Basic Wheelchair PrescriptionWriting
Various wheelchair types are available, with a wide range of
options in the market today.
Wheelchair prescription should:
Maximize functional independence with ADLs
Minimize the risk of secondary injuries
Correct or accommodate for skeletal deformities
Ensure comfort
3.
Basic Wheelchair PrescriptionWriting
Maximize functional independence with ADLs
The wheelchair or seating system should enable individuals to perform
the activities of daily living (ADLs) that are important to them with
minimal to no assistance and with the least amount of energy
expenditure.
Types of activities can include transfers, personal needs (e.g., bathing,
toileting), working, preparing meals, cleaning, and shopping.
4.
Basic Wheelchair PrescriptionWriting
Minimize the Risk of Secondary Injuries
Tips and falls account for more than 70% of wheelchair-related
accidents.
It is imperative that individuals be provided with mobility devices that comply
with internationally recognized wheelchair standards and can be safely
operated.
Seat belts, wheel locks, and a properly-adjusted wheelchair can
prevent serious wheelchair-related injuries.
Pressure ulcers are also a significant risk for those who use wheelchairs.
Advanced cushion designs and seat functions can provide adequate
pressure relief for persons who cannot independently off-load the buttocks.
Shoulder pathology and nerve compression injuries at the wrist are
common among wheelchair users.
Using proper wheelchair propulsion biomechanics and an optimal
wheelchair setup can help delay the onset of overuse injuries.
5.
Basic Wheelchair PrescriptionWriting
Correct or Accommodate for Skeletal Deformities
When the skeletal deformity is “flexible,” the seating system should
correct the deformity, and when the skeletal deformity is “fixed,” the
seating system should accommodate the deformity.
The seating system should not create a “new” deformity such as a
sacral posture (posteriorly tilted pelvis), which results from sitting in a seat
that is too long or using footrests that do not account for tight
hamstrings.
6.
Basic Wheelchair PrescriptionWriting
Ensure Comfort
Along with mobility, comfort has been reported as the most important
attribute or function of a wheelchair.
Research has shown that most wheelchair users experience regular
discomfort. Many either ignore it or seek relief by getting out of the
wheelchair, using pain medications, or doing weight shifting (either
manually or with tilt and recline).
A wheelchair that allows for “fine-tuning” of the adjustments provides
greater options for achieving comfort, as well as meeting the
individual’s postural and pressure needs.
7.
Basic Wheelchair PrescriptionWriting
Prior to wheelchair prescriptions, the clinician should:
Complete a full medical history
Assess the patient’s strength, endurance, ROM, head and trunk control,
skin integrity, sensation, sitting balance
Assess the patient’s current functional status and future rehabilitation
goals
8.
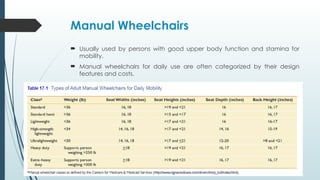
Manual Wheelchairs
Usuallyused by persons with good upper body function and stamina for
mobility.
Manual wheelchairs for daily use are often categorized by their design
features and costs.
9.
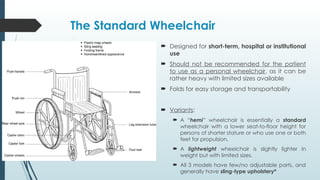
The Standard Wheelchair
Designed for short-term, hospital or institutional
use
Should not be recommended for the patient
to use as a personal wheelchair, as it can be
rather heavy with limited sizes available
Folds for easy storage and transportability
Variants:
A “hemi” wheelchair is essentially a standard
wheelchair with a lower seat-to-floor height for
persons of shorter stature or who use one or both
feet for propulsion.
A lightweight wheelchair is slightly lighter in
weight but with limited sizes.
All 3 models have few/no adjustable parts, and
generally have sling-type upholstery*
10.
The ‘Lighter &Daily Use’ Wheelchairs
The high-strength lightweight and ultralight
wheelchairs are designed for long-term use by
individuals who spend more than a couple of
hours each day in a wheelchair.
They have adjustable features, especially the
ultralights, and provide many advantages
over other wheelchair types (which will be
highlighted later)
11.
