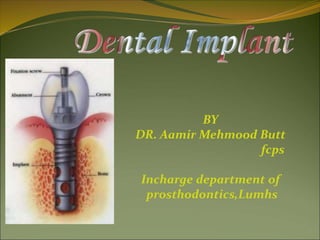
2. WHAT IS A DENTAL IMPLANT?
Dental implant is an artificial titanium fixture
(similar to those used in orthopedics)
which is placed surgically into the jaw bone to
substitute for a missing tooth and its root(s).
OR
A permucosal device which is biocompatible
and biofunctional and is placed within mucosa
or, on or within the bone associated with the
oral cavity to provide support for fixed or
removable prosthetics.
5. Endodontic Implant (Stabilizer)
Endodontic stabilizer implants are
endosteal implants.
threaded post that passes at least 5
mm beyond the apex of the tooth
root into available bone.
providing additional abutment
support for restorative dentistry.
Five millimeters of available apical
bone is the minimum that can
increase the crown-root ratio to an
extent sufficient to affect positively
the prognosis of the tooth.
6. Sub-periosteal implant
introduced in the 1940.
longest period of clinical
application.
shaped to ride on the
residual bony ridge of
either the upper or lower.
have been used in
completely edentulous as
well as partially
edentulous upper and
lower jaws. However, the
best results have been
achieved in treatment of
the edentulous lower jaw.
7. Sub-periosteal implant…
Indications
Usually a severely
resorbed, completely
edentulous, lower jaw
bone which does not
offer enough bone
height to
accommodate Root
form Implants as
anchoring devices.
9. Plate-form implant
Their name is derived from their flat,
blade-like (or plate-like) portion,
which is the part that gets embedded
into the bone.
Used where the residual bone ridge
of the jaw is either too thin (due to
resorption) & Difficult to place
conventional Root form Implants or
certain vital anatomical structures
prevent conventional implants from
being placed.
Bone grafting procedure, which re-
establishes the lost bone have
reduced the use of this form
10. Ramus-frame implant
Ramus-frame Implants belong in the category of
endosseous implants, although their appearance
might not suggest that at first.
These implants are designed for the edentulous lower
jaw only and are surgically inserted into the jaw bone
in three different areas: the left and right back area of
the jaw (the approximate area of the wisdom teeth),
and the chin area in the front of the mouth.
The part of the implant that is visible in the mouth
after the implant is placed looks similar to that of the
Subperiosteal Implant.
12. Dr,salah hegazy
Indications:
Usually a severely resorbed, edentulous lower
jaw bone, which does not offer enough bone
height to accommodate Root form Implants as
anchoring devices. These implants are usually
indicated when the jaws are even resorbed to the
point where Subperiosteal Implants will not
suffice anymore.
Ramus-frame implant
13. Dr Aamir Butt
An additional advantage that comes with this
type of implant is a tripodial stabilization of the
lower jaw. A jaw as thin as the one shown above
can easily fracture at its thinnest part. The
Ramus-frame Implant, once integrated (after a
three month waiting period) will also stabilize
and protect the jaw somewhat from fracturing.
14. Dr Aamir Butt
The Ramus-frame Implant usually comes in a standard pre-shaped form and
needs to be custom-fitted to the patient's individual jaw dimension, as shown
below:
16. C.Root form implant
Since the introduction of the Osseointegration
concept and the Titanium Screw by Dr.
Branemark, these implants have become the
most popular implants in the world today.
17. Root form Implants come in a variety of
shapes, sizes, and materials and are being
offered by many different companies
worldwide. Some clinicians regard them to be
the Standard of Care in Oral Implantology.
These implants can be placed wherever a
tooth or several teeth are missing, when
enough bone is available to accommodate
them. However, even if the bone volume is not
sufficient to place Root form Implants, Bone
grafting procedures within reasonable limits
should be initiated, in order to benefit from
these implants.
18. Root form implant shape:
Other variations dwell on the shape of the Root
form implant. Some are screw-shaped, others are
cylindrical, or even cone-shaped or any
combination thereof.
19. Today, the most accepted material for dental implants
is high grade Titanium—either CP Titanium or an
alloy thereof. The titanium alloy implants tend to be
stronger than the CP titanium implants. The bone
integration shows no difference to the two different
types of titanium.
Some implants have an outer coating of
Hydroxyapatite (HA). Other implants have their
surface altered through plasma spraying, or beading
process. This was developed to increase the surface
area of the titanium implant and, thus, in theory, give
them more stability. These surface treatments were
also offered as an alternative to the HA coatings,
which on some implants have shown to break loose or
even dissolve after a few years.
20. 6. Transosseous implant
These implants are not in use that much
any more, because they necessitate an
extraoral surgical approach to their
placement, which again translates into
general anesthesia, hospitalization and higher
cost, but not necessarily higher benefits to the
patient.
In any case, these implants are used in
mandibles only and are secured at the lower
border of the chin via bone plates. These were
originally designed to have a secure implant
system, even for very resorbed lower jaws.
