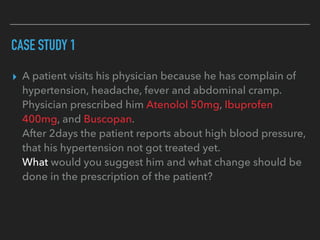
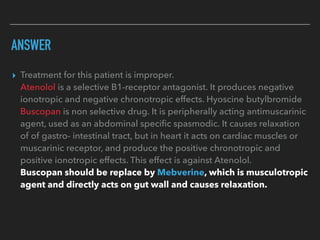
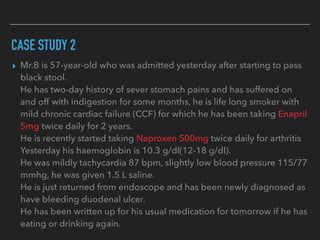
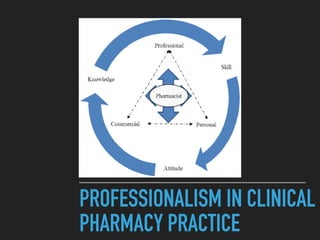
This document discusses clinical pharmacy and provides information on how clinical pharmacists perceive their roles differently than traditional pharmacy roles. It outlines the requirements, goals, and levels of action for clinical pharmacists. Some key roles of clinical pharmacists during inpatient stays include reviewing medication charts, contributing to prescribing decisions, and educating patients. The document also discusses functions of clinical pharmacists like counseling, therapeutic drug monitoring, and adverse drug reaction reporting. It provides examples of clinical pharmacy practice areas and uses case studies to illustrate how clinical pharmacists can assess patients and make therapeutic recommendations.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