The ‘Heavy Duty’Wheelchairs
The heavy duty and extra-heavy duty
wheelchairs pertain to persons who weigh
more than 250 lbs (~113kg)
They are heavier than the wheelchairs in other
classes, to support the extra load.
The expanded class of “extra–heavy-duty”
wheelchairs, referred to as bariatric
wheelchairs, are built to support individuals
who weigh between 300 and 1000 lbs.
12.
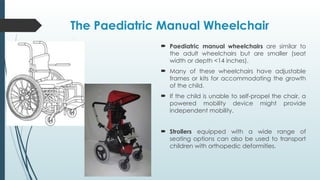
The Paediatric ManualWheelchair
Paediatric manual wheelchairs are similar to
the adult wheelchairs but are smaller (seat
width or depth <14 inches).
Many of these wheelchairs have adjustable
frames or kits for accommodating the growth
of the child.
If the child is unable to self-propel the chair, a
powered mobility device might provide
independent mobility.
Strollers equipped with a wide range of
seating options can also be used to transport
children with orthopedic deformities.
13.
The Sports Wheelchair
Sports wheelchairs are designed specifically
for participating in such athletic endeavors as
racing, rugby, tennis, and basketball.
Made of lightweight materials, and usually
have very aggressive axle positions and
camber.
Some of the sport wheelchairs have only one
wheel in the front, which allows quick turns
and enhanced maneuverability.
14.
Add-Ons: Hand Cycles
Wheelchairs equipped with arm crank
mechanisms (called hand cycles) for exercise
are available from many manufacturers.
Arm crank exercise can help improve
cardiovascular fitness, with research showing
that arm cranking is more efficient and less of
a physical strain than conventional wheelchair
propulsion
15.
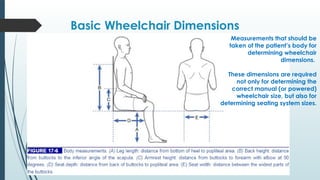
Basic Wheelchair Dimensions
Measurementsthat should be
taken of the patient’s body for
determining wheelchair
dimensions.
These dimensions are required
not only for determining the
correct manual (or powered)
wheelchair size, but also for
determining seating system sizes.
16.
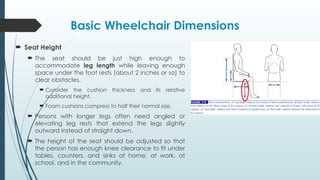
Basic Wheelchair Dimensions
Seat Height
The seat should be just high enough to
accommodate leg length while leaving enough
space under the foot rests (about 2 inches or so) to
clear obstacles.
Consider the cushion thickness and its relative
additional height.
Foam cushions compress to half their normal size.
Persons with longer legs often need angled or
elevating leg rests that extend the legs slightly
outward instead of straight down.
The height of the seat should be adjusted so that
the person has enough knee clearance to fit under
tables, counters, and sinks at home, at work, at
school, and in the community.
17.
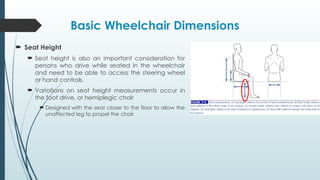
Basic Wheelchair Dimensions
Seat Height
Seat height is also an important consideration for
persons who drive while seated in the wheelchair
and need to be able to access the steering wheel
or hand controls.
Variations on seat height measurements occur in
the foot drive, or hemiplegic chair
Designed with the seat closer to the floor to allow the
unaffected leg to propel the chair
18.
Basic Wheelchair Dimensions
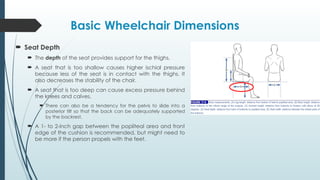
Seat Depth
The depth of the seat provides support for the thighs.
A seat that is too shallow causes higher ischial pressure
because less of the seat is in contact with the thighs. It
also decreases the stability of the chair.
A seat that is too deep can cause excess pressure behind
the knees and calves.
There can also be a tendency for the pelvis to slide into a
posterior tilt so that the back can be adequately supported
by the backrest.
A 1- to 2-inch gap between the popliteal area and front
edge of the cushion is recommended, but might need to
be more if the person propels with the feet.