21. A typical Transosseous Implant. The plate on the
bottom is firmly pressed against the bottom part of
the chin bone, whereas the long screw posts go
through the chin bone, all the way to the top of the jaw
ridge inside the mouth. The two attachments that will
eventually protrude through the gums can be used to
attach an overdenture-type prosthesis.
The plate
long screw posts
The two attachments
25. Early Implants
1937Adams’s submergible threaded cylindrical
implant with round bottom
1938 Strock’s (long term) threaded vitallium
implant
(cobalt+chrome+molybdenum)
The modern implants appear to be variants or
composites of some of the designs of early
implants
26. Subperiosteal Implants
Placing implants on and around bone rather than in it
1943 Dahl of Sweden placed with 4 projecting posts
Direct bone impression
Cobalt-chrome-molybdenum casting
CT-generated CAD-CAM model
27. One-stage pins and screws
Early 1960s pin, screw, and cylinder shaped implants
One piece and not submerged
Did not osseo-integration
Fibrous peri-implant membrane
Shock-absorbing claim
28. Blade Implants
1967 Linkow blade implant-in narrow ridge
Required shared support with natural teeth
1970 Roberts and Roberts – Ramus blade
implant (titanium)
31. The First Dental Implant Consensus Conference,
sponsored by the National Institutes of Health (NIH)
and Harvard University in 1978, was a landmark event.
“ Dental Implants: Benefits and Risks”
32. The Toronto Conference opened the door to prompt
widespread recognition of the Branemark implant.
The discovery of osseointegration has been one of the
most significant scientific break throughs in dentistry.
33. Endosteal root-form implants
1978Two-stage threaded titanium root-form implant
was first presented in North America by Branemark
(Toronto conference)
Terms “fixture”
First fixture was placed in 1965
Well-documented, long term prospective study
35. “In Bone”
1. Ramus concepts (Harold and Ralph Roberts)
2. Pin concepts (J. Scialom Michelle Chercheve)
3. Disk concepts (Gerard Scorteci)
4. Plateform concepts (Harold + Roberts/Linkow)
5. Cylindrical or root form concepts
36. Present Status
Many other root-forms have been introduced.
Body shaped competition
Surface competition – roughness
Varieties competition
Connection competition
37.
38. Dental Implants
Implant material should have suitable:
Mechanical strength,
Biocompatibility,
Structural Biostability in physiologic environments.
39. I. Modulus of elasticity
II. Tensile strength
III. Compressive strength
IV. Elongation
V. Metallurgy
40. BIOCOMPATIBILITY
“The ability of an implanted material to undergo
only a minimal amount of deterioration during service,
to produce only a minimal change in the body
environment, and to function satisfactorily in every
other respect.”
41. KEY FACTORS THAT INFLUENCE THE BENEFITS AND
MAINTENANCE OF BIOCOMPATIBILITY
Corrosion resistance
Cytotoxicity of corrosion products
Metal contamination
42. Biostability
Based on tissue response and systemic toxicity effects of
the implant:
Biotolerant
Bioinert
Bioactive
43. Long term effects
Biotolerant materials, such as polymethylmethacrylate
(PMMA), are usually characterized by thin fibrous
tissue interface.
Chemical product irritate surrounding tissues.
44. Long term effects
Bioinert materials, such as titanium and aluminum
oxide, are characterized by direct bone contact, or
osseointegration, at the interface under favorable
mechanical conditions.
Non-reactive
45. Long term effects
Bioactive materials, such as glass and calcium
phosphate ceramics, have a bone-implant interface
characterized by direct chemical bonding of the
implant with surrounding bone.
Free calcium and phosphate compounds at the surface.
46. Tissue response to implant materials
Most commonly used biomaterials:
Commercially pure (CP) titanium
Titanium-aluminum-vanadium alloy (Ti-6Al-4V)
Cobalt-chromium-molydenum (Co-Cr-Mo) alloy is
most used for subperiosteal implants.
47. Tissue response to implant materials
Calcium phosphate ceramics, Hydroxyapatite (HA),
used for augmentation material or coating on surface.
49. Advantages & disadvantages of implant
over conventional treatment
Implants do not involve preparation of the
adjacent teeth, they preserve the residual bone,
and excellent aesthetics can be achieved.
However, it is expensive, the patient requires
surgery, time consuming, and technically
complex.
50. INDICATIONS FOR TREATMENT
Factors precluding wear of a removable prosthesis
Poor anatomy for denture support
Poor oral muscular coordination
Poor mucosal tissue tolerance
Parafunctional habits
Unrealistic expectations
Hyperactive gag reflex
Psychological inability to wear
Unfavourable number and location of
abutments
53. Dr,salah hegazy
Diagnosis and
Treatment Planning
The evaluation of a patient as a suitable
candidate for implants should follow the same
basic format as the standard patient
evaluation, although some areas require
additional emphasis and attention:
I. Medical History.
II. Psychological Status.
III. Dental History.
54. Dr,salah hegazy
I. Medical History
The patient’s medical history may reveal a number
of conditions that could complicate or even contra-
indicate implant therapy. These include:
1. Bleeding disorders; Paget’s disease; A history of
radiation therapy in the maxilla or mandible region;
Uncontrolled diabetes; Epilepsy that presents with
more than one grand mal seizure per month;
2. In addition, there are a host of systemic medical
conditions, including steroid therapy,
hyperthyroidism, and adrenal gland dysfunction
3. Substance abuse including tobacco and alcohol
55. Diabetes
7% population is affected
Type I (insulin depandent) & Type II which effects
older age group & more common.
