
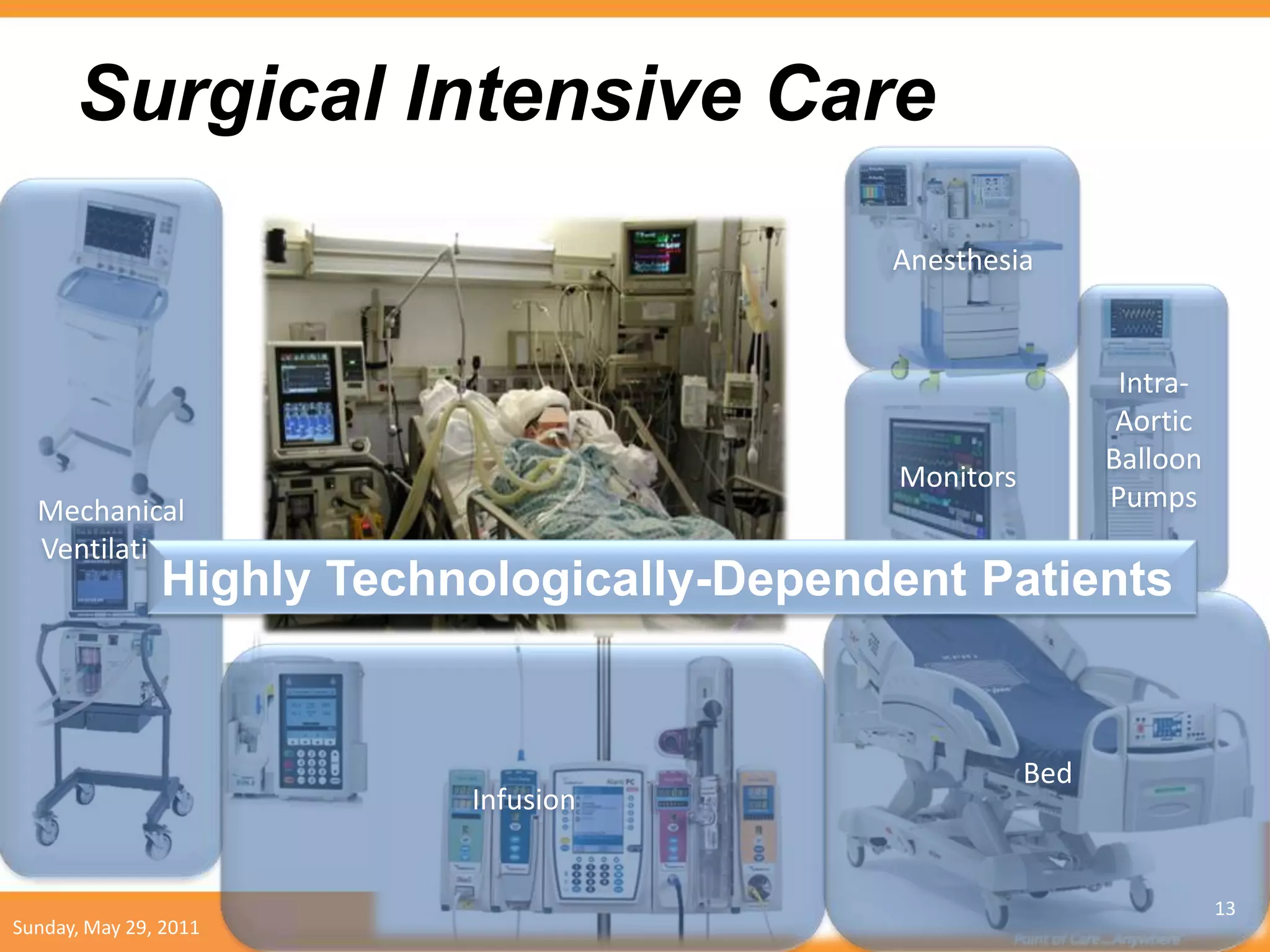