19.
Basic Wheelchair Dimensions
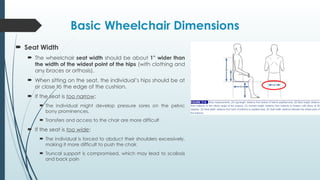
Seat Width
The wheelchair seat width should be about 1” wider than
the width of the widest point of the hips (with clothing and
any braces or orthosis).
When sitting on the seat, the individual’s hips should be at
or close to the edge of the cushion.
If the seat is too narrow:
The individual might develop pressure sores on the pelvic
bony prominences.
Transfers and access to the chair are more difficult
If the seat is too wide:
The individual is forced to abduct their shoulders excessively,
making it more difficult to push the chair.
Truncal support is compromised, which may lead to scoliosis
and back pain
20.
Basic Wheelchair Dimensions
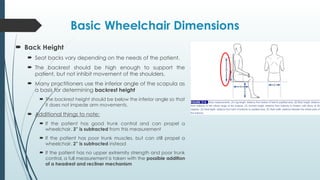
Back Height
Seat backs vary depending on the needs of the patient.
The backrest should be high enough to support the
patient, but not inhibit movement of the shoulders.
Many practitioners use the inferior angle of the scapula as
a basis for determining backrest height
The backrest height should be below the inferior angle so that
it does not impede arm movements.
Additional things to note:
If the patient has good trunk control and can propel a
wheelchair, 3” is subtracted from this measurement
If the patient has poor trunk muscles, but can still propel a
wheelchair, 2” is subtracted instead
If the patient has no upper extremity strength and poor trunk
control, a full measurement is taken with the possible addition
of a headrest and recliner mechanism
21.
Basic Wheelchair Dimensions
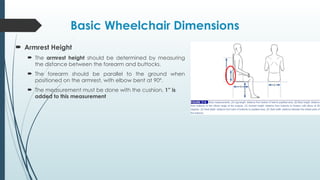
Armrest Height
The armrest height should be determined by measuring
the distance between the forearm and buttocks.
The forearm should be parallel to the ground when
positioned on the armrest, with elbow bent at 90º.
The measurement must be done with the cushion, 1” is
added to this measurement
22.
Wheelchair Seat Selection
The selection of a proper seat is important for stability,
comfort, ease of propulsion, and skin integrity.
There are various types of seats, each with their own
benefits and limitations, ranging from:
Vinyl sling seat easy to fold, easy to clean, and
lightweight
Solid seat firm but provides better postural control. It is
heavier and makes the chair more difficult to fold.
Patients should not sit directly on either seat. All
patients should receive some type of cushion.
24.
Recline and TiltBackrest Mechanism
These systems can be manually or power controlled and are
for patients who:
Are prone to skin pressure breakdown
Cannot sit fully erect
Have poor sitting balance and/or endurance
Have orthostasis
Have respiratory needs
The most important reason is to perform adequate weight shifts
and prevent skin breakdown.
These systems add weight + bulk, and require a longer wheel
base to maintain adequate stability when the chair is reclined.
25.
Recline and TiltBackrest Mechanism
A. Recliner Back
Semi recliner can be adjusted to 30º. The chair is 3” longer
and more difficult to propel
Full recliner reclines to 90º and is 6” longer than the
standard chair
Shear forces are increased when reclined.
There are low and zero shear recliners; however no system will
completely eliminate shear forces
26.
Recline and TiltBackrest Mechanism
A. Recliner Back
Power recliner
Advantages:
Independent pressure relief
Can assist in orthostatic episodes
Allows for passive ROM of hip and knee
Makes it easier to perform catheterization
Can help mobilize secretions
Disadvantages:
May result in shear forces
Can increase spasticity
Increased turning radius
27.
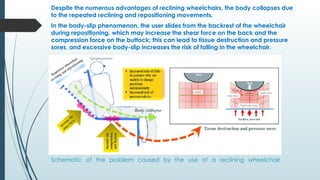
Schematic of theproblem caused by the use of a reclining wheelchair
Despite the numerous advantages of reclining wheelchairs, the body collapses due
to the repeated reclining and repositioning movements.
