Chhattishgarh , nursingcollege
Dhanora, bhilai
SUBJECT - COMMUNITY HEALTH NURSING – I
TOPIC - NATIONAL PROGRAMME FOR THE PREVENTION &
CONTROL OF DEAFNESS
SEMINAR ON
PRESENTATED TO PRESENTATED BY
MR. PAWAN GAJPAL
SIR
( H.O.D. ) OF C.H.N.
MR CHANDRAHAS
BSC NURSING
5TH
SEM
13TH
BATCH CNC BHILAI
3.
INTRODUCTION
Hearing loss isthe most
common sensory deficit in
human today as per who
estimate in india there are
approximately 63 million people.
Who are suffering from significant
editory impairment this places the
estimated prevalence all 6.3 % in
india population .
4.
DEFINITION-
According to K.KGulani
Hearing impairment is when an individual loses the ability
to hear in either one or both ears The level of impairment
can vary form mild to 8 severe or total of hearing.
According to BT Basavanthappa“
A Person who is not able to hear as well Someone with
normal hearing – hearing three holds of 25db or better in
both ears is said to have hearing loss.
5.
INCIDENCE -
Hearing impairmenthas been reported
to occur in 3 of every 1000 births
the Globally around 1.5 billion People have some degree
of heaving loss and Number is expected to increase to 2.5
billion by 2050
This mean that move than 7oo million people may Need
hearing rehabilitation by then.
6.
CLASSIFICATION
1 ) CONDUCTIVEHEARING LOSS
2 ) SENSORINEURAL HEARING LOSS
3 ) MIXED HEARING LOSS
4) CENTRAL / FUNCTIONAL HEARING LOSS
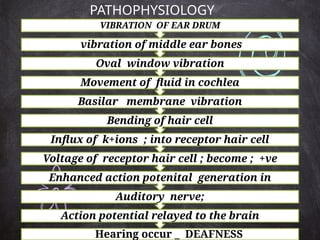
Action potential relayedto the brain
Auditory nerve;
Enhanced action potenital generation in
Voltage of receptor hair cell ; become ; +ve
Influx of k+ions ; into receptor hair cell
Bending of hair cell
Basilar membrane vibration
Movement of fluid in cochlea
Oval window vibration
vibration of middle ear bones
VIBRATION OF EAR DRUM
PATHOPHYSIOLOGY
Hearing occur _ DEAFNESS
EFFECTIVE STRATEGIESFOR REDUSING
HEARING LOSS AT DIFFRENT STAGES OF THE
LIFE COURSE INCLUDE:
#Immunization
# Good maternal and Childcare Practices
#Genetic Counseling
# Identification and Management of Common1 Ear
Condition
# occupational hearing Conservation Programme for
Noise and Chemical exposure
#Safe listening Strategies for the reduction of
exposure to bad Sounds
#Rational use of medicine to Prevent ototoxic
hearing loss
NATIONAL PROGRAMME FOR
PREVENTIONAND CONTROL OF DEAFNESS
Hearing loss is the most common sensory deficit in
humans today. As per WHO estimates in India, there
are approximately 63 million people, who are
suffering from significant auditory impairment;
this places the estimated prevalence at 6.3% in
Indian population.
As per NSSO survey, currently there are 291
persons per one lakh population who are suffering
from severe to profound hearing loss (NSSO, 2001).
Of these, a large percentage is children between the
ages of 0 to 14 years.
29.
OBJECTIVES OF THEPROGRAMME-
•To prevent avoidable hearing loss on account of
disease or injury .
• Early identification, diagnosis and treatment of ear
problems responsible for hearing loss and deafness.
• To medically rehabilitate persons of all age groups,
suffering with deafness.
• To strengthen the existing inter-sectoral linkages
for continuity of the rehabilitation programme, for
persons with deafness.
•To develop institutional capacity for ear care
services by providing support for equipment,
material and training personnel.
30.
Long term objective:
•To prevent and control major causes of
hearing impairment and deafness, so as to
reduce the total disease burden by 25% of
the existing burden by the end of 12th five
year plan.
31.
COMPONENTS OF THEPROGRAMME -
Manpower training & development –
For - prevention, early identification and management of
hearing impaired and deafness cases, training would be
provided from medical college level specialists (ENT and
audiology) to grass root level workers.
Capacity building - for the district hospital, community
health centers and primary health center in respect of ENT/
audiology infrastructure.
Service provision-Early detection and management of
hearing and speech impaired cases and rehabilitation, at
different levels of health care delivery system.
Awareness generation through IEC/ BCC activities- for
early identification of hearing impaired, especially children
so that timely management of such cases is possible and to
remove the stigma attached to deafness.
32.
STRATEGIES-
• To strengthenthe service delivery for ear
care
• To develop human resource for ear care
services
• To promote public awareness through
appropriate The and effective IEC
strategies with special emphasis neck on
prevention of deafness
• To develop institutional capacity of the
district hospitals, community health
centers and primary health centers
CONCLUSION-
The national programmefor prevention and control of
deafness
( NPPCD ) aims to reduce the number of people with hearing
loss and deafness the programme also seeks to improve the
quality of care for people with hearing loss and deafness.








































![hepatitis condition and the types of problems [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hepatitisvinay1-250305165228-f67bb5bb-thumbnail.jpg?width=640&height=640&fit=bounds)




























