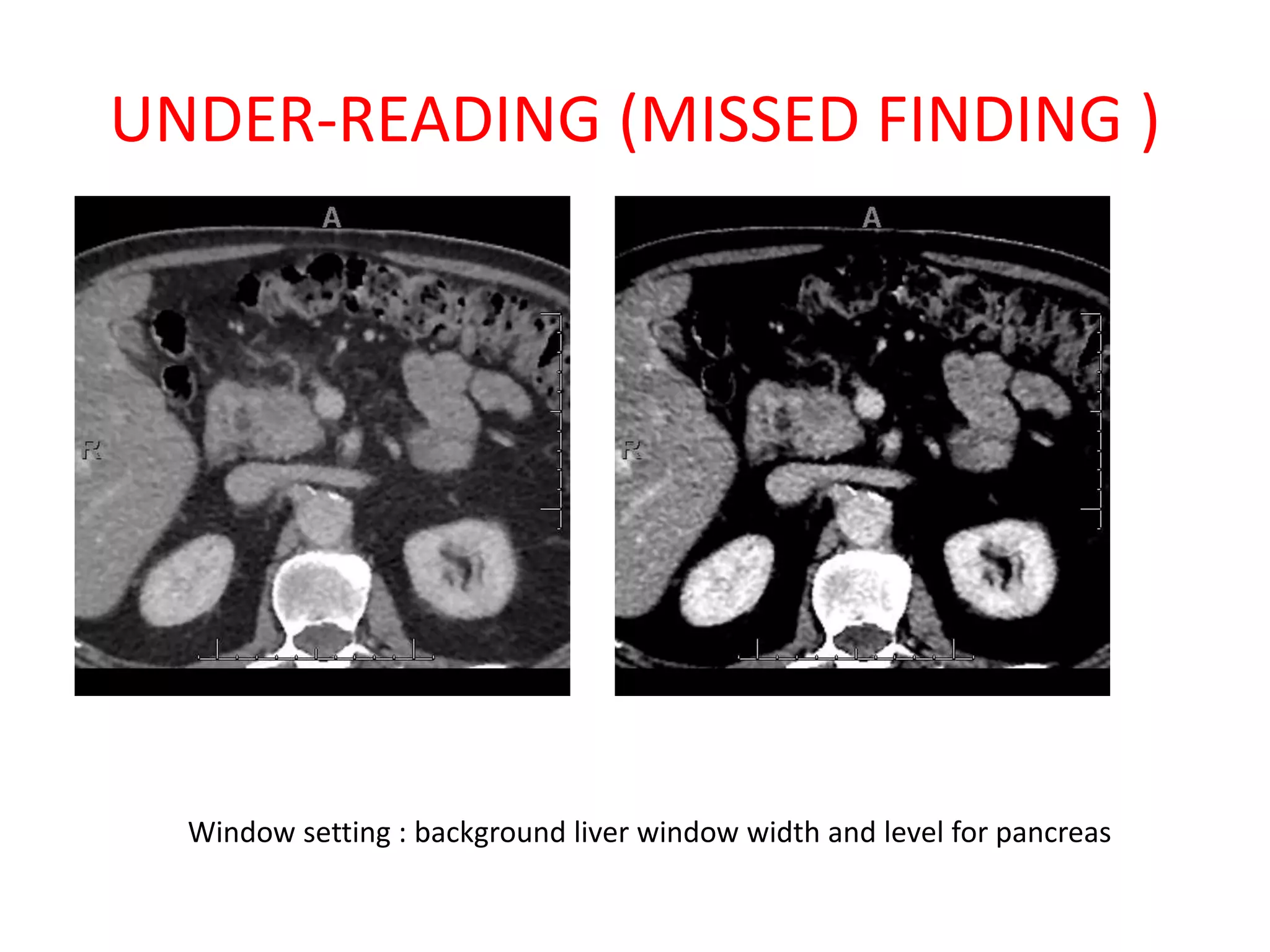
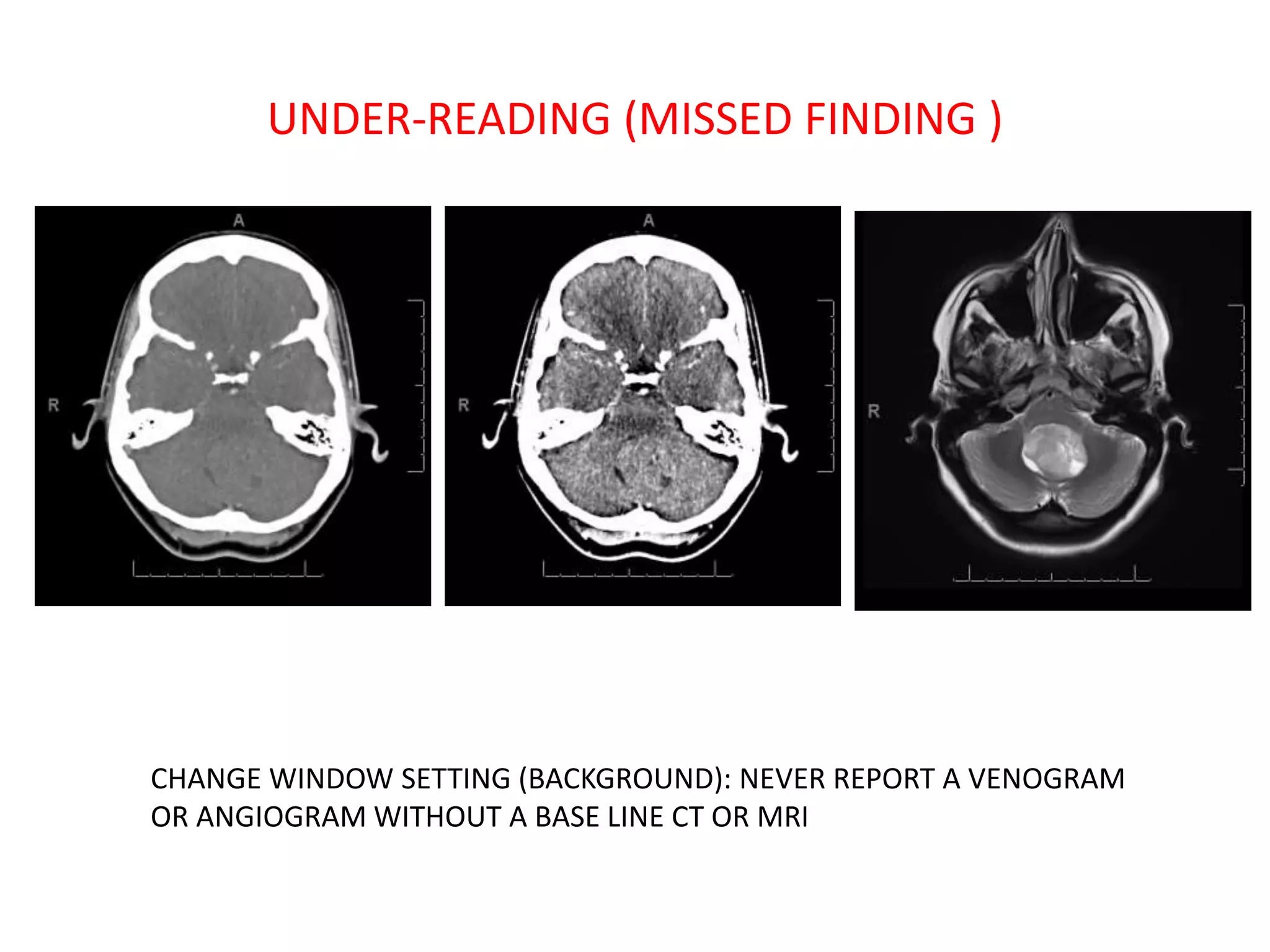
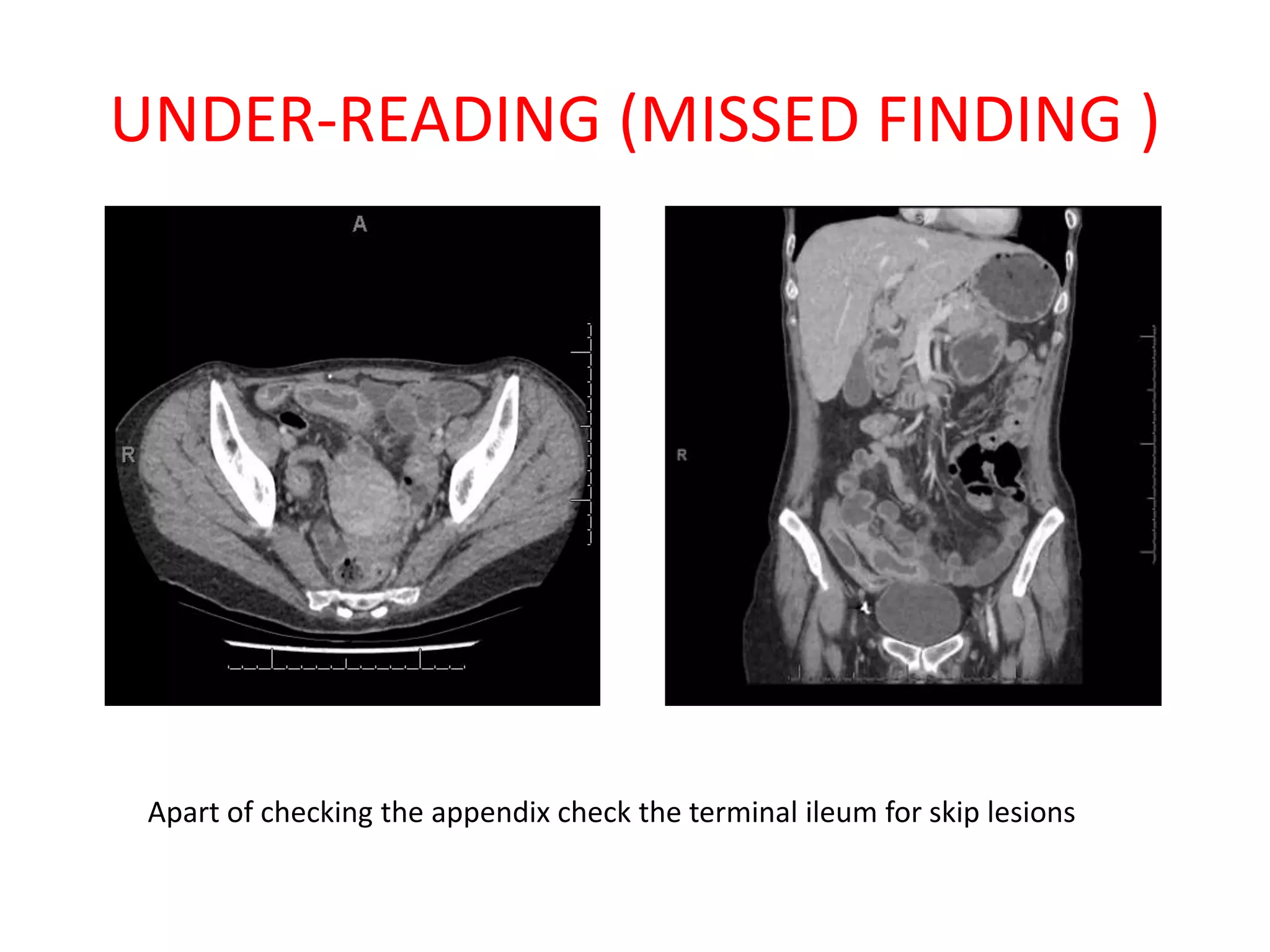
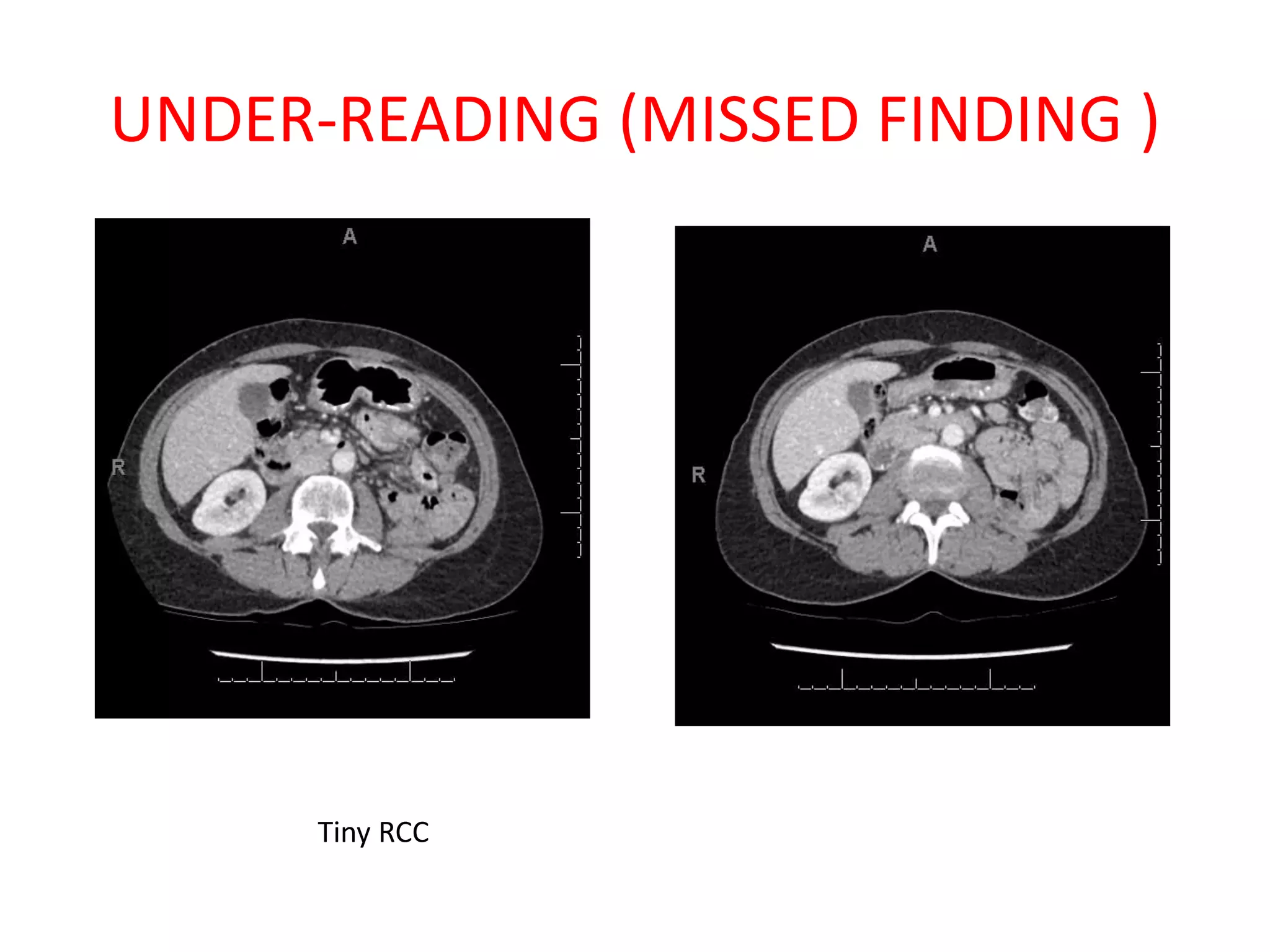
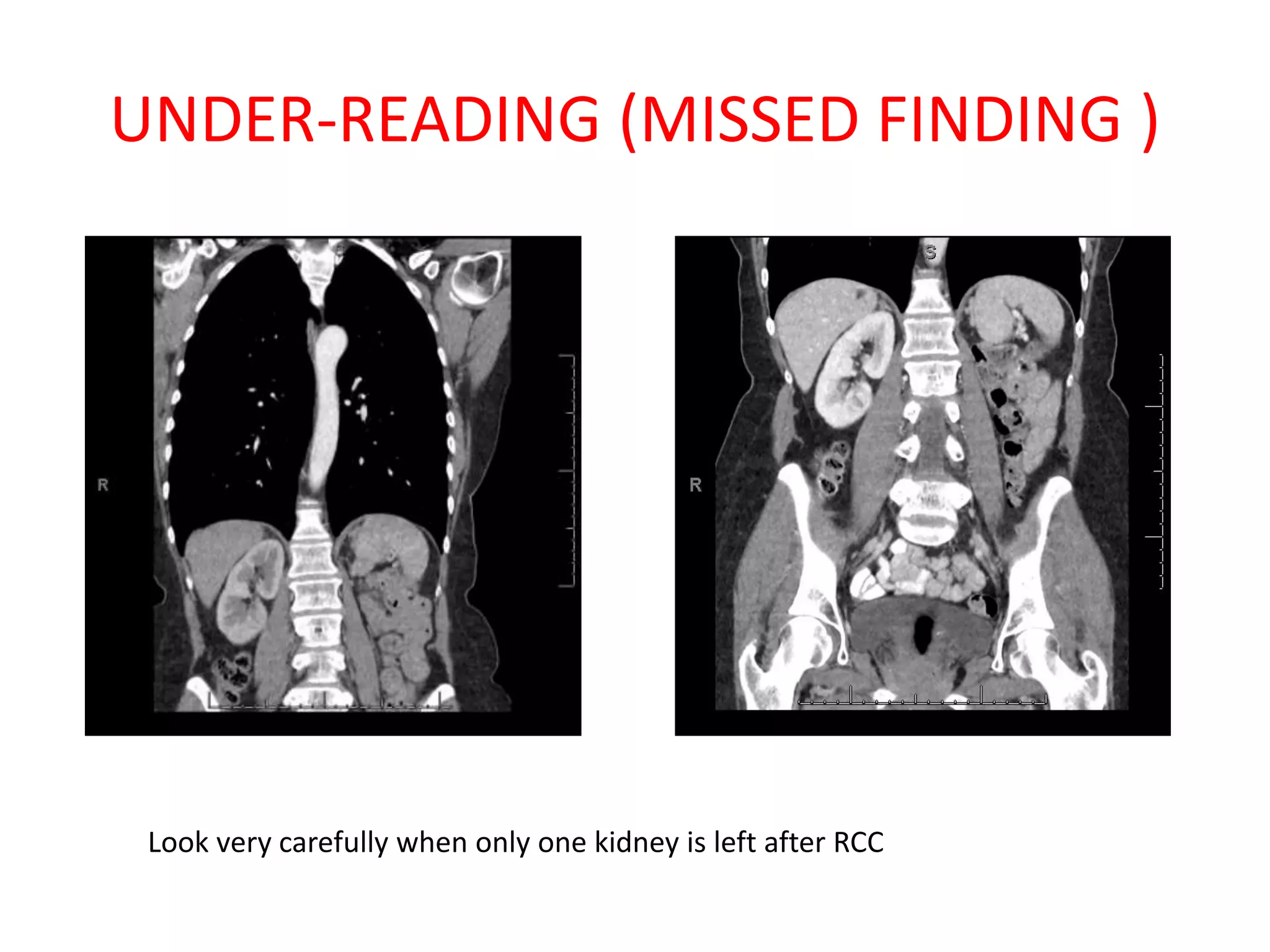