In the body-slip phenomenon, the user slides from the backrest of the wheelchair
during repositioning, which may increase the shear force on the back and the
compression force on the buttock; this can lead to tissue destruction and pressure
sores, and excessive body-slip increases the risk of falling in the wheelchair.
28.
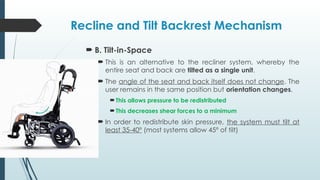
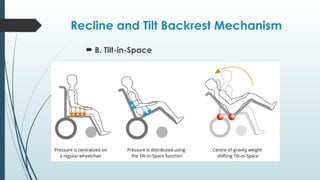
Recline and TiltBackrest Mechanism
B. Tilt-in-Space
This is an alternative to the recliner system, whereby the
entire seat and back are tilted as a single unit.
The angle of the seat and back itself does not change. The
user remains in the same position but orientation changes.
This allows pressure to be redistributed
This decreases shear forces to a minimum
In order to redistribute skin pressure, the system must tilt at
least 35-40º (most systems allow 45º of tilt)
Recline and TiltBackrest Mechanism
B. Tilt-in-Space
TIS Advantages:
Independent pressure relief
Can assist in orthostatic episodes
Alleviates shear
Diminishes effects of spasticity during position changes
Maintains seating position during weight shifts
Helps mobilize secretions
Tighter turning radius
TIS Disadvantages:
No ROM benefits
May not offer as much pressure relief as a recliner
If patient is on CBD, urine may run backwards in the tilted position
Difficult to maintain items on a lap tray when tilted
More difficult to perform catheterization
31.
Wheelchair Armrests
Chairarms may be fixed, swing-away or fully
removable; adjustable or fixed height, full length or
desk arm; and made tubular or standard.
They provide arm support, lateral support, and aid
patients who must elevate their body at regular
intervals to prevent pressure breakdown.
Options:
1. Fixed vs Detachable
Fixed armrests are lighter, but not usually prescribed
secondary to interference with transfers and ADLs. Fixed
armrests do not add width to the chair
Removable armrests are for patients that are close to being
independent with transfers. The width is increased by 2”.
Weight is also increased
32.
Wheelchair Armrests
Options:
2. Full Length vs. Desk Arm
Full length offers more arm support and adjusts with sit to stand
positioning. The disadvantage is that the patient will be unable to
get close to any table
Desk arm allows table access.
3. Adjustable Height Armrests
Adjustable height is available as an alternative to ordering a
fixed custom height
Adjustable armrests are heavier than fixed
4. Tubular vs. Standard Armrests
Tubular arms are more cosmetic, but not suited for heavier
individuals (over 200 pounds)
They are not used when upper extremity weight shifts are
necessary.
33.
Wheelchair Armrests
Variations:
Wraparound armrests are removable and attach behind
the seat. This feature does not increase the width of the
wheelchair.
Swing-away or flip-up armrests are preferred by active SCI
patients.
Younger patients prefer no armrests if balance is not a
concern.
The removable desk arm is the most popular type
prescribed
34.
Wheelchair Wheels
Thestandard chair comes with 2–8” diameter front
caster wheels and 2–24” diameter rear wheels.
However, rear wheels with a diameter of 20–22” are
available.
Mag wheels are most common. They are one piece
and are now cast with metal alloys or metal and
plastic to weigh no more than the wire spoke wheel
and are maintenance-free.
Spoke wheels, similar to a bicycle wheel, are lighter
and easier to propel and improve shock absorption.
However, in the past, they required more maintenance
secondary to bending and loosening.
35.
Wheelchair Wheels
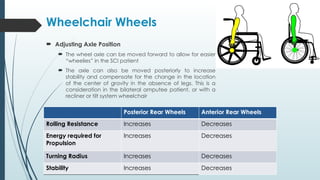
AdjustingAxle Position
The wheel axle can be moved forward to allow for easier
“wheelies” in the SCI patient
The axle can also be moved posteriorly to increase
stability and compensate for the change in the location
of the center of gravity in the absence of legs. This is a
consideration in the bilateral amputee patient, or with a
recliner or tilt system wheelchair
Posterior Rear Wheels Anterior Rear Wheels
Rolling Resistance Increases Decreases
Energy required for
Propulsion
Increases Decreases
Turning Radius Increases Decreases
Stability Increases Decreases
36.