Blood glucose less than 150mg/dl with HbA1c value is
7. can be manage with normal protocols i:e
Early morning appointment
Stress reduction protocols
Infection control measures
Intravenous glucose for lengthy procedures
Do not prescribe steroids
For insulin controlled diabetes implant may be
contraindicated . This may not be the case for diet
56. Adrenal gland disorder
Epinephrine, nor epinephrine, corticosteroids &
mineralocorticoids are affected.
Complicate the implant placement by:
Inhibiting the response to inflammation
,pain & swelling
Steroids reduced the protein synthesis &
leukocytic activity that effects the
healing process & incresed tendency to
infection
57. Thyroid disorders
Large endocrine gland responsible for T3 & T4
hormones level in blood
Sensitivity to Epinephrine in LA & retraction cords
Stress related to implant surgery increase the
catecholomine level that leads to thyrotoxicosis or
thyroid storm symptoms includes:
Fever
Hypertension
arrhythmias
58. Hematological disorders
ANEMIA & POLYCYTHEMIA
Anemia characterized by reduced Hb level
Almost associated with every other blood disoder
Most common form is Iron deficiency anemia
For implants special considerations are required
including:
Suppressed bone marrow maturation
Increased trabecular pattern & reduced density of bone
therefore more time for osseointegration is required
59. LIVER DISEASES
Cirrhosis is the third leading cause of death
Alcohol, viruses are the common causes of liver
damage.
Reduced formation of fibrinogen & clotting proteins
Vit: K
Qualitative & quantitative defect of platelet
1.5 times Increased PT contra indicate the implant
placement.
60. OSTEOPOROSIS
Disease of bone metabolism.
Bone mineral density less than 2.5 standard deviation
of the young healthy women.
Common in post menopausal women because of low
estrogen level
Implant treatment need special considerations:
Implant body with greater width & threads plus some
surface coating to improve bone formation is selected
More healing time
Progressive loading of implant
Hormonal therapy does not effect the prognosis
61. OSTEOMALACIA
Vit: D deficiency
Oral findings are;
Dec: trabecular bone
Indistinct lamina dura
Inc: chronic periodontitis
Treatment includes: supplement oral vit: D (50,000
IU)
Don’t Give implant during active phase of the disease
62. Hyperparathyroidism
Hormonal problem
Sever skeletal depletion
Alveolar bone involvement is earlier than others bones
Ground glossy appearance b/c of altered trabecular
pattern
Loose teeth
Loss of lamina dura
Implant is contraindicated in active disease
63. Fibrous Dysplasia
Bone is replaced with the mass of fibrous connective
tissue.
Twice as common in women as men.
May effect single or multiple bones
Ground glass appearance
Movement of teeth
Inc: in trabeculation
Implant is used following the excision & stabilization
of bone in an affected area
64. Osteitis Deformans (Paget's Disease)
Metabolic disease
Slow apposition & resorption of bone
Characterized by:
Lion face
Bone pain
Diastemas of teeth
High level of serum alkaline phosphatase level
Normal serum calcium level
Implant is contraindicated
65. Multiple Myeloma
Plasma cell neoplasm originates in bone marrow.
Causes sever hypercalcemia, immune suppression,
anemia, thrombocytopenia & widesprad bone
destruction.
Found b/w 40 – 70 years of age.
Orally ( paresthesia, swelling, tooth mobility, gingival
enlargement)
Plasma cell malignancy
Case report has described a successful placement of
implants in this disease ( Sager RD 1990)
66. Osteomyelitis
Acute or chronic inflammatory bone disease.
Bacterial in nature
Radiographically…… poorly defined radiolucent area
with isolated segments of bone.
Caused by… odontogenic, periodontal infections,
trauma, implants, immuno-compromised state &
hypovascularized bone,
Common in mandible .
Treated by surgical drainage & I/V antibiotics
Relative contraindication to dental implants
67. Osteogenesis imperfecta
Inherent bone disease,
characterized by poor bone quality & fragility.
Bone fractures with poor healing .
Thin cortical & trabecular pattern of bone .
Dental implants need prolong healing time.
68. Cement-Osseous Dysplasia
Fibro-osseous lesion
Mandibular anterior region is affected.
Common in middle age women
Implants are only restricted in sclerotic phase of
disease where bone is hypovascularized
69. Prosthetic joints
450,000 joint arthroplasties are performed every year
in USA.
Dental implants may be used with other prosthetic
implants
The most critical period is up to 2 years after joints
placement where hematogenous infection can spread
b/c of dental implant placement.
Prophylactic antibiotic can prevent hematogenous
infection .
70. Ectodermal Dysplasia
Genetically inherent disorder affects 1 per 100,000 live
births.