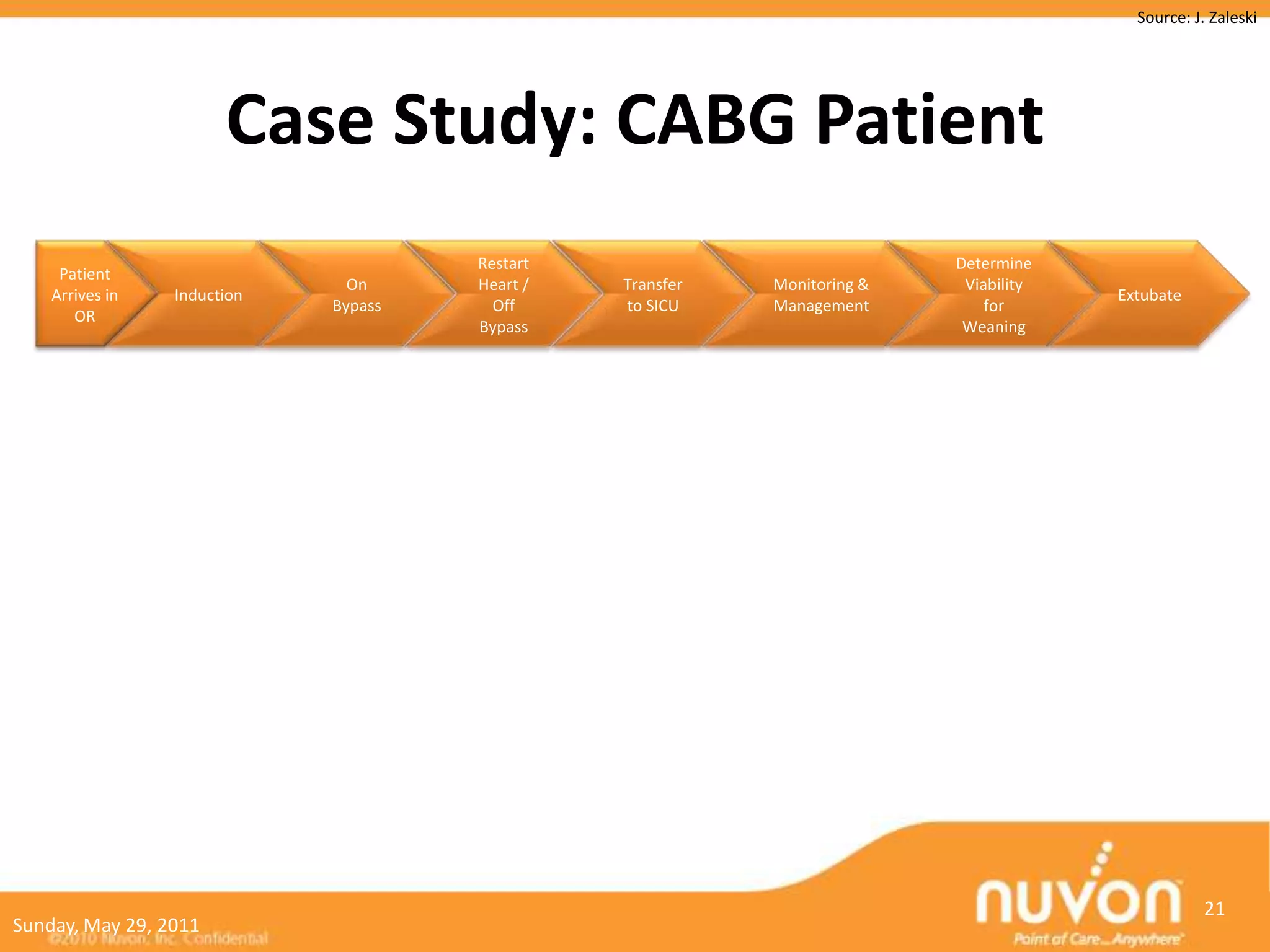