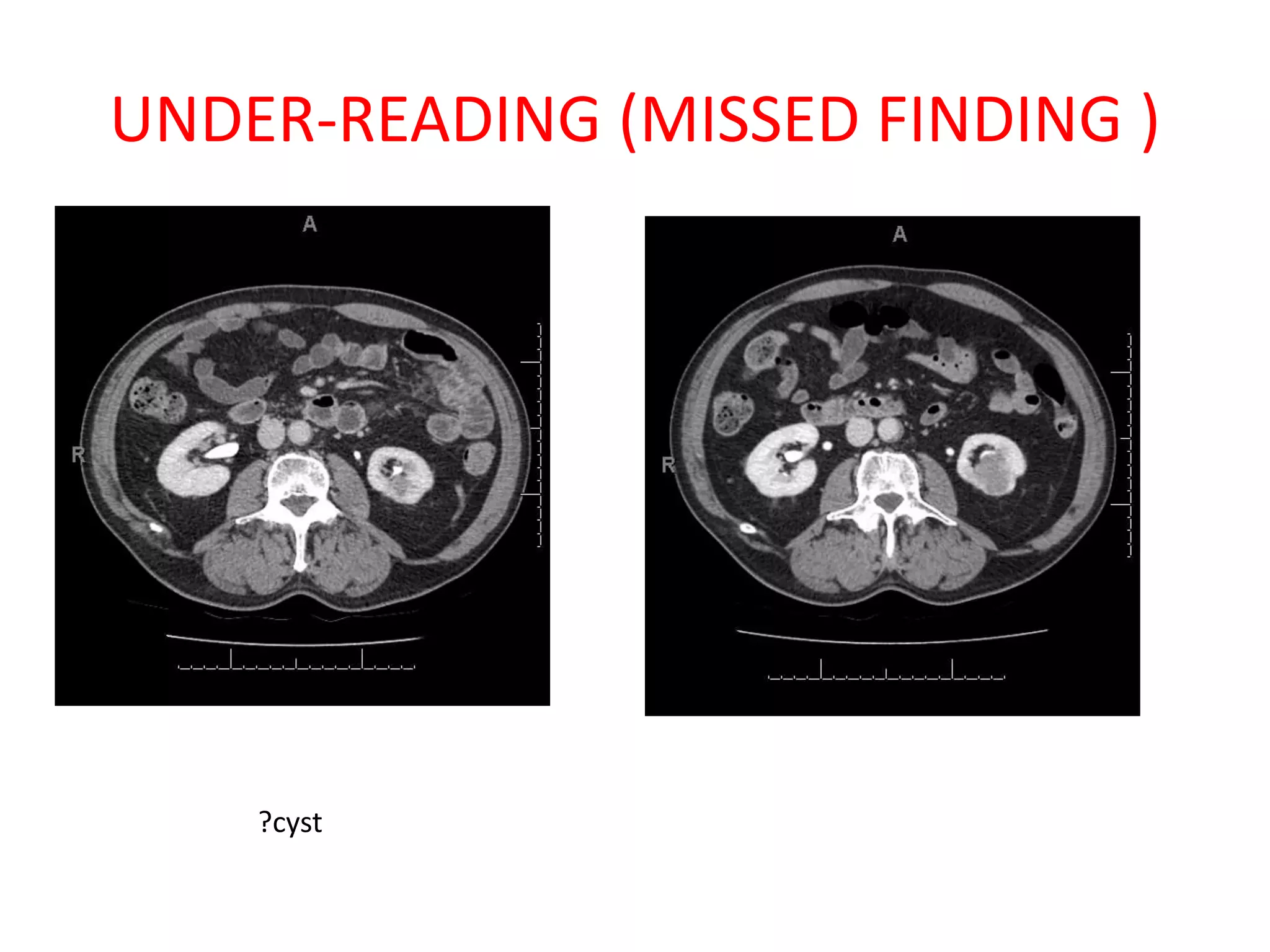
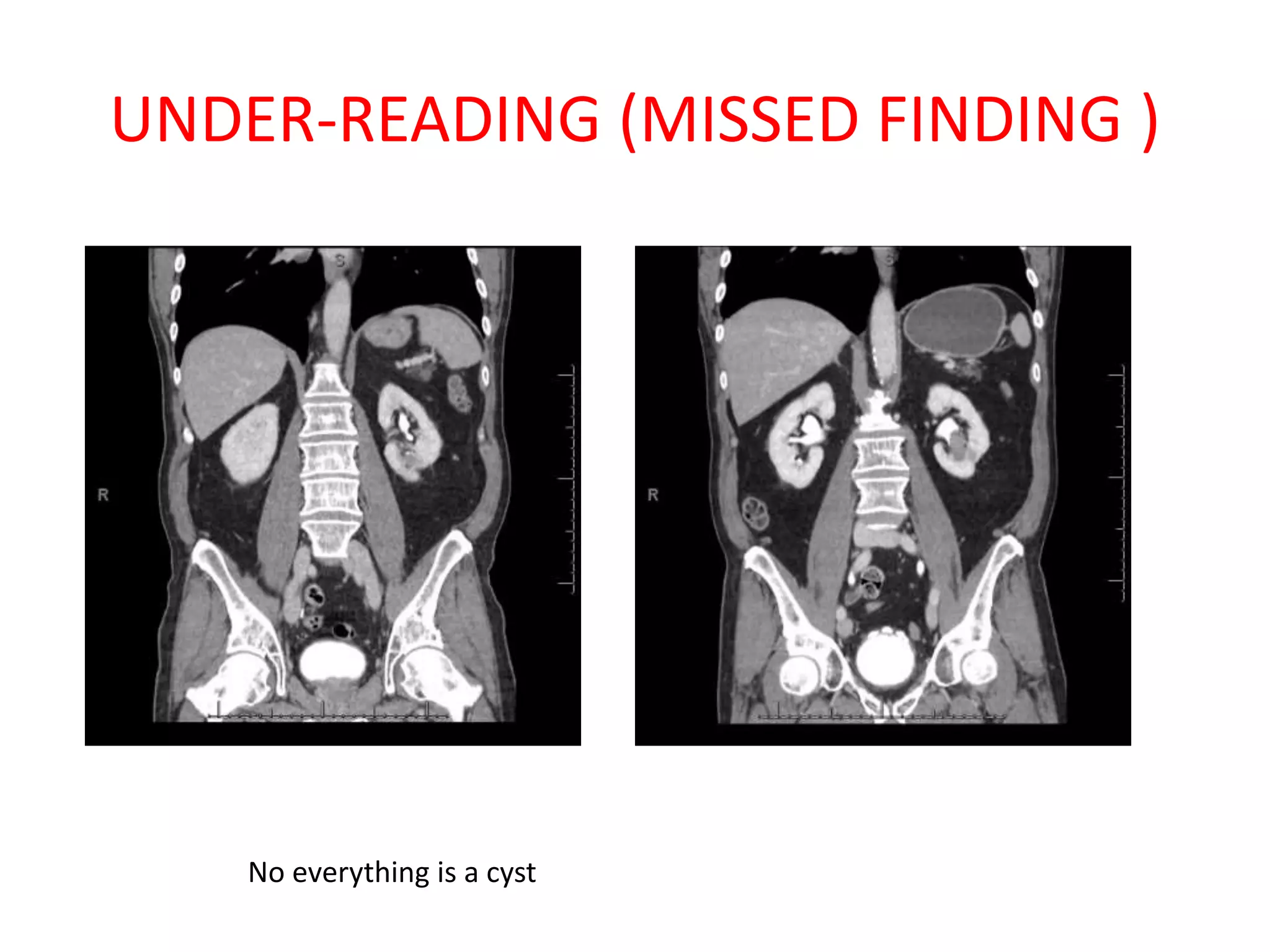
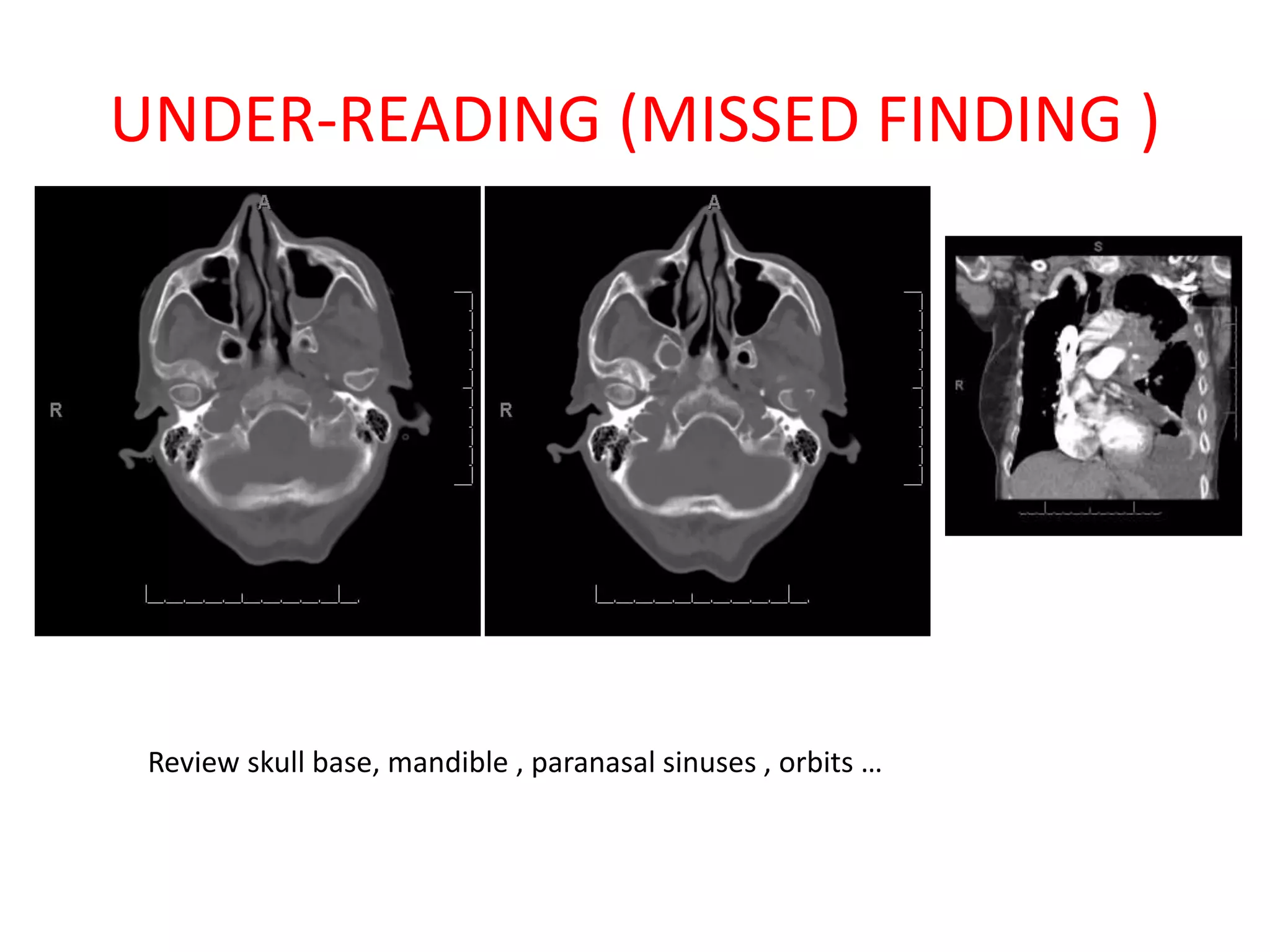
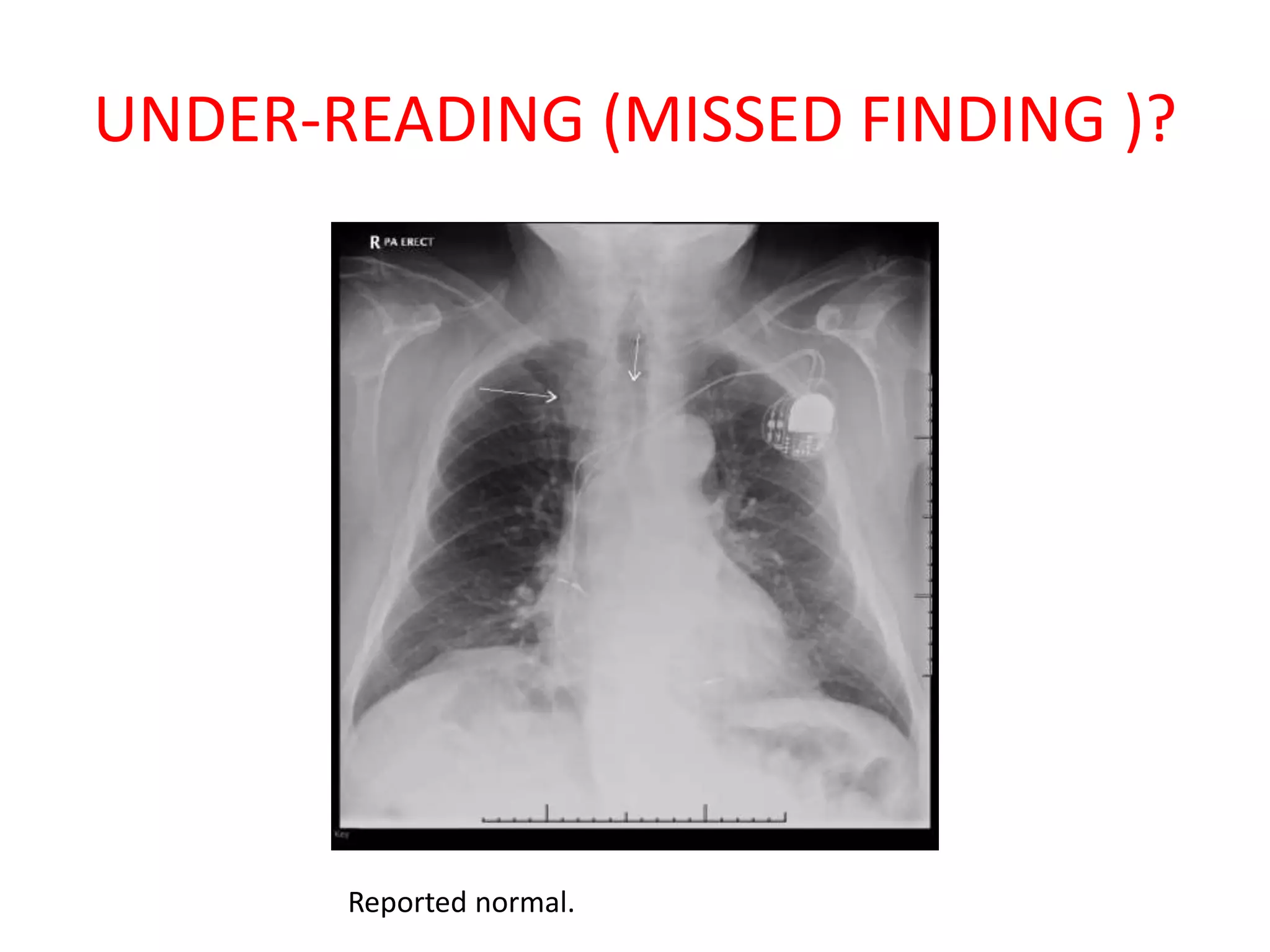
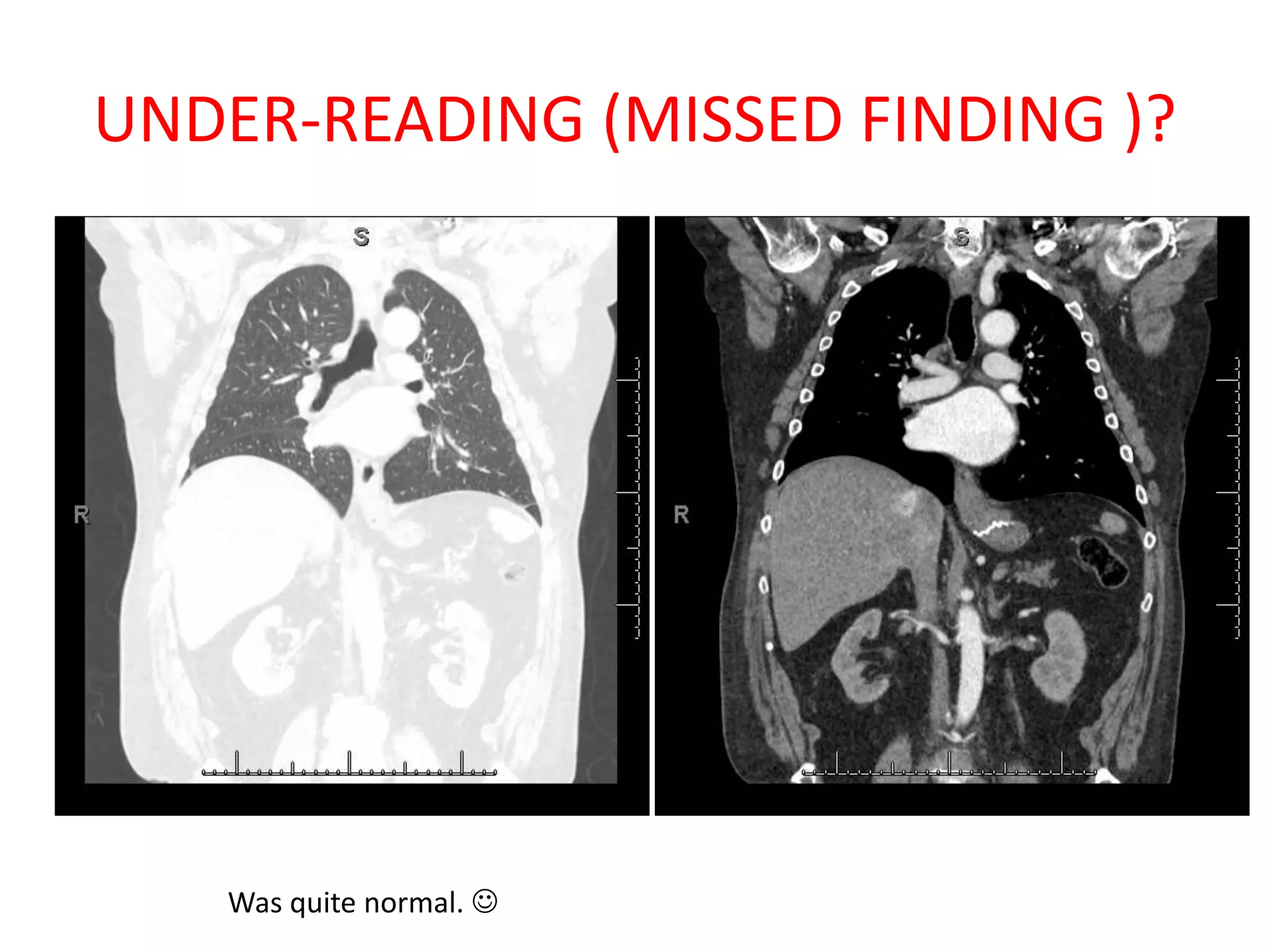