May be X= linked or Autosomal
Characterized by hypodontia, hypohydrosis &
hypotrichosis.
Intra orally anodontia is common feature.
Conventional prosthodontics does not fullfill the
functional, esthetic & psychological requirements b/c
of anatomical variations.
success Rate of implants in Preadolescencents:
Age 7 – 11 yrs, 87% …….. Age 12 – 17 yrs, 90%......
Age above 17 yrs 97%
71. Ectodermal Dysplasia
Vertical growth results in submersion of implants
need prosthetic revision or possible use of longer
abutments
72. Sjogren's Syndrome
Autoimmune disease
Xerostomia & xeropthalmia
Healing response & integration of implants is not
affected.
non tissue borne prostheses reduced the prosthetic
complications in these pt:
73. Systemic Lupus Erythematosus
Autoimmune disorder
Dematological manifestation ( malar rash )
Oral vesicu lo-bulous lesions.
Treated with steroids & immunosuppresive drugs
No direct contraindications
74. scleroderma
Chronic disease chracterized by deposits of collagen
that cause musculoskeletal, pulmonary & GI
involvement.
Detal implants with fixed prostheses is recommended
since pt: is not be able to retrieve a removable
prostheses.
75. Rheumatoid Arthritis
Chronic inflammatory autoimmune disease
Affects muscles & joints
Loss of mobility & dexterity
Implants with fix restoration is indicated however
special attention should be given to treatment
medications as steroids may contraindicate the
implant placement.
76. Human Immunodeficiency Virus
HIV is a retrovirus resposible for AIDS.
Immune system get depressed
Pt: suffer life threatening opportunistic infections
Implant therapy is successful in HIV pts: however
current status of immune system & medications toxic
effects must be evaluated.
78. Tobacco/smoking
Pt should be informed abt detrimental effects of
implants
Recommend ceasation of smoking 2 weeks before
surgery & continue 8 weeks after the surgery.
Smoking is not the absolute contraindication
79. Alcohol use
Ethyl alcohol most widely mood altering drug in
world.
Associated with :
dec: osteoblasts functions
Dec bone formation
Dec wound healing
Inc parathyroid hormone secretion which lead to dec
bone density
81. IRRADIATION
Radiotherapy results in:
Progressive fibrosis of blood vessels & soft tissues
Xerostomia
Dec: bone healing quality.
Tissues get hypovascularized, hypoxic, hypocellular
These detrimental effects the wound repair & healing
significantly .
82. Implant Placement after Radiotherapy
The ability of implant to osseointegrate with the
irradiated bone depends on:
Area of irradiation
Radiation dosage
Time elapsed since radiation exposure
84. The time B/w radiotherapy &
implant placement
Controversial…..?
More the time elapsed better will be the prognosis.
Different periods to initiate the implant treatment are
recommended:
3 – 6 months ( King MA 1979)
12 months (Albrekttson T 1988)
& 24 months (Taylor TD 1993)
85. II. Psychological Status
Perception of outcome
hypercritical
demanding
unrealistic expectation
Time and expense
Aesthetics
Maintenance
86. III. Dental History
It is also vital to evaluate the patient’s chief
complaint, as it may have an equal bearing on
treatment outcome.
For example, the treatment plan
recommended to the patient desiring a more
secure lower denture will be quite different from
the one proposed to the patient seeking a fixed
and rigid appliance.
94. CT SCANE
Give best cross sectional assessment of an object
Irradiated portion of the jaw can be determine
Height of the available bone can be assessed by a
millimeter ruler.
Metallic restoration interferes the results.
Both quantity & density of bone can be assessed
Ideal for pre-maxillary region.
96. MRI
Has limited use in implantology
Expensive
No radiations
Qulity of bone is difficult to assess.
97. Implant Guidelines
surgical analysis -
implant length/diameter
determined by quantity of bone apical to
extraction site
use longest implant safely possible
diameter dictated by corresponding root
anatomy at crest of bone
98. Implant Guidelines
surgical analysis
treatment options
immediate - place implant at time of tooth
extraction
delayed immediate - 8-10 week delay
delayed - 9-10 months or longer
NOTE : immediate will not allow bone resorption, but delayed
allows bone fill for stabilization
99. Implant Guidelines
surgical analysis
proper surgical technique during implant placement is
critical
minimal heat generation important
100. esthetic analysis
implant emergence profile
restored implant should appear to
“grow” or emerge from the gingiva
very natural & desirable in appearance
101.
102. A direct structural and functional connection
between ordered living bone and the surface of a
load carrying implant
P-I Branemark
103. IV. Osseointegration
Definition:
A time-dependant healing process where by
clinically symptomatic rigid fixation of alloplastic
materials is achieved, and maintained, in bone
during functional loading.