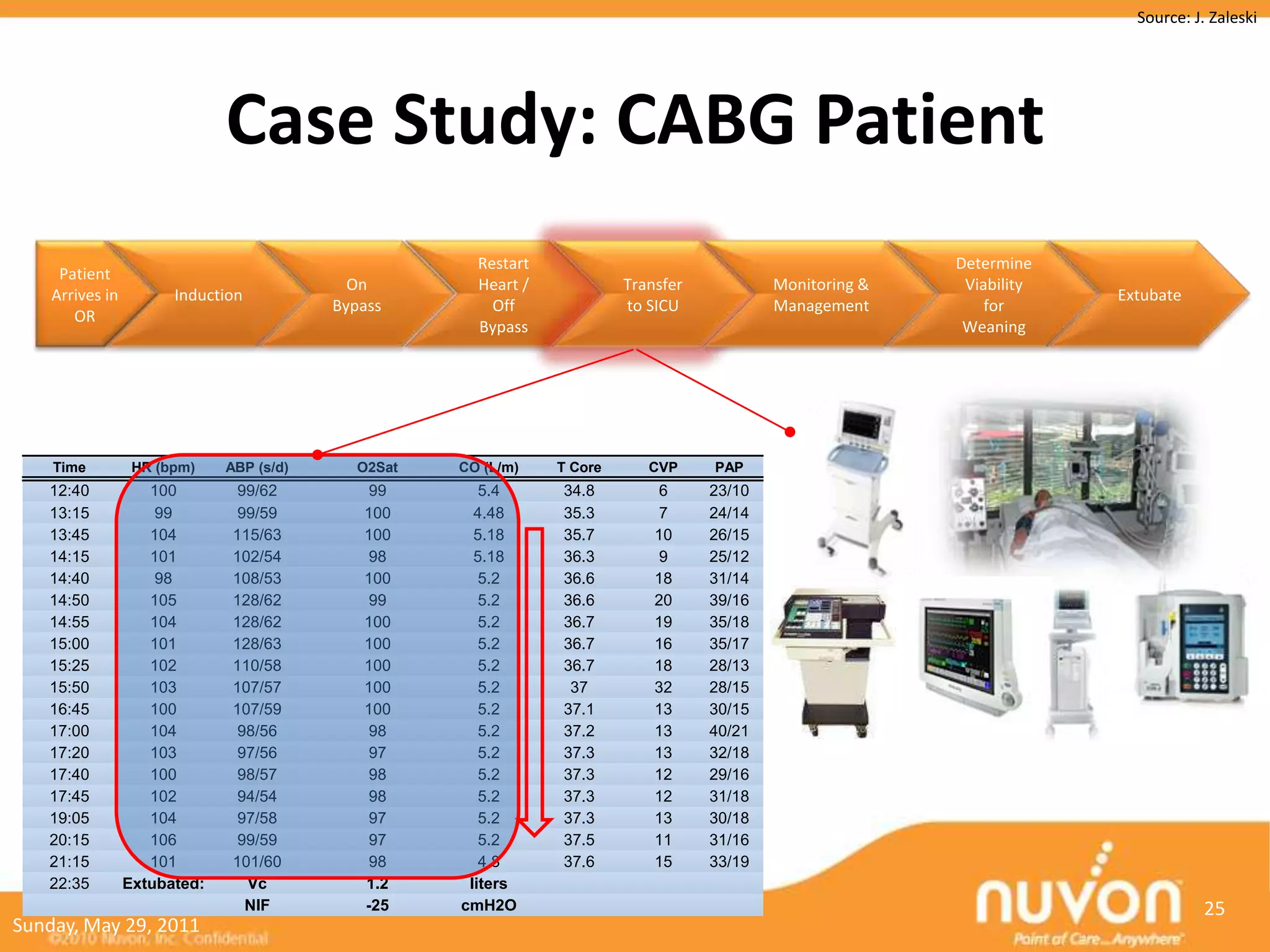