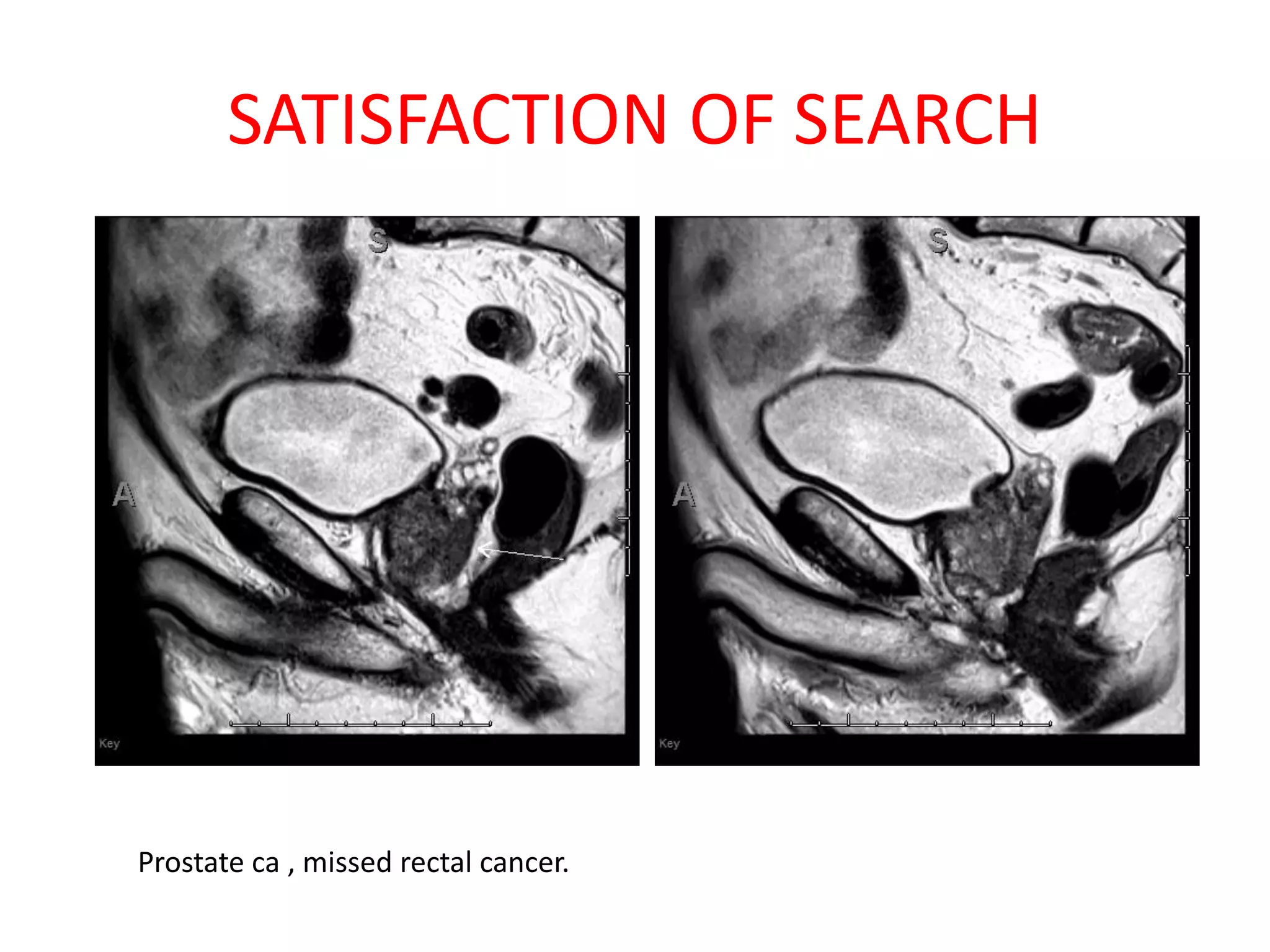
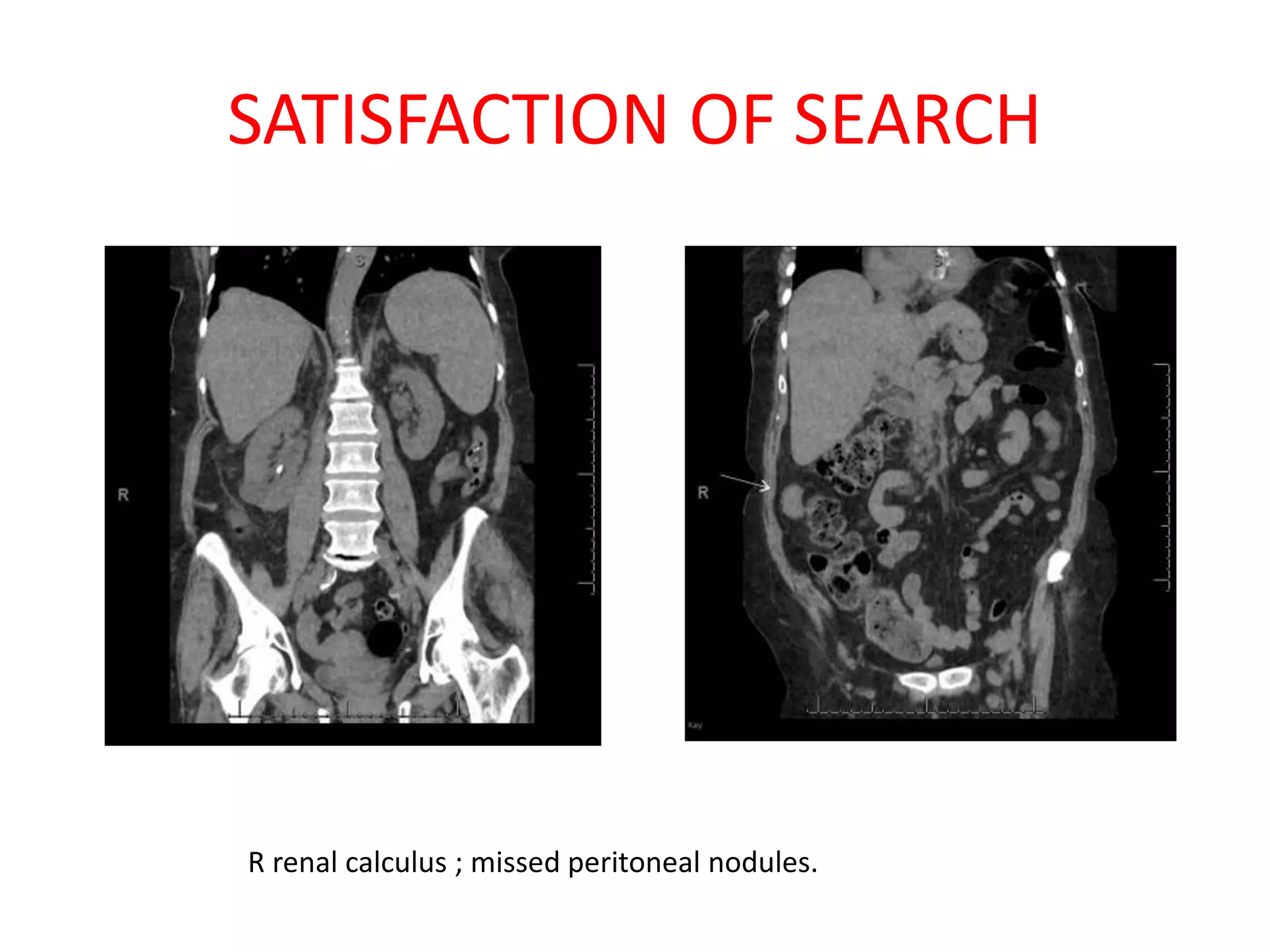
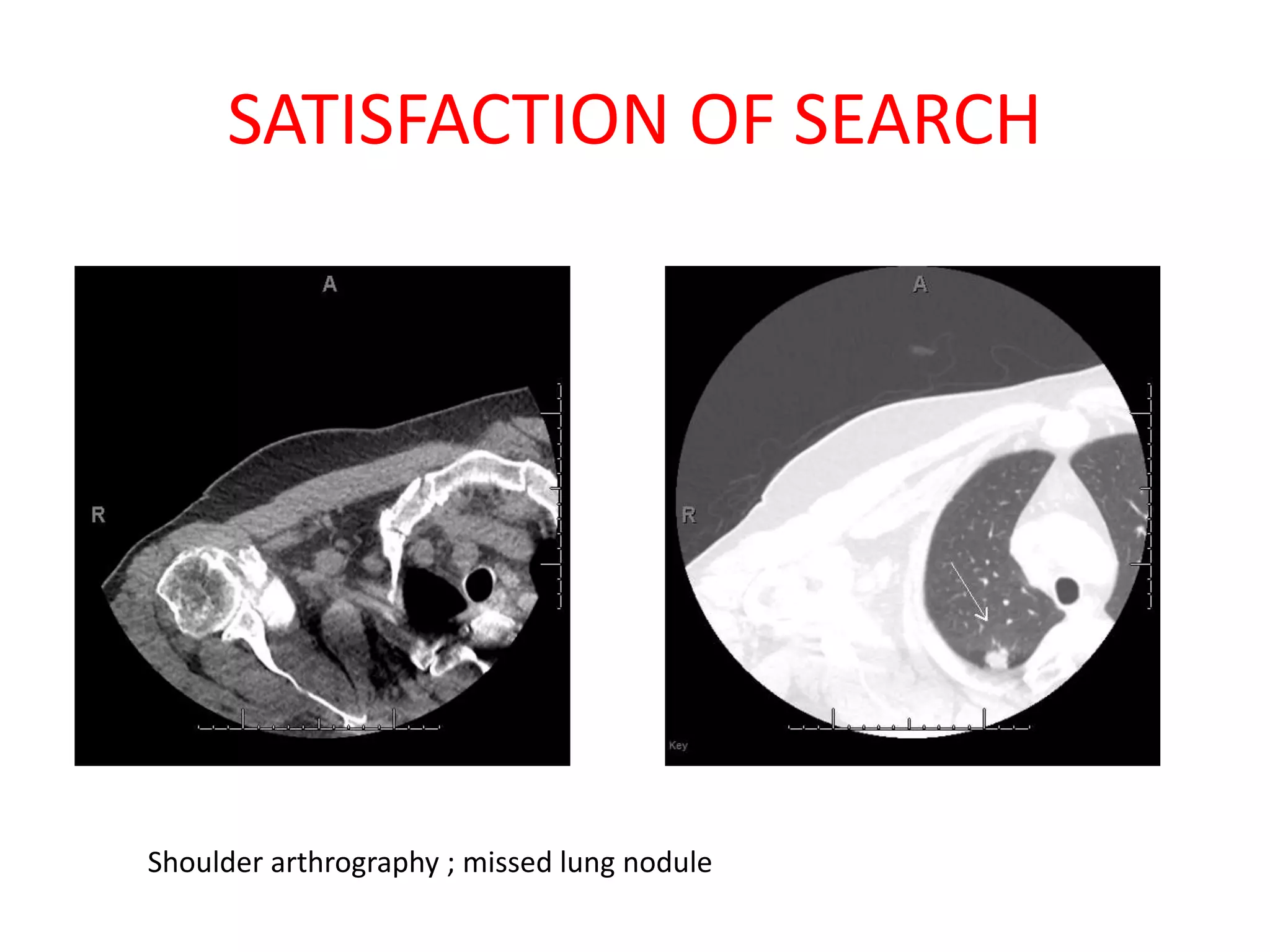
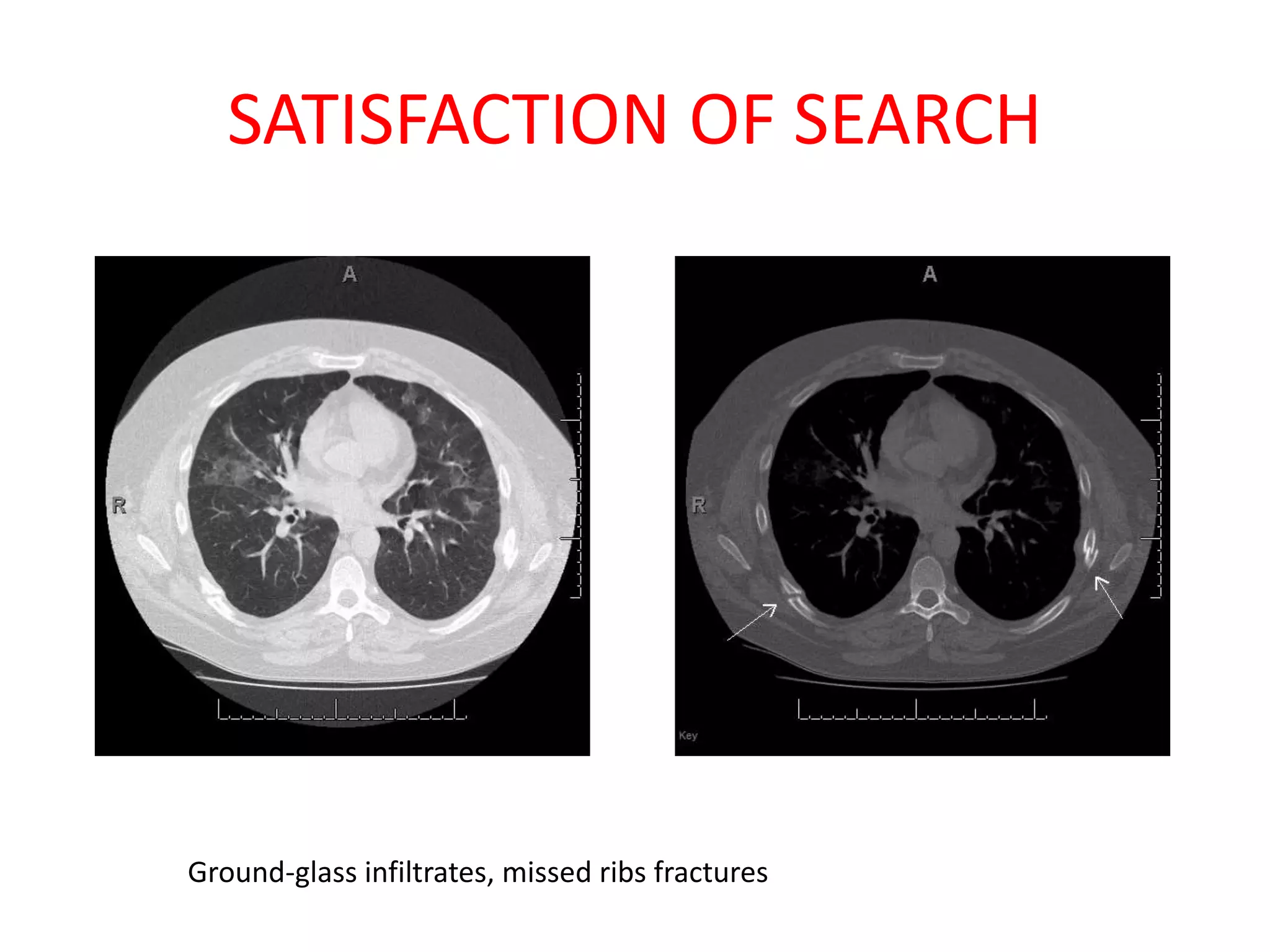
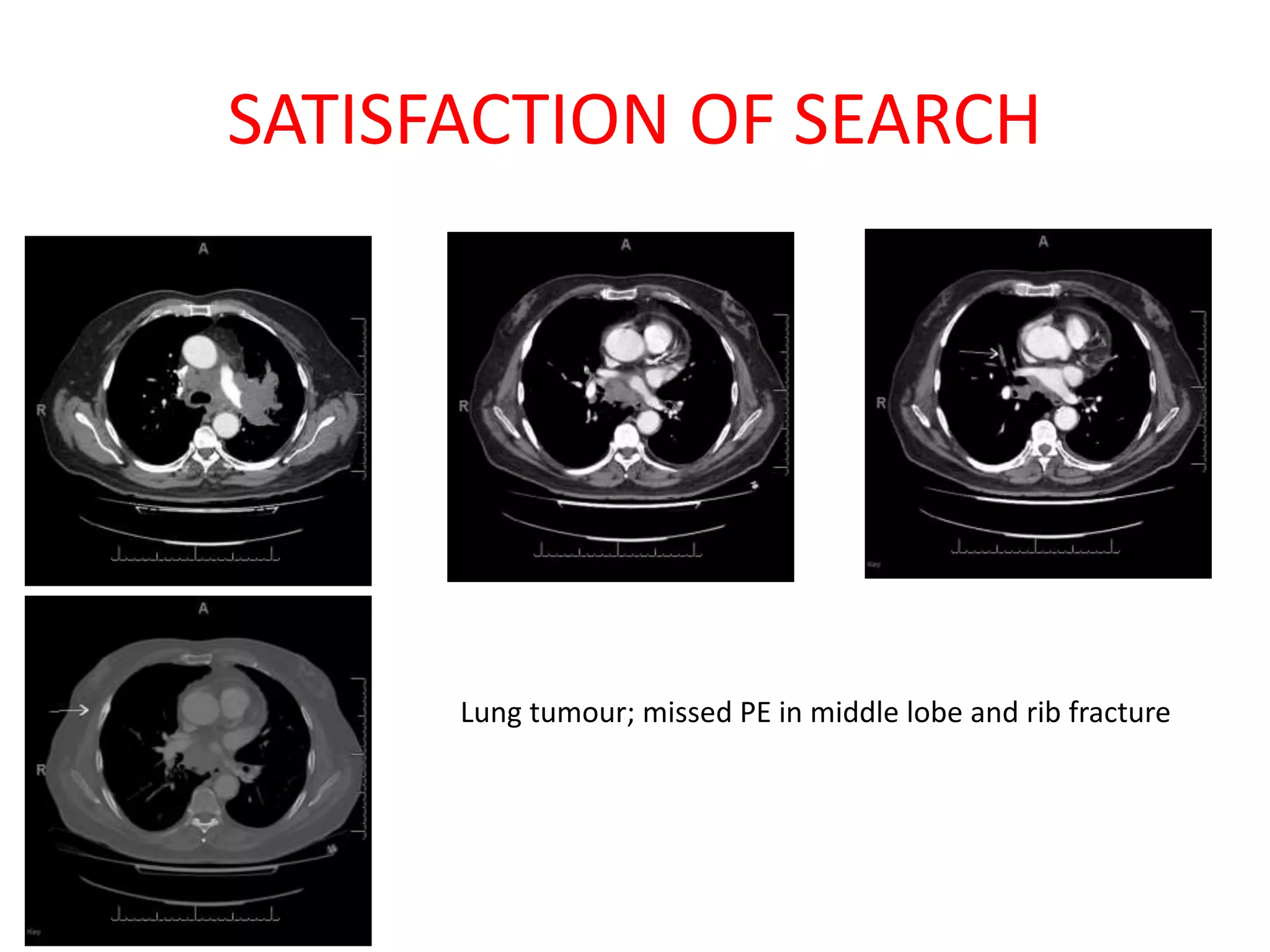