(Zarb & Albrektson,1991)
105. 1. Implant biocompatibility
Materials used are:
Cp titanium (commercially pure titanium)
Titanium alloy (titanium-6aluminum-
4vanadium)
Zirconium
Hydroxyapatite (HA), one type of calcium
phosphate ceramic material
5. Plasma sprayed coating
106. Osseointegration
(A) Hematoma occurs near screw threads
(B) After 3 weeks – Osteoblasts begin forming spongy
bone
(C) After 4 months – spongy bone replaced by
compact bone Lamellar bone – strongest type of
bone, most desired next to implant
(D) Osseointegration failure
107. 2. Implant design (root-form)
Cylindrical Implant
Some investigators explain the lack of
bone steady state by overload due to
micromovement of the cylindrical design,
whereas others incriminates an
inflammation/infection caused particularly
by the very rough surfaces typical for these
types of implant.
Threaded Implant
In contrast, Threaded implants have
demonstrated maintenance of a clear steady
state bone response.
To enhance initial stability and increase
surface contact, most implant forms have
108. 3. Implant surface
The Pitch is the number of threads per unit
length, is an important factor in implant
osseointegration. Increased pitch and increased
depth between individual threads allows for
improved contact area between bone and
implant.
Moderately rough surfaces with 1.5µm also,
improved contact area between bone and
implant surface.
Reactive implant surface by anodizing
(Oxide layer) ,acid etching or HA coating
enhanced osseointegration
109.
110. Bone Quality
Quality I
Was composed of homogenous compact bone, usually found in
the anterior lower jaw.
Quality II
Had a thick layer of cortical bone surrounding dense
trabecular bone, usually found in the posterior lower jaw.
Quality III
Had a thin layer of cortical bone surrounding dense trabecular
bone, normally found in the anterior upper jaw but can also be
seen in the posterior lower jaw and the posterior upper jaw.
Quality IV
Had a very thin layer of cortical bone surrounding a core of
low-density trabecular bone, It is very soft bone and normally
found in the posterior upper jaw. It can also be seen in the
anterior upper jaw.
According to Lekholm and Zarb.,1985
113. 5. Surgical technique
Minimal tissue violence at surgery is essential for
proper osseointegration.
Careful cooling while surgical drilling is
performed at low rotatory rates
Use of sharp drills
Use of graded series of drills
Proper drill geometry is important, as
intermittent drilling.
The insertion torque should be of a moderate
level because strong insertion torques may result
in stress concentrations around the implant,
with subsequent bone resorption.
114. 6. Loading condition
A. Delayed / conventional loading :
B. Immediate loading:
C. Early loading
(prosthetic function within two months)
D. Progressive loading
115. Delayed / conventional loading :
Restoration is placed from 3 – 6 months
This is applicable for two stage
protocol
116. Immediate loading:
The biomechanical definition of immediate loading is
also debated: For some researchers,
The concept of immediate loading is
satisfied as soon as the coronal portion of the prosthesis
is inserted, even if it is kept out of occlusion.
• For others,
The term immediate loading can be applied
only if the prosthesis is subjected to occlusal forces as
soon as it is inserted.
To qualify as an immediately loaded implant, the
definitive prosthesis must be placed on the same day.
Still others accept a delay in loading of 48 hours to
72 hours.
117. Following are immediate-loading protocols •
A. Immediate occlusal loading vs immediate
functional loading
B. Immediate functional loading vs immediate
nonfunctional loading
118. Progressive loading
Misch first proposed the concept of progressive
or gradual bone loading during prosthetic
reconstruction to decrease crestal bone loss
and early implant failure of endosteal implants
in 1980 based on empirical information.
98.9% survival at Stage II uncovery followed
with a progressive loading format and found no
early loading failures during the first year of
function.
120. Progressive loading protocol (TIME)
• The macroscopic coarse trabecular bone heals about
50% faster than dense cortical bone.
• The healing time between the initial and second-stage
surgeries is kept similar for Dl and D2 bone and is 3 to
4 months.
A longer time is suggested for the initial healing phase
of D3 and D4 bone (5 and 6 months, respectively)
because of the lesser bone contact and decreased
amount of cortical bone to allow for the maturation
of the interface and the development of some lamellar
bone.
122. Progressive loading protocol (DIET)
• The patient is limited to a soft diet such as pasta and
fish, from the initial transitional prosthesis delivery
until the initial delivery of the final prosthesis.
• After the initial delivery of the final prosthesis, the
patient may include meat in the diet, which requires
about 21 psi in bite force.
The final restoration can bear the greater force without
risk of fracture or uncementation. After the final
evaluation appointment, the patient may include raw
vegetables, which require an average 27 psi of force. A
normal diet is permitted only after evaluation of
the final prosthesis function, occlusion, and
proper cementation.
123. Progressive loading protocol (OCClUSAl.
MATERIAL)
Using acrylic as the occlusal material, with the benefit
of a lower impact force than metal or porcelain.
Either metal or porcelain can be used as the final
occlusal material.
If parafunction or cantilever length cause concern
relative to the amount of force on the early implant-
bone interface, the dentist may extend the softer diet
and acrylic restoration phase several months. In this
way, the bone has a longer time to mineralize and
organize to accommodate the higher forces.
124. Progressive loading protocol
(OCCLUSION)
(step 1):
No occlusal contacts are permitted during initial
healing.
(step 2).
