Dermatitis atópica
•Download as PPTX, PDF•
2 likes•434 views

This document discusses atopic dermatitis (eczema), including its pathophysiology, epidemiology, treatment recommendations, and evidence. Key points: 1. Atopic dermatitis is a chronic, relapsing inflammatory skin disease caused by genetic and immune mechanisms resulting in dry, itchy skin. 2. Treatment recommendations include topical corticosteroids and calcineurin inhibitors based on severity, with more potent topical/oral steroids, phototherapy, immunosuppressants for refractory cases. 3. Evidence suggests ultra-potent topical steroids should not be used continuously for more than 3 weeks to avoid side effects like skin atrophy.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Dermatitis atópica
Similar to Dermatitis atópica (20)
Recently uploaded
Recently uploaded (20)
Dermatitis atópica
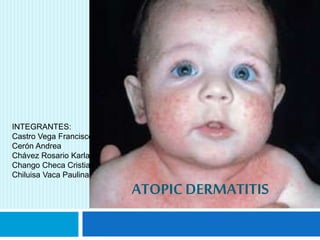
- 1. ATOPICDERMATITIS INTEGRANTES: Castro Vega Francisco Cerón Andrea Chávez Rosario Karla Chango Checa Cristian Chiluisa Vaca Paulina
- 2. Chronic, relapsing inflammatory skin disease immune mechanism
- 3. prurigo intense dry skin erythema exudate Characterized by lesions
- 4. • Folds of elbows-knees • Face • neck • Asthma • Rhinitis • Food allergic. Flexural surfaces affects Clinical phenotype
- 5. EPIDEMIOLOGY
- 6. EPIDEMIOLOGY
- 7. Families of patients with atopic dermatitis are also affected by the disease 3.4% a normal quality of life 23.3% slightly affected 66.4% moderately impaired 6.9% strong impact on their quality of life.
- 10. Genetic predisposition Genes encoding elements of the immune system • 5q 31-33 • Th2: IL4, IL5, IL13, GM-CSF Genes encoding structural proteins of the skin • 1q 21-23 FLG (filaggrin) • epidermal differentiation genes
- 11. Skin barrier dysfunction LOSS OF THE UNION CORNEODESMOSOME
- 12. LOSS OF LIPID •LOSS OF WATER ELASTICITY AND FLEXIBILITY. •PENETRATION O SOLUBLE SUBSTANCES.
- 13. DRY SKIN PRESENTS CRACKS THAT PERMIT THE ENTRANCE OF MICROORGANISMS PRODUCE INFLAMMATION
- 14. Immunological Alterations Imbalance in the production of lymphocytes. Increased production of Th2 lymphocytes INFLAMMATION PRURITUS ERYTHEMA
- 17. Education and training of patients and their families: Recommendations concerning bathing, hydration with emollients, stress reduction, psychological support, and avoidance of triggers (irritants, detergents, solvents, aeroallergens, and certain foods). The chronic nature of the disease and possible complications should be explained and patients and their families should be given any other information considered helpful.
- 18. Induction therapy Topical corticosteroids and calcineurin inhibitors (pimecrolimus, tacrolimus). Maintenance therapy Used in cases of persistent disease or very severe or frequent relapses. Intermittent (weekend) regimen of topical corticosteroids and maintenance therapy with calcineurin inhibitors (twice weekly)
- 19. Treatment of refractory cases Very potent topical corticosteroids, oral corticosteroids, oral ciclosporin, and phototherapy. In each case, assess the patient’s age and the stage and type of the predominant lesions (acute, subacute, chronic lichenified), the site of lesions, the extent of disease, and response to prior treatment. Oral antihistamines to control pruritus Treatment of complications (bacterial and viral infections) with topical and/or systemic antibiotics or antivirals if necessary.