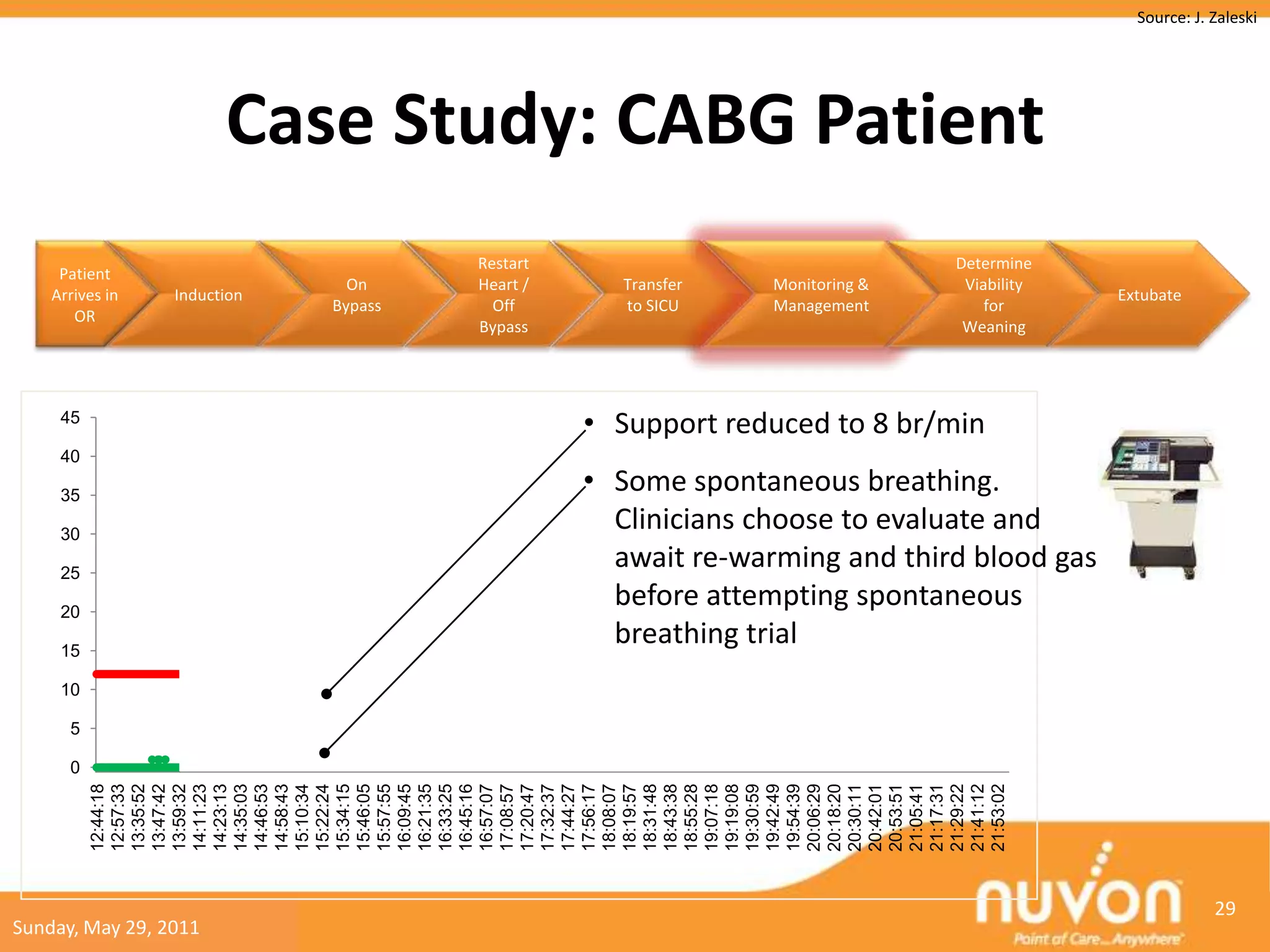