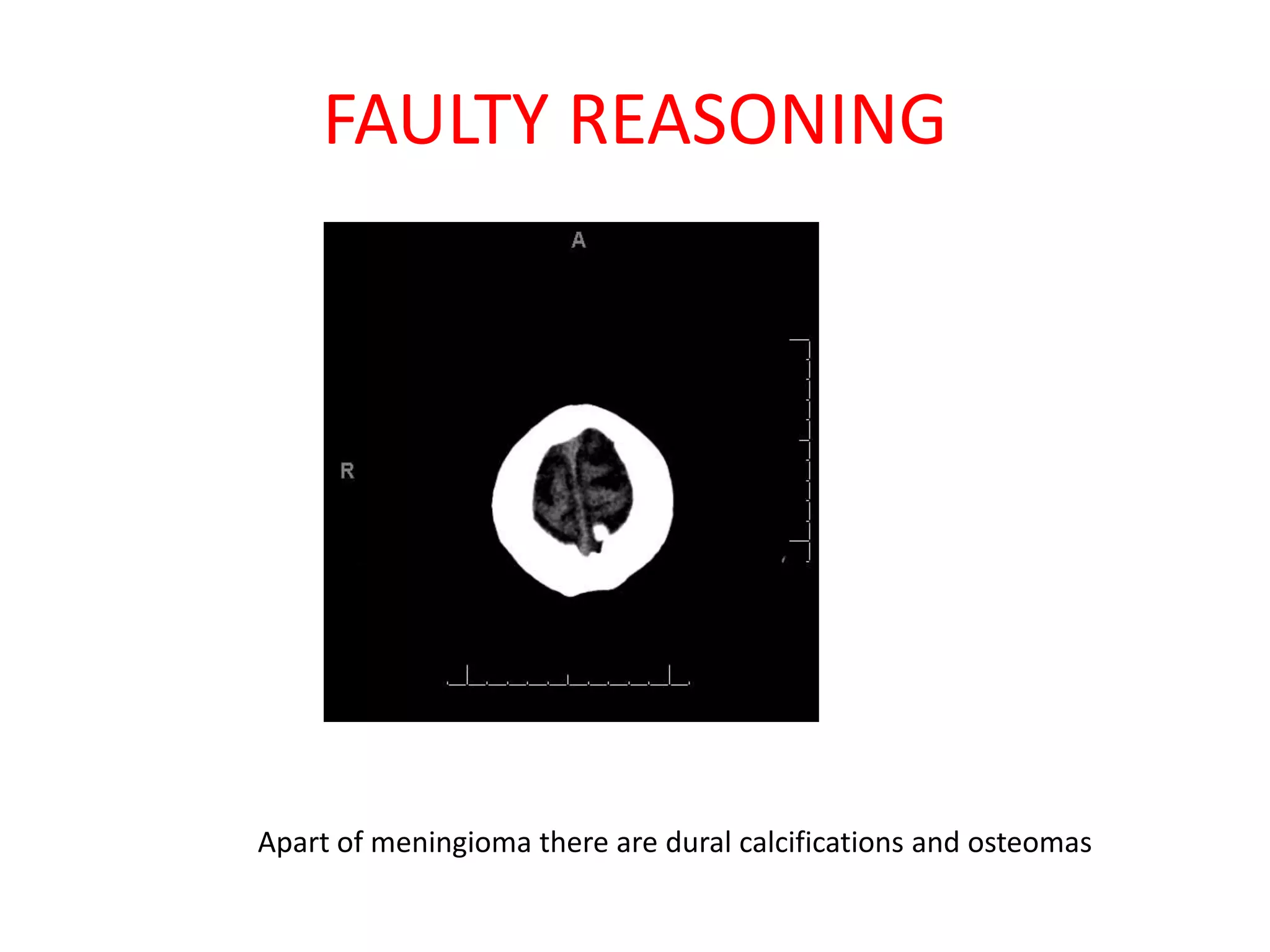
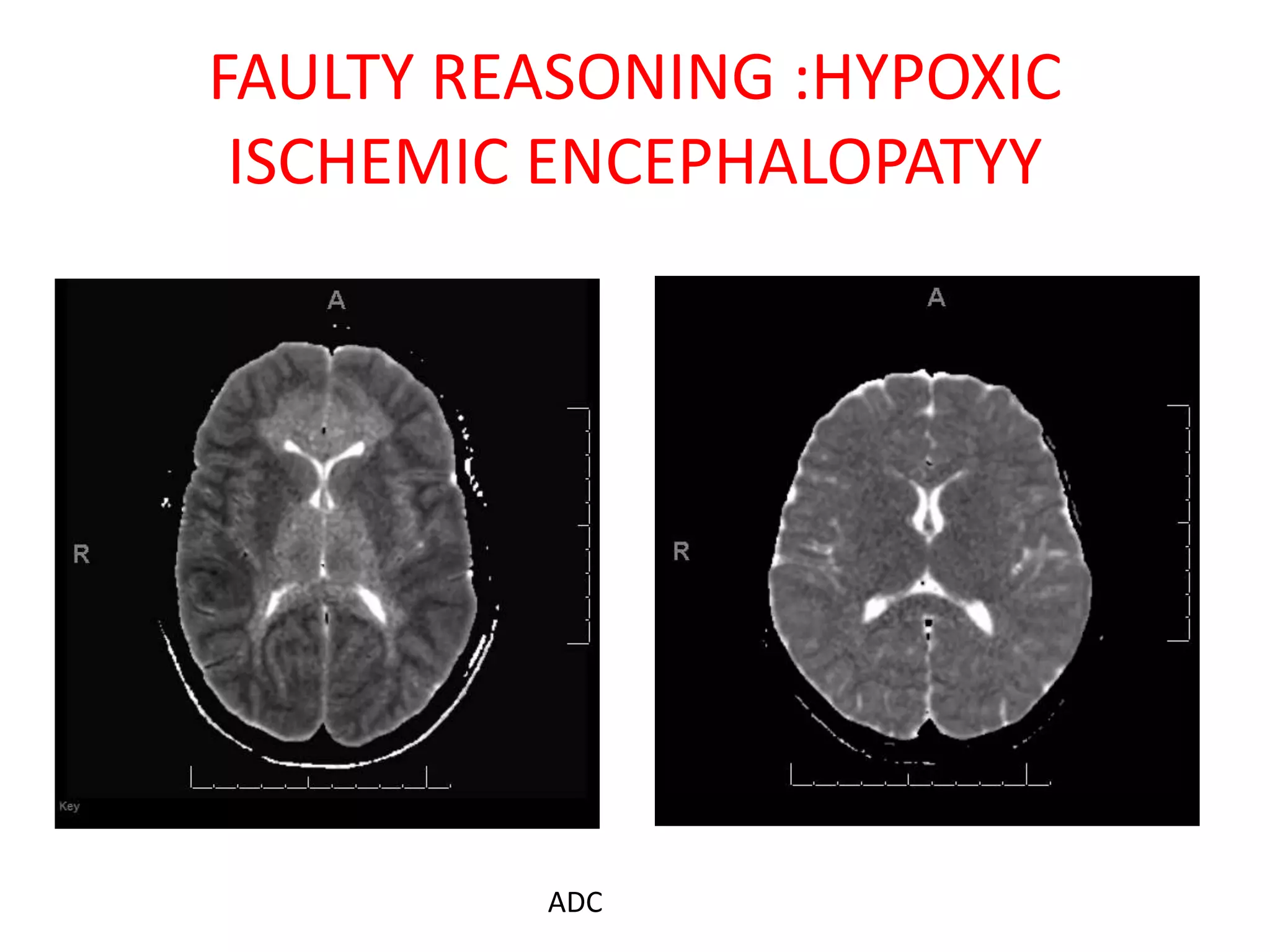
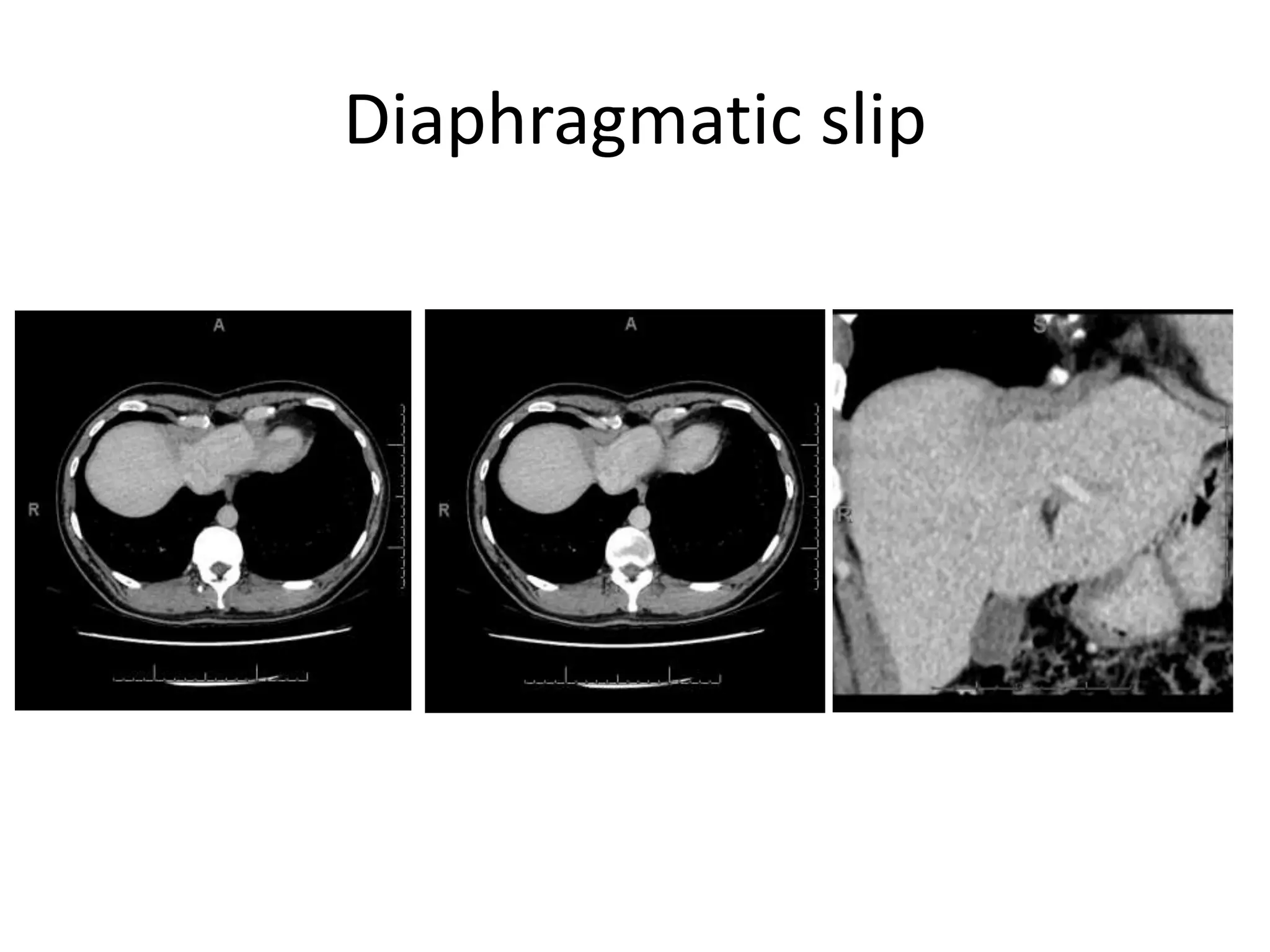
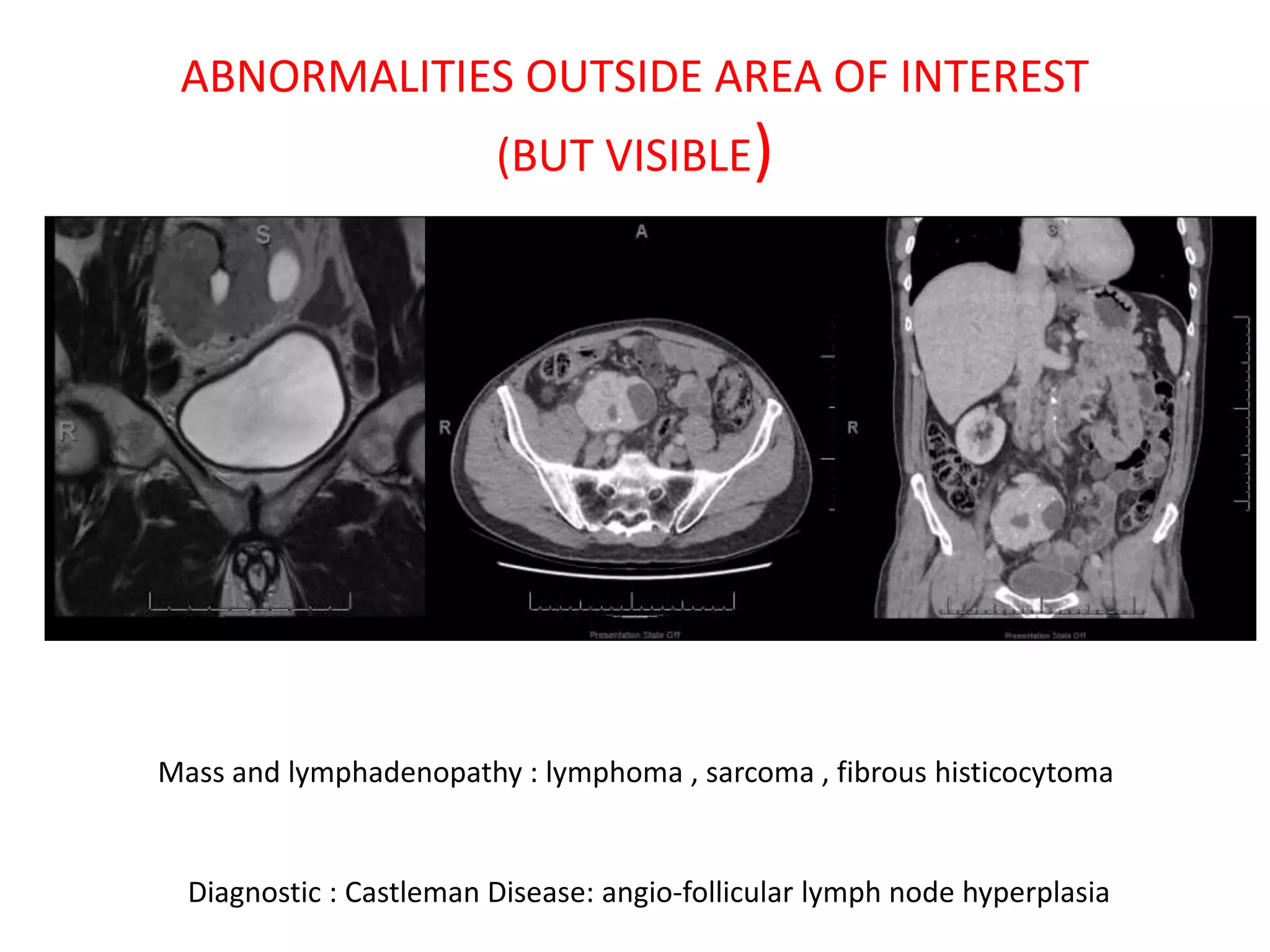
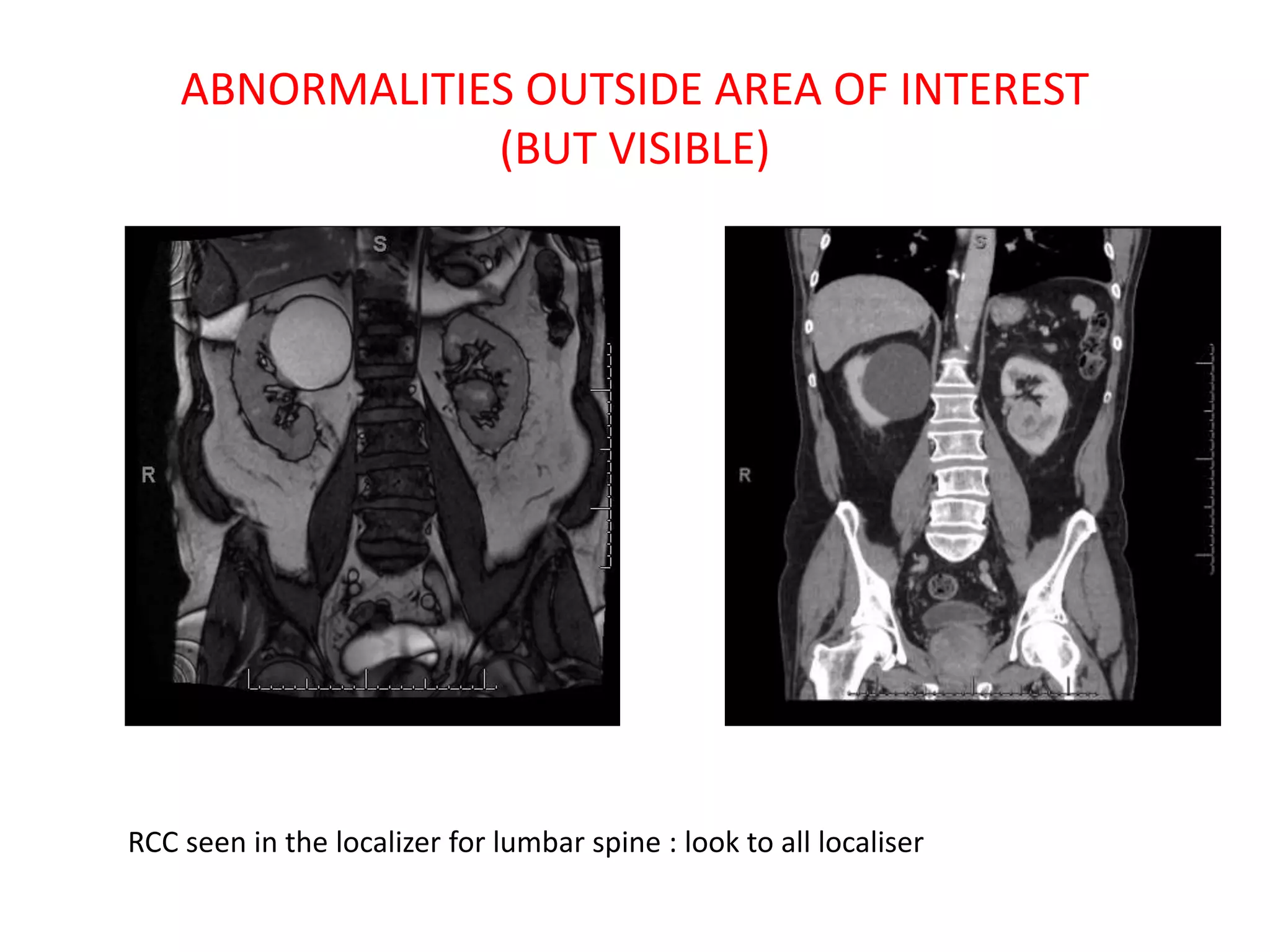