Wheelchair Wheels
Typesof Tires
Solid rubber tires
Very low rolling resistance on flat or smooth surfaces
Flat tires do not occur
Lack “cushioning” on rougher terrain
Heavier than pneumatic tires
Pneumatic tires
Contain air inner tube and are lightweight
Best ride on most surfaces
Provide cushioning for outdoor use to allow a more
comfortable ride and reduce wheelchair wear and tear
Also come with an airless (flat-free) insert that is a soft rubber
or latex gel that replaces the inner tube. The ride is cushioned
and it does not go flat. However, it is slightly heavier than the
basic pneumatic tire
37.
Wheelchair Wheels
Camber
Camber is the wheel angle against the vertical axis
Negative camber makes the wheelchair easier to propel
(especially at higher speeds), increases stability, and
tightens the tuning radius
An angle of 7 degrees maximizes lateral stability
The disadvantages are increased overall width of the
chair up to 6”, increased tire wear, and lower seat height
which may increase wear and tear of the shoulder joint
(NEGATIVE)
38.
Wheelchair Wheels
WheelchairHandrims
Handrims are attached to the driving wheels to
allow propulsion and control safety without
touching the tire directly to avoid soiling the hands
The handrim is also smaller than the wheel making
the chair easier to propel
The larger the diameter of the handrim, the easier it
is to grasp and propel, but it becomes heavier with
increased thickness and requires an increased
number of arm strokes to cover a given distance
The standard handrim is the circular steel tube
However, for individuals who have difficulty with
gripping the smooth surface, vinyl, rubber or plastic
coating is available with optional glove use
There are also vertical, horizontal, or oblique
projections to improve propulsion.
39.
Wheelchair Handrims
Another variation is the one-hand drive chair for
individuals with plexus injury, upper extremity
amputee or hemiplegia
The wheelchair can have interconnected driving
wheels so that both wheels can be controlled from
one side through a dual set of handrims
Mechanism:
When one handrim is moved independently of the
other, only one wheel moves.
When both rims are grasped together, both wheels
are driven simultaneously
Wheelchair Wheels
40.
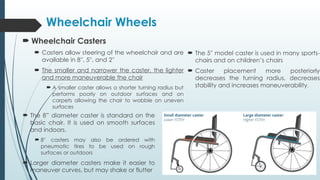
Wheelchair Casters
Casters allow steering of the wheelchair and are
available in 8′′, 5′′, and 2′′
The smaller and narrower the caster, the lighter
and more maneuverable the chair
A smaller caster allows a shorter turning radius but
performs poorly on outdoor surfaces and on
carpets allowing the chair to wobble on uneven
surfaces
Wheelchair Wheels
The 8” diameter caster is standard on the
basic chair. It is used on smooth surfaces
and indoors.
8′′ casters may also be ordered with
pneumatic tires to be used on rough
surfaces or outdoors
Larger diameter casters make it easier to
maneuver curves, but may shake or flutter
The 5′′ model caster is used in many sports-
chairs and on children’s chairs
Caster placement more posteriorly
decreases the turning radius, decreases
stability and increases maneuverability.
41.
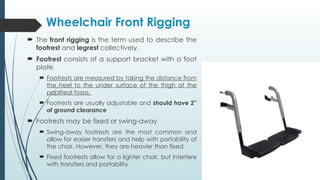
The frontrigging is the term used to describe the
footrest and legrest collectively.
Footrest consists of a support bracket with a foot
plate
Footrests are measured by taking the distance from
the heel to the under surface of the thigh at the
popliteal fossa.
Footrests are usually adjustable and should have 2”
of ground clearance
Footrests may be fixed or swing-away
Swing-away footrests are the most common and
allow for easier transfers and help with portability of
the chair. However, they are heavier than fixed
Fixed footrests allow for a lighter chair, but interfere
with transfers and portability
Wheelchair Front Rigging
42.