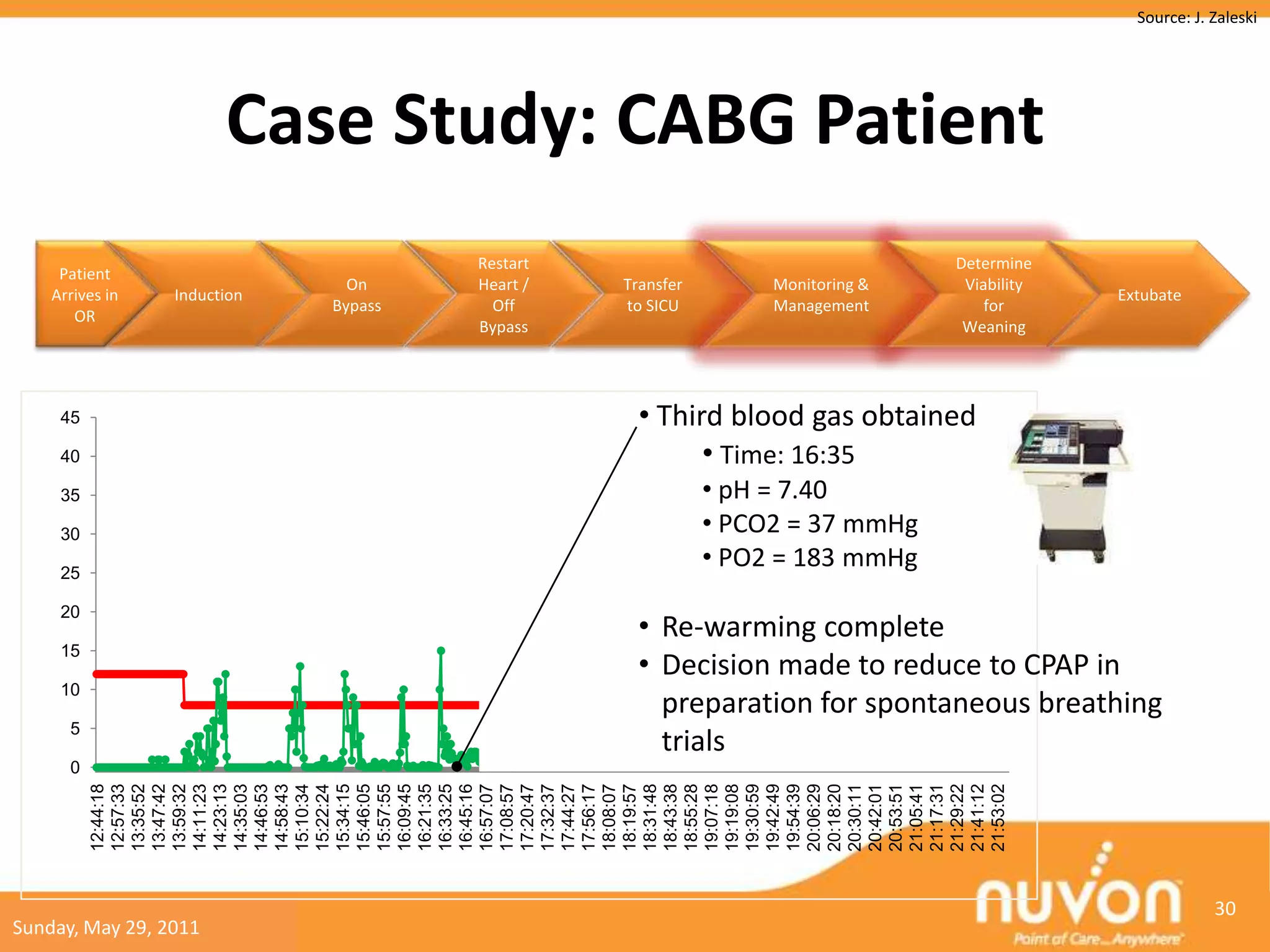