The first transitional prosthesis is left out of
occlusion in partially edentulous patients The occlusal
contacts then are similar to those of the final restoration
for areas supported by implants.
(step 3).
However, no occlusal contacts are made on
cantilevers The occlusal contacts of the final restoration
follow the implant protective occlusion concepts.
126. Progressive loading protocol
(PROSTHESIS DESIGN)
Its purpose is to splint the implants together, to reduce
stress by the mechanical advantage, and to have
implants sustain masticatory forces solely from
chewing.
In the second acrylic transitional restoration,
occlusal contacts are placed on the implants with
occlusal tables similar to the final restoration but with
no cantilevers in nonesthetic regions.
In the final restoration, narrow occlusal tables and
cantilevers are designed with occlusal contacts
following implant-protective occlusion guidelines.
127. implant-protective occlusion
Concept was developed by MISCH
Concept refers to an occlusal plane that is often
unique & specifically designed for the restoration
of endosteal implants, providing an environment
for improved clinical longevity of both implant &
prosthesis
128. implant-protective occlusion
The salient features are:
Using wider width of dental implant whenever
possible.
Anterior teeth should disclude the posterior
teeth.
Absence of lateral contacts in excursion.
All occlusal contacts more medial than the natural
teeth.
A reduced width of occlusal table
129. V. Biomechanics of osseointegrated
implant.
In all incidences of clinical loading, occlusal forces are
first introduced to the prosthesis and then reach the
bone implant interface via the implant. So far, many
researchers have, therefore, focused on each of these
steps of force transfer to gain insight into the
biomechanical effect of several factors such as
Force directions and magnitudes,
Prosthesis type,
Prosthesis material,
Implant design,
Number and distribution of supporting implants,
Bone density, and
The mechanical properties of the bone-implant
interface.
131. Parts of Implant
1. Implant body or fixture
The implant body is the
component that is placed
within the bone during first
stage of surgery. It could be
threaded or non threaded.
The implant bodies may be
coated with hydroxyapatite
or titanium particles to
incorporate microscopic
component into them.
132. Prosthetic Component Cont….
2. First stage cover (Healing screw)
During the healing phase ,this screw is
normally placed in the superior
surface of the body.
The functions of this component are:
• Facilitates the suturing of soft
tissue.
• Prevents the growth of tissue
over the edge of the implant.
133. Prosthetic Component Cont…
3. Second stage permucosal extension or
healing abutment (healing cap)
After a prescribed healing period, a second stage
procedure may be performed to expose the implant
and/or attach atransepithelial portion.
This transepithelial portion is termed a permucosal
extension because it extends the implant above the soft
tissues and results in the development of a permucosal
seal around the implant. This implant component is also
called a healing abutment because stage II uncovery
surgery often uses this device for initial soft tissue healing.
134. Prosthetic Component Cont….
4. Abutment
It is the portion of the implant
that supports or retains a
prosthesis or implant
superstructure.
135. Three main categories of implant
abutment are described according
to the method by which the
prosthesis or superstructure is
retained to the abutment.
A. An abutment for screw retention
B. An abutment for cement
retention
C. An abutment for attachments
136. Prosthetic Component Cont….
5. Impression coping or impression posts
It is a part of the implant that facilitates the transfer
of the intraoral location (of the implant or
abutment) to a similar position on the cast.
Therefore it can also be called as implant body
transfer coping or abutment transfer coping.
It has two types:
Transfer impression
Pick type impression
139. Prosthetic Component Cont . . .
6. Laboratory analogues
An analogue is something that is similar or analogous to
something else. An implant analogue is used in the
fabrication of the master cast to replicate the
retentive portion of the implant body or abutment
(implant body analogue, implant abutment
analogue). After the master impression is obtained
the corresponding analogue( e.g., implant body,
abutment for screw) is attached to the transfer coping
and the assembly is poured in stone to fabricate the
master cast.
140. Prosthetic Component Cont . . .
7. Prosthesis retaining
screw
A screw retained prosthesis
or superstructure is
secured to the implant
body or abutment with a
prosthetic screw.
141. IMPLANT SUPER STRUCTURES
A super structure is the prosthetic component fabricated
over the implant after its placement.
Commonly used super structures include
1. Overdentures,
2. Fixed partial dentures/bridges
3. Single Crown
142. IMPLANT SUPER STRUCTURES
1 - Implant Supported
Over Dentures
They can be either a
complete or a partial
over denture. The
implants are placed on
suitable sites in the
edentulous ridge. The
implant abutments may
either be present
individually or be
connected to one
another with a bar.
143. IMPLANT SUPER STRUCTURES
2 – Implant Supported
Fixed Partial Dentures
These may be either pure
implant supported or a
combination of implant
and tooth supported
fixed bridges.
146. C.Misch in 1989 reported five prosthetic options
in implant dentistry.
Of the five, the first three are fixed prosthesis (FP)
that may be partial or complete replacements,
which in turn may be cemented or screw
retained.
The remaining two are removable prosthesis (RP)
that are classified on the support derived.
147. PROSTHETIC OPTIONS IN
IMPLANT DENTISTRY Cont. . .