Wheelchair Front Rigging
A legrest consists of an elevating support bracket with
swing-away mechanism, a foot plate and a calf pad
to support the back of the leg when elevated
Elevating legrests are essential for patients with:
Gravity-dependent oedema
Transtibial amputations
Knee extension contractures
Other joint abnormalities
A footrest that is excessively long increases pressure
over the lower posterior thigh or hit the floor on uneven
surfaces.
A footrest that is too short increases pressure over the
ischial tuberosities by increasing knee elevation and
shifting the patient within the seat.
43.
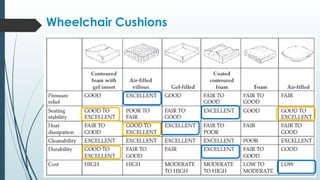
Many differentdesigns of seat cushions are available.
Selection of seat cushions may be divided into 6 basic
types.
All wheelchairs should be used with a seat cushion i.e.
patients should not sit directly on the constructed seat
(sling or rigid) of the wheelchair.
Seating should provide proper pressure relief, enhance
truncal and pelvic stability and provide comfort.
Cushions should be durable and should not retain
perspiration or unacceptable odours.
Wheelchair Cushions
When orderinga wheelchair prescription,
items should also include specific safety
equipment.
Seat belt
Seat belts should be worn for safety
Although the individual patient may be
extremely cautious while seated in the chair,
unforeseen circumstances surrounding the
individual may jar the chair enough to send a
patient out of the chair.
Seat belts are important not only for safety, but
to maintain the pelvis in good position
Wheelchair Safety Equipment
46.
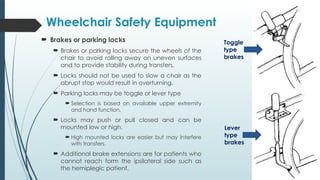
Brakes orparking locks
Brakes or parking locks secure the wheels of the
chair to avoid rolling away on uneven surfaces
and to provide stability during transfers.
Locks should not be used to slow a chair as the
abrupt stop would result in overturning.
Parking locks may be toggle or lever type
Selection is based on available upper extremity
and hand function.
Locks may push or pull closed and can be
mounted low or high.
High mounted locks are easier but may interfere
with transfers.
Additional brake extensions are for patients who
cannot reach form the ipsilateral side such as
the hemiplegic patient.
Wheelchair Safety Equipment
Toggle
type
brakes
Lever
type
brakes
47.
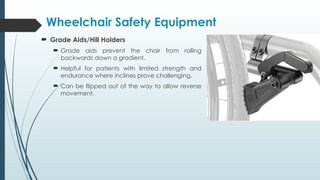
Grade Aids/HillHolders
Grade aids prevent the chair from rolling
backwards down a gradient.
Helpful for patients with limited strength and
endurance where inclines prove challenging.
Can be flipped out of the way to allow reverse
movement.
Wheelchair Safety Equipment
48.
Anti-Tipping Devices
Anti-tipping devices can be fixed or removable
and are extensions placed on the lower rail of
the chair to prevent the chair from falling
backwards.
They are also available for attachment to the
front-rigging to avoid forward tipping.
Anti-tipping devices are mostly used in TF
amputees and in SCI patients.
However, they may interfere with curb
negotiation in patients independent in
community wheelchair mobility.
Wheelchair Safety Equipment
49.
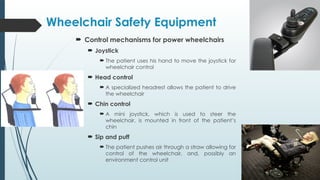
Control mechanismsfor power wheelchairs
Joystick
The patient uses his hand to move the joystick for
wheelchair control
Head control
A specialized headrest allows the patient to drive
the wheelchair
Chin control
A mini joystick, which is used to steer the
wheelchair, is mounted in front of the patient’s
chin
Sip and puff
The patient pushes air through a straw allowing for
control of the wheelchair, and, possibly an
environment control unit
Wheelchair Safety Equipment
50.