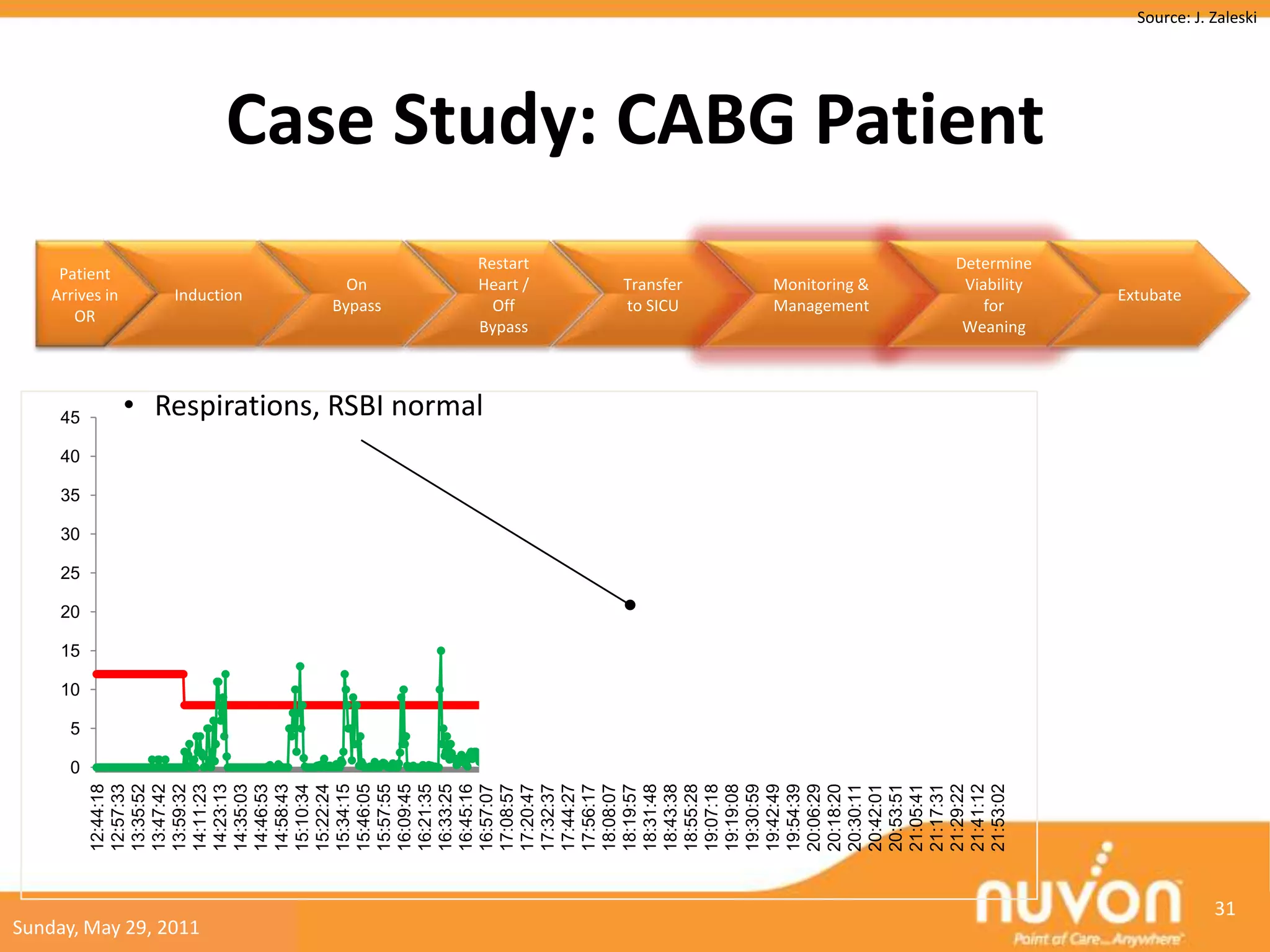