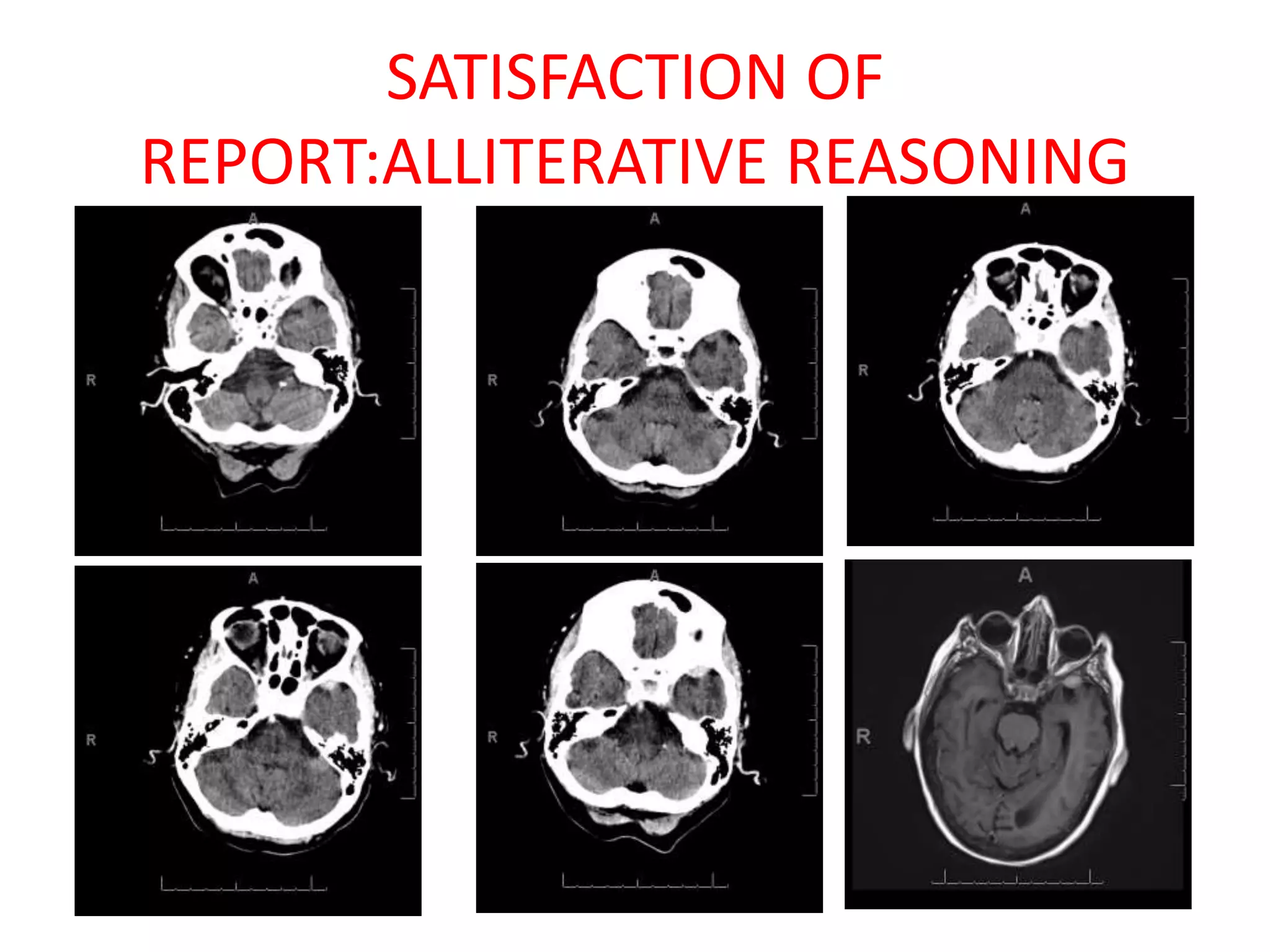
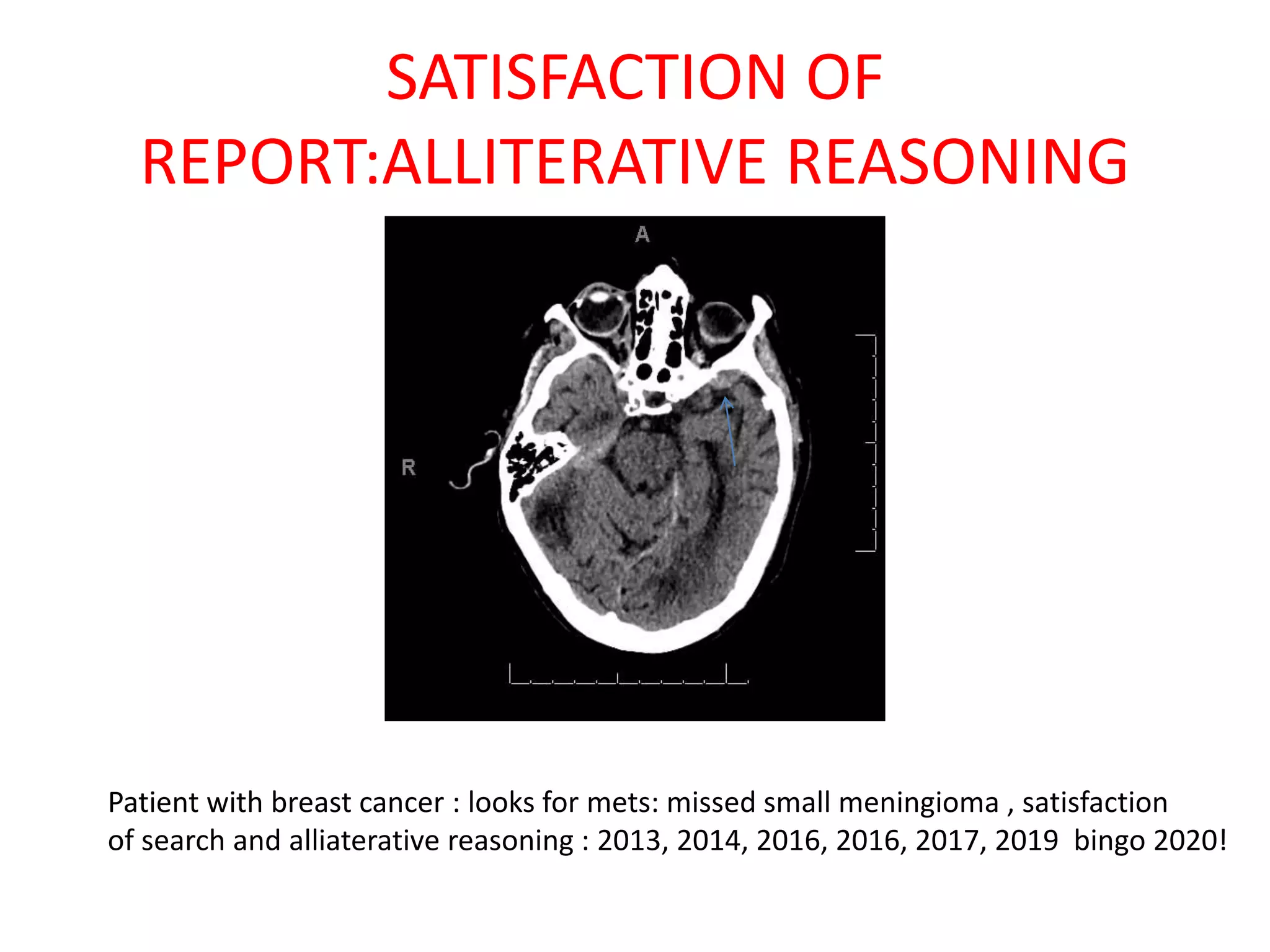
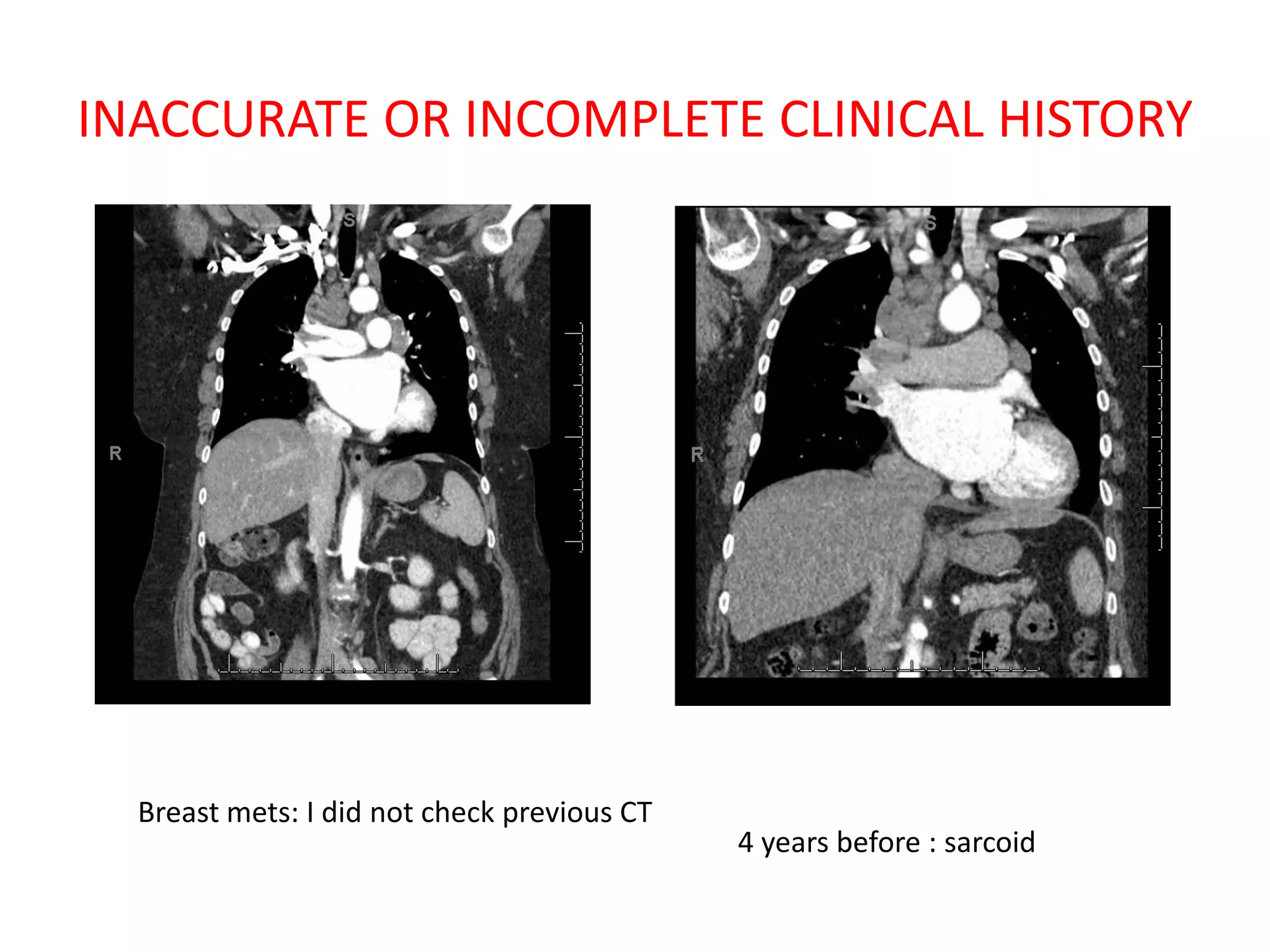
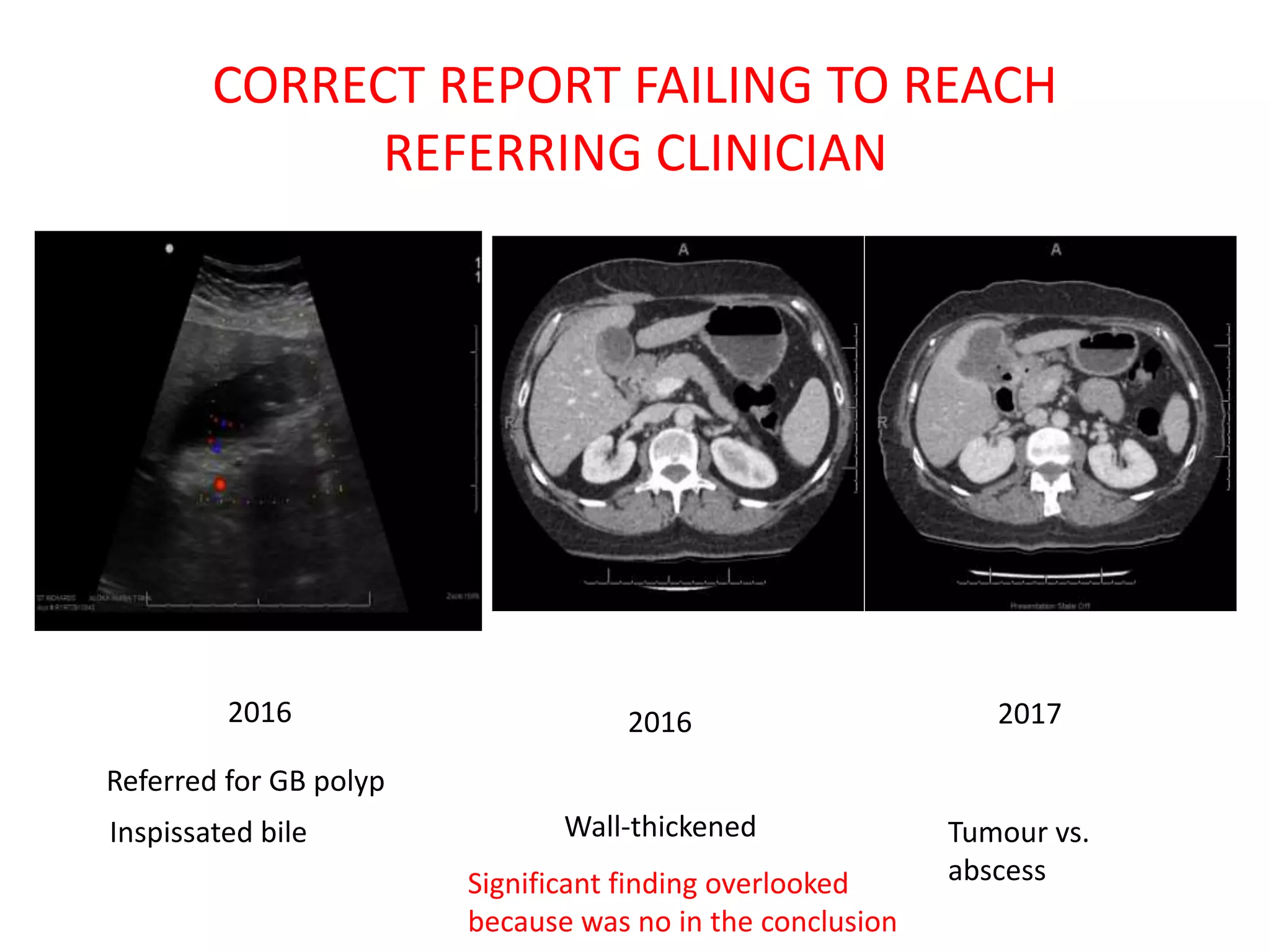
The document discusses various types of errors that can occur in diagnostic radiology, including perceptual errors, interpretative errors, and biases. It notes that perceptual errors, where an abnormality is simply missed on images, account for around 60-80% of errors. Common missed findings on chest X-rays include small pulmonary nodules. Cognitive and interpretative errors involve seeing an abnormality but misunderstanding its meaning, leading to an incorrect diagnosis. The most frequent types of errors identified in studies include under-reading/missed findings, satisfaction of search errors, and faulty reasoning errors. Human biases like anchoring bias can also influence diagnoses.