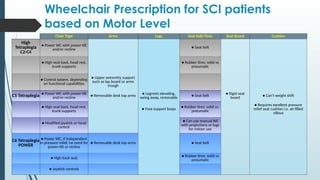
Wheelchair Prescription forSCI patients
based on Motor Level
Chair Type Arms Legs Seat belt/Tires Seat Board Cushion
High
Tetraplegia
C2-C4
● Power WC with power-tilt
and/or recline
● Seat belt
● High seat back, head rest,
trunk supports
● Rubber tires: solid vs
pneumatic
● Control system, depending
on functional capabilities
● Upper extremity support
such as lap board or arms
trough
C5 Tetraplegia ● Power WC with power-tilt
and/or recline ● Removable desk top arms
● Legrests elevating,
swing away, removable ● Seat belt
● Rigid seat
board ● Can't weight shift
● High seat back, head rest,
trunk supports
● Foot support loops ● Rubber tires: solid vs.
pneumatic
● Requires excellent pressure
relief seat cushion i.e. air-filled
villous
● Modified joystick or head
control
● Can use manual WC
with projections or lugs
for indoor use
C6 Tetraplegia
POWER
● Power WC, if independent
in pressure relief, no need for
power-tilt or recline
● Removable desk top arms ● Seat belt
● High back seat
● Rubber tires: solid vs
pneumatic
● Joystick controls
51.
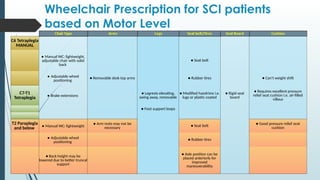
Wheelchair Prescription forSCI patients
based on Motor Level
C6 Tetraplegia
MANUAL
● Manual WC: lightweight,
adjustable chair with solid
back
● Seat belt
● Adjustable wheel
positioning
● Removable desk top arms ● Rubber tires ● Can't weight shift
C7-T1
Tetraplegia ● Brake extensions
● Legrests elevating,
swing away, removable
● Modified handrims i.e.
lugs or plastic coated
● Rigid seat
board
● Requires excellent pressure
relief seat cushion i.e. air-filled
villous
● Foot support loops
T2 Paraplegia
and below ● Manual WC: lightweight
● Arm rests may not be
necessary ● Seat belt
● Good pressure relief seat
cushion
● Adjustable wheel
positioning
● Rubber tires
● Back height may be
lowered due to better truncal
support
● Axle position can be
placed anteriorly for
improved
maneuverability
52.
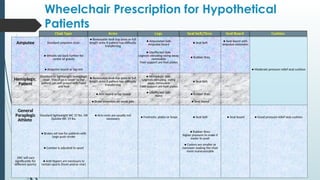
Wheelchair Prescription forHypothetical
Patients
Amputee Standard amputee chair:
● Removable desk top arms or full
length arms if patient has difficulty
transferring
● Amputated Side:
Amputee board ● Seat belt
● Seat board with
amputee extension
● Wheels set back further for
center of gravity
● Unaffected Side:
Legrests elevating swing away,
removable
Foot support are foot plates
● Rubber tires
● Amputee board or leg rest ● Moderate pressure relief seat cushion
Hemiplegic
Patient
Standard or lightweight hemiplegic
chair: This chair is lower so the
patient can self-propel with hand
and foot
● Removable desk top arms or full
length arms if patient has difficulty
transferring
● Hemiplegic Side:
Legrests elevating, swing
away, removable
Foot support are foot plates
● Seat belt
● Arm board or lap board ● Unaffected Side:
None
● Rubber tires
● Brake extension on weak side ● Seat board
General
Paraplegic
Athlete
Standard lightweight WC 37 lbs. OR
Quickie WC 19 lbs.
● Arm rests are usually not
necessary ● Footrests: plates or loops ● Seat belt ● Seat board ● Good pressure relief seat cushion
● Brakes set low for patients with
large push stroke
● Rubber tires:
higher pressure to make it
easier to push
● Camber is adjusted to sport
● Casters are smaller or
narrower making the chair
more maneuverable
(WC will vary
significantly for
different sports)
● Anti-tippers are necessary in
certain sports (front and/or rear)
53.
The basic componentsof wheelchair
prescriptions and measurements have been
covered.
There are many accessories available to assist
with activities of daily living (ADLs) and
everyday functional activities.
Just like a car, wheelchairs can be modified to
meet the aesthetical requirements and needs of
each individual.
CONCLUSION
#9 * Sling upholstery has no capacity to provide pressure relief, and the hammock effect that occurs from wear causes uncomfortable and unstable inward rotation of the hips