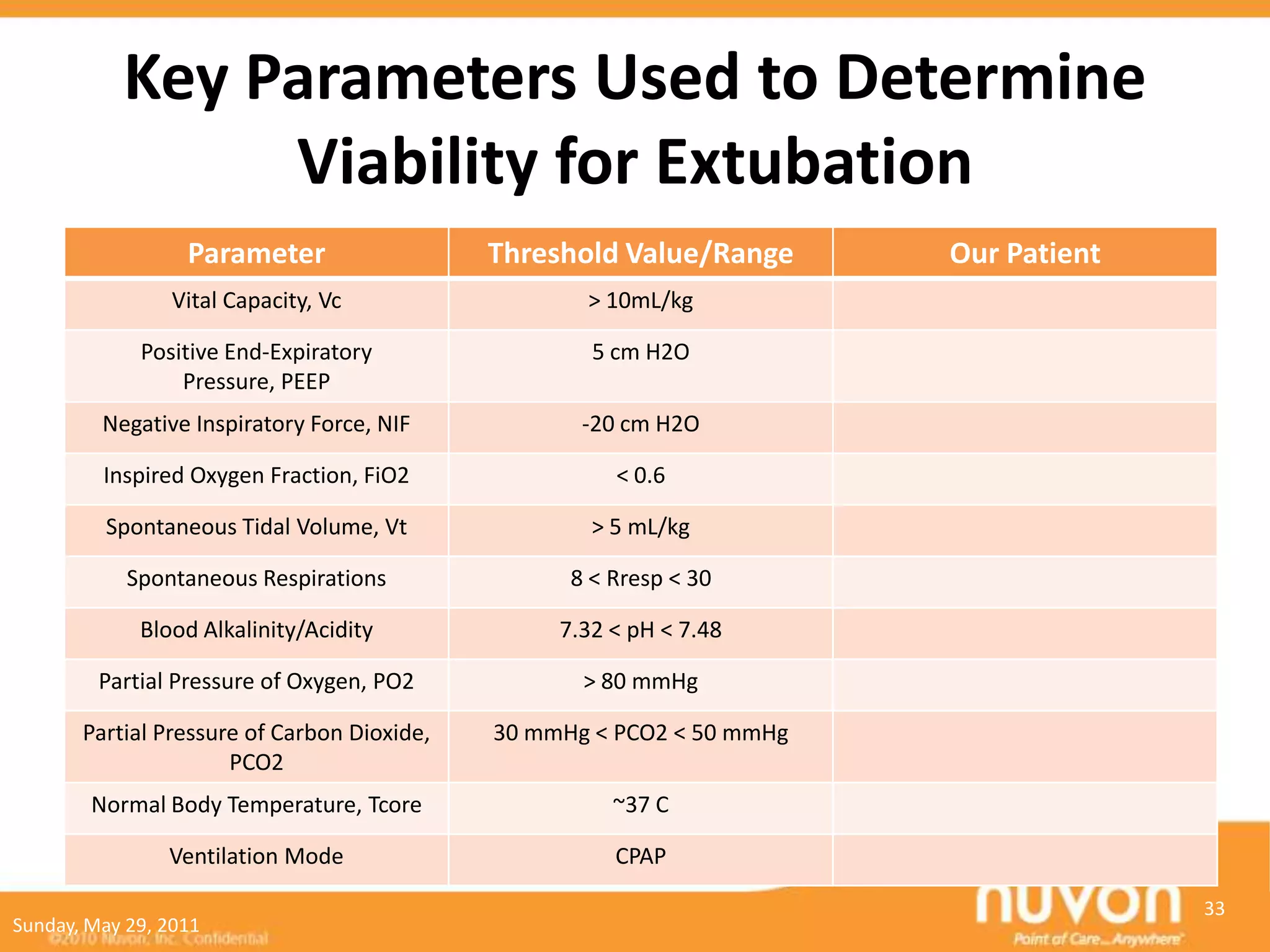