• FP-1: Fixed prosthesis; replaces only the crown; looks
like a natural tooth.
148. PROSTHETIC OPTIONS IN
IMPLANT DENTISTRY Cont. . .
• FP-2: Fixed prosthesis; replaces the crown and a portion
of the root; crown contour appears normal in the occlusal
half but it is elongated or hypercontoured in the gingival
half.
149. PROSTHETIC OPTIONS IN
IMPLANT DENTISTRY Cont. . .
• FP-3: Fixed prosthesis; replaces missing crowns and
gingival color and the portion of the edentulous side;
prosthesis most often uses denture teeth and acrylic
gingiva, but may be made of porcelain.
150. PROSTHETIC OPTIONS IN
IMPLANT DENTISTRY Cont. .
• RP-4: Removable prosthesis; overdenture supported
completely by implants.
151. PROSTHETIC OPTIONS IN
IMPLANT DENTISTRY Cont. .
• RP-5: Removable prosthesis; overdenture supported by
both soft tissue and implants.
152. Ideal design of implant
and tissue supported
overdentures;
Internal of overdenture;
154. 1. Number of implants abutment
2. Location of implants
3. Quality of bone
4. Amount of bone
5. Amount of circumoral activity
155. Quasi- general formula i:e
• five implants b/w two mental foramina to support 10 – 12
units fixed mandibular prosthesis.
•& six implants for maxilla
formula did not address the following considerations:
Arch form ( Flat versus curvature)
Length of implants
Length of cantilever
Occlusal forces
156. Location of implants
Implant distribution is more favorable in curved
arches since it provides :
More occlusal units
& optimal cantilever design
Flat arches are favorable for overdentures
158. Quantity of bone
10 mm of vertical height of the bone is minimally
required
Bone grafting, sinus lift, frozen bone use to improves
the quantity of bone
159. Amount of circumoral activity
This would effect the choice of maxillary prosthesis
Where high lip line & advance residual ridge
resorption will require the use of visible labial flange
to compensate bone resorption .
This design demands high value for hygiene
maintenance & preclude fixed option
161. Treatment Planning Determinants
1. Changes in Oral Structures in Edentulism
2. Posterior Ridge Anatomy
3. Occlusal Forces
4. Quality, Location and Quantity of Bone
5. Implant Size
6. Implant Location
7. Arch configuration
8. "Mapping" the Mandible
9. Cantilevering
162. 1. Changes in Oral Structures in
Edentulism
With successive denture treatments, it is
common for the vertical dimension of occlusion
to decrease as bone resorbs. This promotes an
increased tendency toward a skeletal Class III
relationship.
163. Posteriorly, poor ridge height, inadequate
attached gingiva and compromised ridge
shape cause increased horizontal movement of
the prosthesis. This increases the lateral
forces that are brought to bear on the anterior
implants, and will affect bar and prosthesis
design.
2. Posterior Ridge Anatomy
165. 3. Occlusal Forces
The maximum bite force of subjects with a
mandibular denture supported by implants is
60 to 200% higher than that of subjects with a
conventional denture
Edentulous patients that are predisposed to
clenching and bruxing may be given the
necessary "tools" to begin parafunctional
habits once the implant bar is secured in
place.
166. The minimum buccal-lingual thickness of
osseous tissue required to successfully place an
implant is 5 mm.
In order to achieve a 5.0 mm "flat" base, either
the anterior ridge crest peak must be removed or
a bone graft must be considered.
4. Quality, Location and Quantity of
Bone
167. 5. Implant Size.
The greater the surface area of the implant-
bone system, the less concentrated the force
transmitted to the crest of bone at the implant
interface. Similarly, the greater the surface area
of the implant-bone system, the better the
prognosis for the implant.
For each 0.25 mm increase in diameter, the
surface area of a cylinder increases by more
than 10 per cent;
For each 3.0 mm increase in length , the surface
area of a cylinder increases by more than 10 per
cent.
169. 6. Implant Location
Ideally, occlusal forces should be directed
along the long axis of the implants. Therefore
,The angle of the osseous ridge crest is a key
determinant of implant angulation.
the distance between an implant and any
adjacent "landmark" (natural tooth or another
implant), which should be not less than 2.0
mm.
170. The angle of the osseous ridge crest is a key
determinant of implant angulation.
171. 7. Arch configuration
Mandibular arch forms may be classified as
tapered or square.
With tapered arch forms, the most posterior
right and left implants in a four-implant
treatment are often placed well around the
"turn" of the arch, creating a "U" shaped design
that is well suited to cantilevering,
With a square arch, the four implants are
usually placed in a relatively straight line. This
"straight line" bar design is not well suited to
cantilevering.
172. 8. "Mapping" the Mandible
The anterior symphysis can be divided into five
geographic sites:
A point, 6.0 mm anterior to each mental
foramen, determines the most posterior
boundaries, right and left.
Another possible implant location occurs at the
midline.
Two additional sites are chosen on each side of
the midline, spaced equidistantly between the
midline and the respective distal sites.
174. Factors which helps in determining the appropriate
cantilever than a suggested formula.
