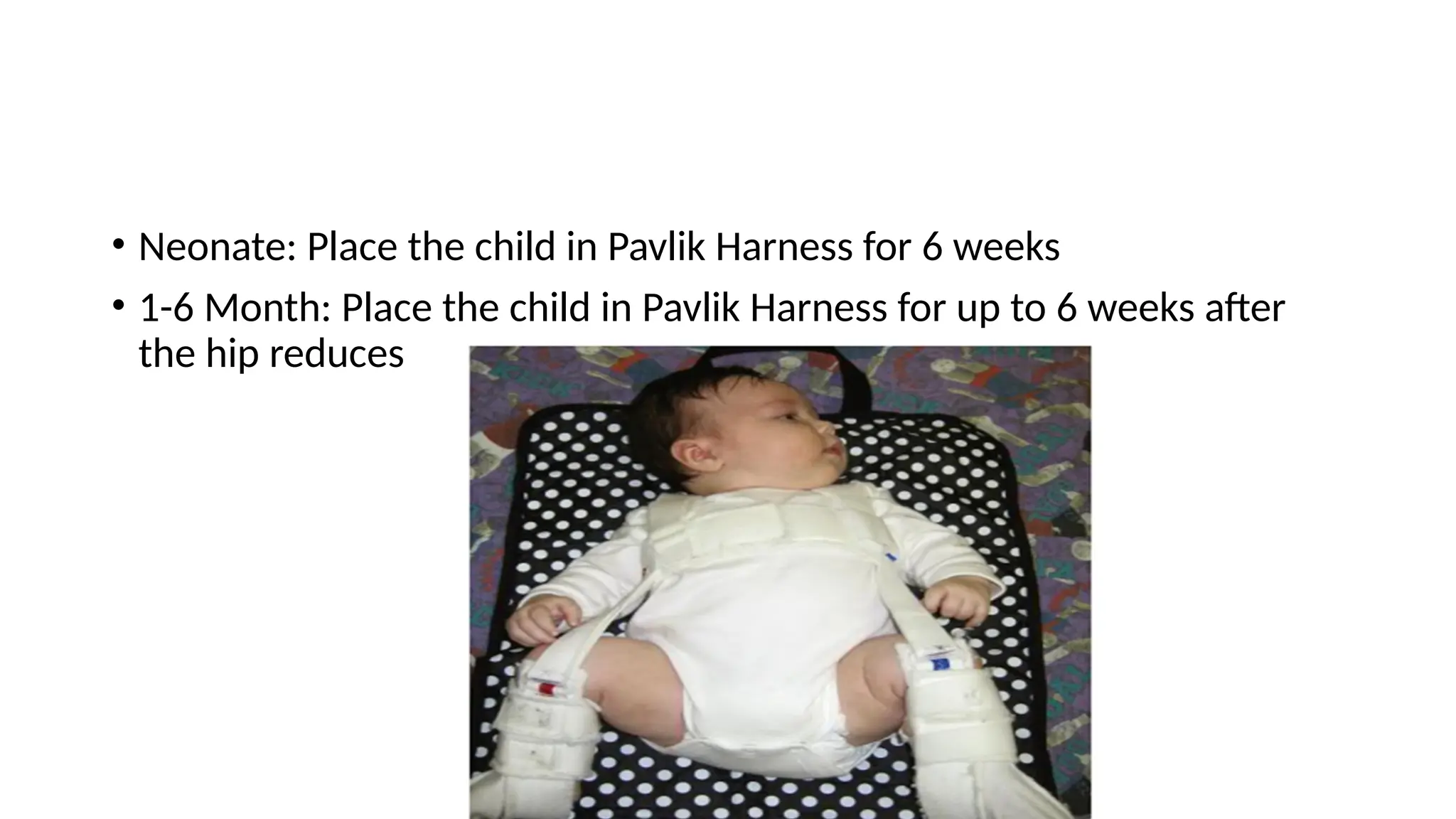
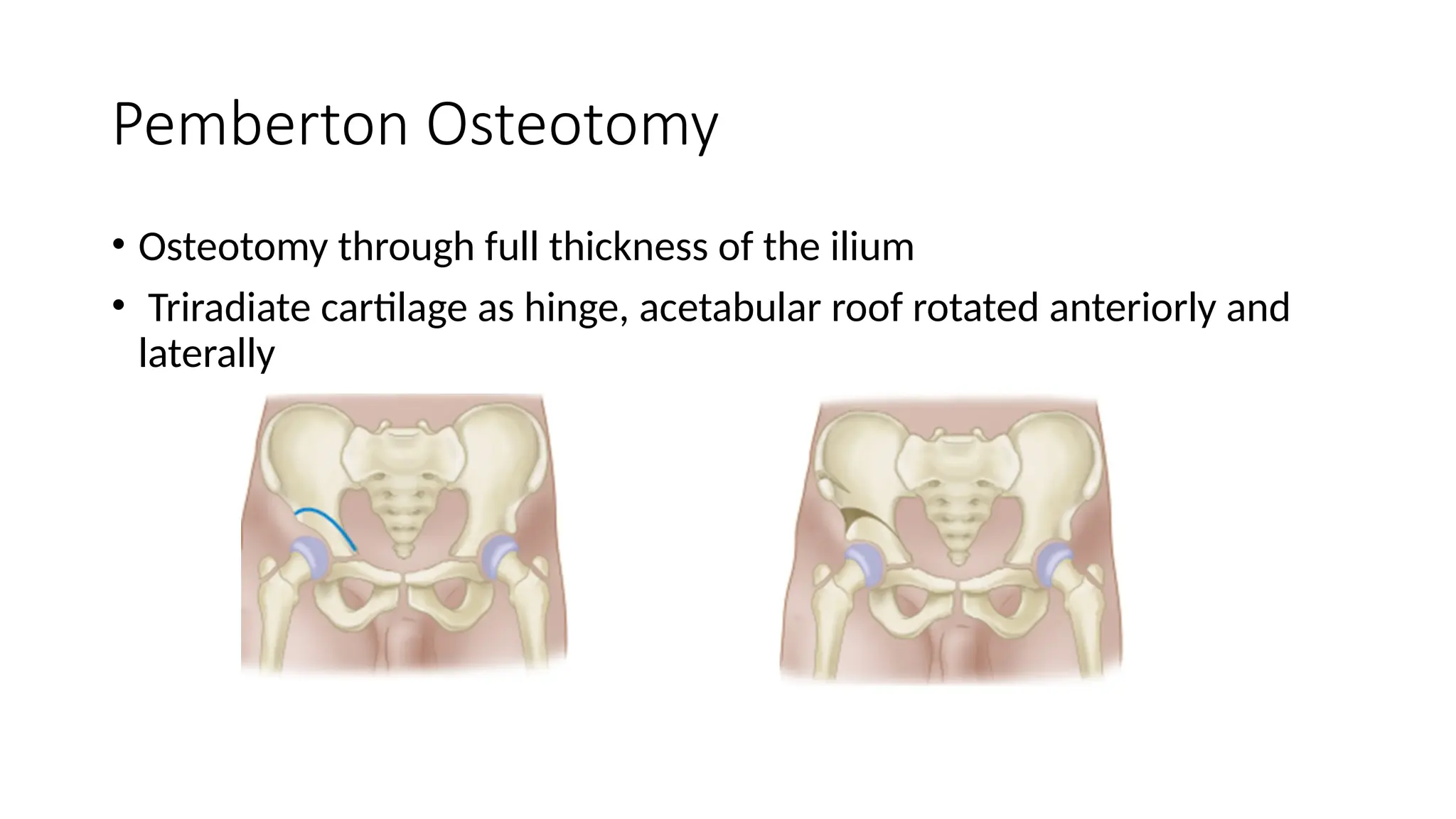
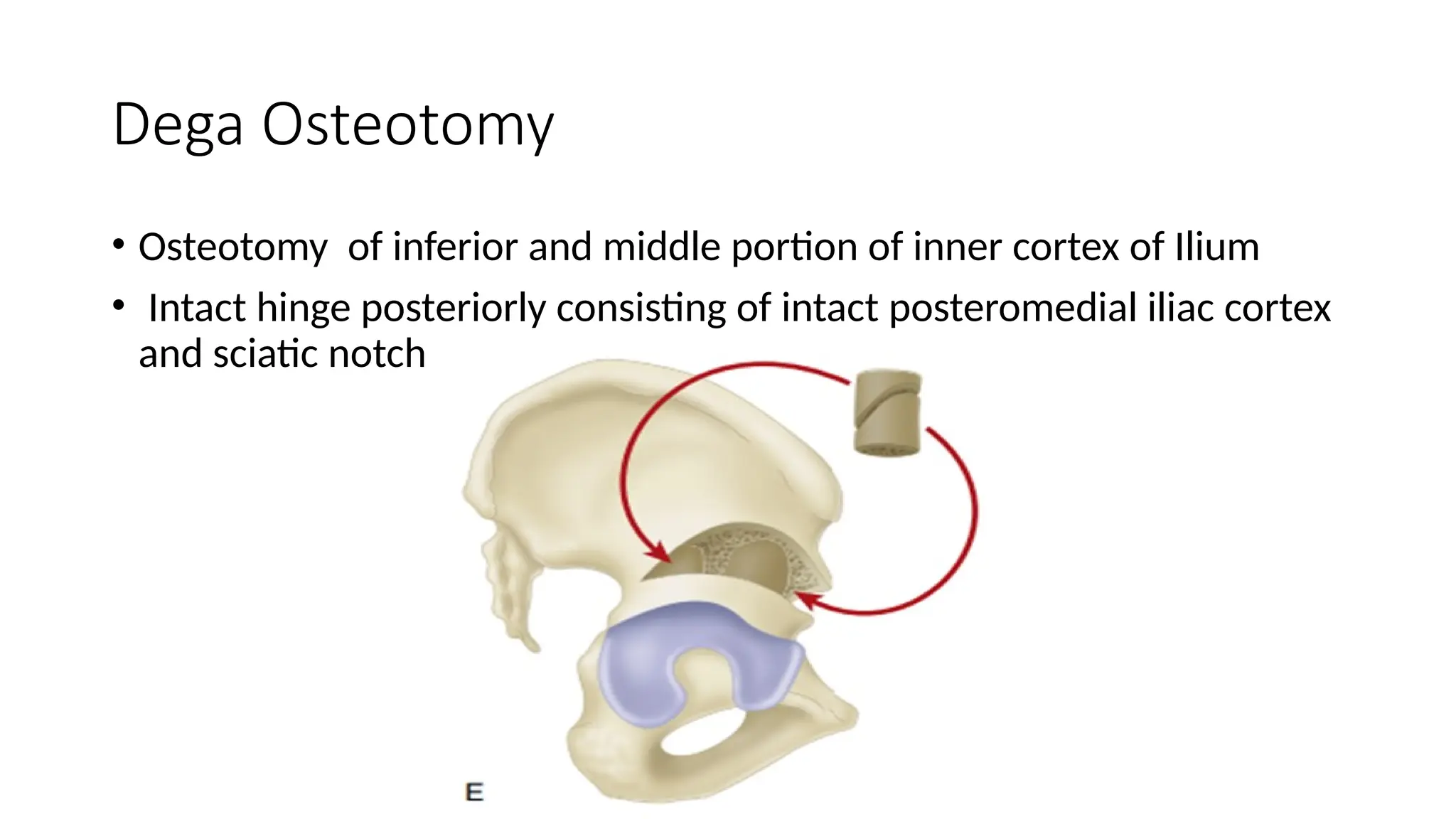
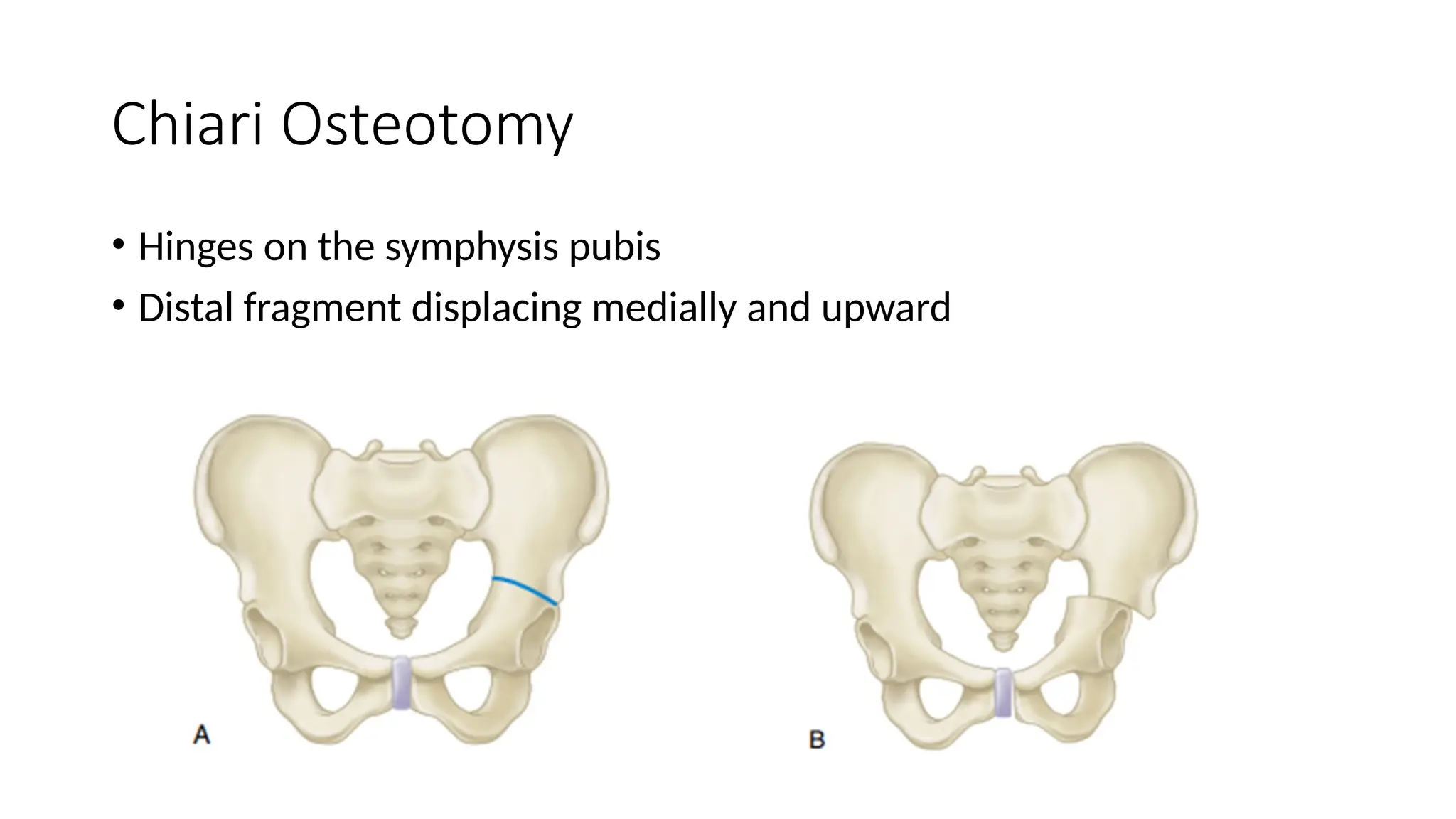
The document outlines the treatment protocol for developmental dysplasia of the hip (DDH) in neonates and young children, emphasizing the use of Pavlik harnesses and various surgical options depending on the child's age and condition. It details follow-up procedures, closed and open reduction techniques, and various osteotomy options for cases not stable with conservative management. The approach varies significantly from infancy through age six, necessitating a tailored treatment plan based on the child's ongoing assessment.