- 20. MILD ATOPIC DERMATITIS: 1. Basic recommendations and information: bathing, hydration, avoid triggers, reduce stress, chronic nature of condition and possible complications, food, psychological support, consideration of prebiotic and/or probiotic treatment, etc. 2. Topical corticosteroids (1/24 h) until remission 3. Topical pimecrolimus or tacrolimus (1/12-24 hours) until remission.
- 21. MODERATE ATOPIC DERMATITIS: 1. Maintenance regimen of topical corticosteroids (twice weekly, weekend regimen) 2. Maintenance regimen of topical pimecrolimus or tacrolimus (twice weekly) 3. Oral corticosteroids: PREDNISONE (1 mg/kg/24 h) until flare is controlled, then gradually tapered (1-3 wk) 4. Emollient–corticosteroid wet-wrap dressings 1/24 h for 1 week 5. CICLOSPORIN (3-5-7 mg/kg/24 h) until flare is controlled (6-12 wk), then gradually tapered. 6. PHOTOTHERAPY: Medium doses of narrowband UV-B, UV-B or UV-A.
- 22. SEVERE ATOPIC DERMATITIS: 1. CICLOSPORIN (2.5 mg/kg/24 h) for at least 6 months 2. AZATHIOPRINE, maintenance regimen (100-200 mg/24 h) 3. METHOTREXATE, maintenance regimen (10-20 mg/wk) 4. MYCOPHENOLATE MOFETIL, maintenance regimen (1-2 g/24 h) 5. Psoralen UV-A 6. Intravenous immunoglobulins. (1-2 g/kg/mo) for 3-6 mo 7. Interferon- 50 g/m2/24 h for 12 wk 8. Hydroxychloroquine (200 mg/24 h) 9. Omalizumab 10. Rituximab 11. Alefacept 12. TNF- inhibitors
- 23. TO CONTROL PRURITUS 1. Sedative antihistamines 2. Antileukotrienes 3. Naltrexone 4. Serotonin modifiers 5. Ondansetron 6. Doxepin TO CONTROL INFECTION 1. Topical or systemic antibiotics (against Staphylococcus aureus) when signs of superinfection are present until infection resolves 2. Topical or systemic antivirals
- 24. EVIDENCE
- 25. Evidence of double infraorbital foldz
- 26. The objectives are as : To assess the best application strategies of topical corticosteroids for treating established eczema in people of all ages
- 27. The term ’atopic eczema’ should only refer to individuals who have the physical features of eczema plus evidence o specific immunoglobulin E (IgE) antibodies to common environ-mental allergens.
- 28. Types of studies All randomised controlled trials (RCTs) comparing different strategies for administering topical corticosteroids for treating eczema
- 29. When prescribing topical steroids is important to consider the diagnostic and the steroid potency route of administration frequency of administration duration of treatment side effects
- 30. Recommendations for clinical practice CLINICAL RECOMMENDATION Level of Evidence Ultra highly potent topical steroids should not be used continuously for more than three weeks C Corticosteroids low power to high power should not be used continuously for more than three months to avoid side effects. C Combinations of topical steroids and antifungal agents should generally avoided to reduce the risk of infections C
- 31. Power of Topical Corticosteroids Power GENERIC Ultra high ( I) Betamethasone dipropionate 0.05% Clobetasol propionate 0.05 % high (II) Amcinonide 0,1% Desoximetasona Medium-High ( III ) Propionato fluticasona 0,005% Acetónido triamcinolona 0,5%
- 32. Power GENERIC Medium ( IV and V ) Valerato betametasona Valerato hidrocortisona 0,2% Low ( VI) Alclometasona dipropionato 0,05% Desonida 0,05% Less potent (VII ) Fluocinolona 0,01% Butirato hidrocortisona 0,1% Hidrocortisona 1%, 2,5%
- 33. Frequency of administration Application once or twice a day is recommended for Most preparations. The administration's often does not provide better results. Chronic application of topical steroids can induce tolerance and tachyphylaxis
- 34. Side Effects The most common side effect of using topical corticosteroids is skin atrophy . more powerful steroids , occlusion , the skin more thin, and the older the patient increases the risk .