The number of implants,
Their respective lengths and locations,
The quality of bone support,
The posterior ridge anatomy,
Occlusal forces,
And the opposing dentition
175. 9. Cantilevering
suggested formula.
One method is to draw a line through the
most anterior implant, and another
through the two most posterior implants.
The distance between the two lines can
then be measured. A suggested
maximum cantilever would be 1.5 times
this distance.
176. Dr,salah hegazy
The distance between the
two lines can then be
measured. A suggested
maximum cantilever would
be 1.5 times this distance.
178. Treatment Planning
When all the diagnostic information has been
assembled, a variety of available treatment
options must be assessed:
1. One-Implant Overdenture
2. Two-Implant Overdenture
3. Three-Implant Overdenture
4. Four-Implant Overdenture
5. Five-Implant Overdenture
179. One-Implant Overdentures
Indications:
The maladaptive or dissatisfied denture
patient who demands greater stability and
oral comfort,
Elderly patients desiring a more stable
mandibular denture,
Or, as a minimal implant treatment objective
for the partially edentulous patient with
severely compromised teeth in which
removal would convert a patient to a fully
edentulous state
181. In the two-implant over-denture, an
attachment is used to greatly enhance the
retentive potential of what is essentially a
tissue-supported prosthesis.
If only two implants are placed, which are
13mm long or longer, and they are in
dense bone, they can be left as individual
supporting units with little risk.
. Two-Implant Solitary Overdenture
184. 2. Two-Implant Bar Overdenture
If the two implants are 10 mm long or
shorter, or the bone quality is
compromised, then ideally:
They should be splinted.
They should be at least 10 mm apart (in
order to allow room for a clip or fastening
mechanism)
They should be no further than 18 mm
apart in order to limit bar flexure.
187. 3. Three-Implant Overdenture
The three-implant overdenture is
still essentially a tissue-
supported prosthesis with
enhanced retention supplied by
the attachment/bar complex.
189. 4. Four-Implant Overdenture
At this level, the prosthesis begins to
derive a larger part of its support and
retention from the implant/bar complex,
and the importance of tissue support
decreases.
Also, the attachments selected for a four-
implant bar over-denture can be more rigid,
as the torquing forces generated by the
prosthesis will be better tolerated.
This number allows for some "insurance"
in case one implant fails to integrate.
192. 5. Five-Implant Overdenture
At this level, a prosthesis can be fabricated
that is completely implant supported and
retained, if the AP spread of the implants is
adequate.
The decision to fabricate a bar over-denture
over five implants, rather than a fixed
detachable restoration, usually relates to the
patients’ ability to maintain proper oral
hygiene.
195. PROSTHETIC
PROTOCOL
Overdenture abutments were cemented or scrowed into
the implants.
Pressure indicating paste was placed on each
overdenture ball.
The denture was seated so that the pressure indicating
paste could mark the exact location of the overdenture
abutments. Then, a recess was cut into the denture at
each abutment location
The resulting depressions in the mucosal aspect of the
denture were lined with polyvinylsiloxane material and
seated in the patient's mouth.
The denture was either lined with a lab-processed
material or O-rings were used for retention.
200. The denture was either lined with a
lab-processed material or O-rings were
used for retention
201.
202. MAINTENANCE & RECALL
Recall appointmens should be
after every 3-4 months
Scaling and proper cleaning is
done with only plastic disposible
instruments
Use of steel probes and other
instruments is prohibited
Home care aids like flosses
interproximal brushes and water
jets should be advised for patients
to use at home
217. Second stage
Loose implant
Excess bone coverage
Exposed threads
Coverscrew problems
COMPLICATIONS
218. STAGE TWO SURGERY
Wrong abutment length
Faulty abutment seating
Retained sutures
Gingival hyperplasia
Mobile tissue
Destroyed cover screw hex
Failure of integration
219. FAULTY PLACEMENT
Labial / buccal
Lingual
Too close
Straight line in mandibular anteriors
Angulation
Divergence
Correct by use of a surgical template
224. PROSTHODONTIC
Avoid premature loading
Passive fit
Good design
Good oral hygiene
Loss of integration
Soft tissue problems
Oral hygiene and maintenance
Retrievable vs cemented
226. MANAGEMENT OF FAILURE
Failing implants FAIL
Removal
Abandon
Alternative site
Larger diameter
Replacement after healing
227. PROSTHODONTIC PROBLEMS
AND COMPLICATIONS
TYPE
Structural
Cosmatic
Functional
DESCRIPTION
Prosthesis fracture
Fracture of prosthesis rataining
screw
Fracture of implant
Fracture of abutment
As perceived by patient and dentist
Speech problems
Transient muscle discomfort or TMJ
disorders
228. SURGICAL PROBLEMS AND
COMPLICATIONS
TIME
Stage 1 surgery
post- stage 1 surgery
Stage 2 surgery
Delayed complications
DESCRIPTION
Unfavorable implant
position/allignment
Swelling or echymosis.
infection and neuroapthy
Failure of osseointegration
Unfavorable position or angle
makes the implant unusable
Component fracture
Soft tissue complications