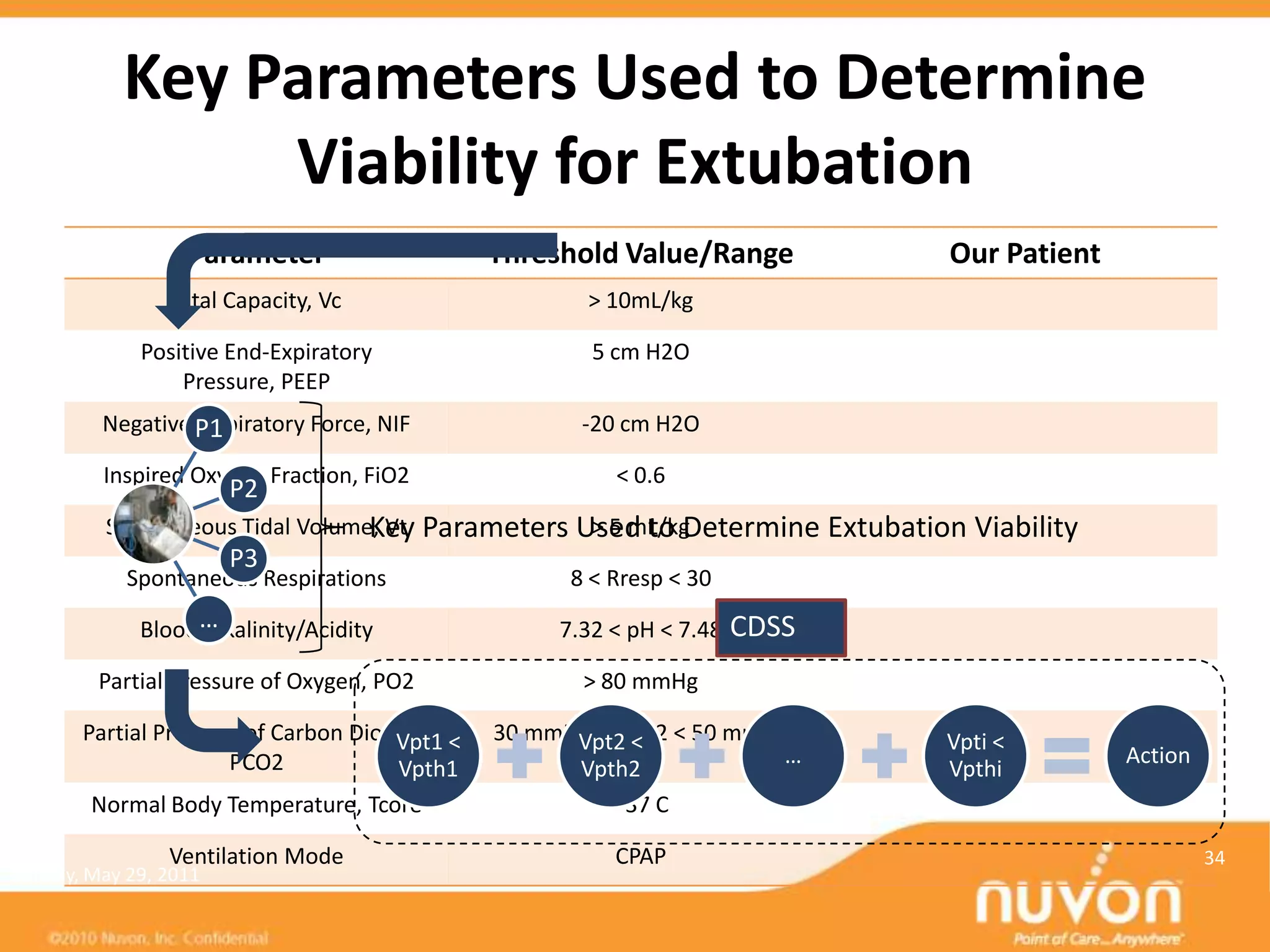
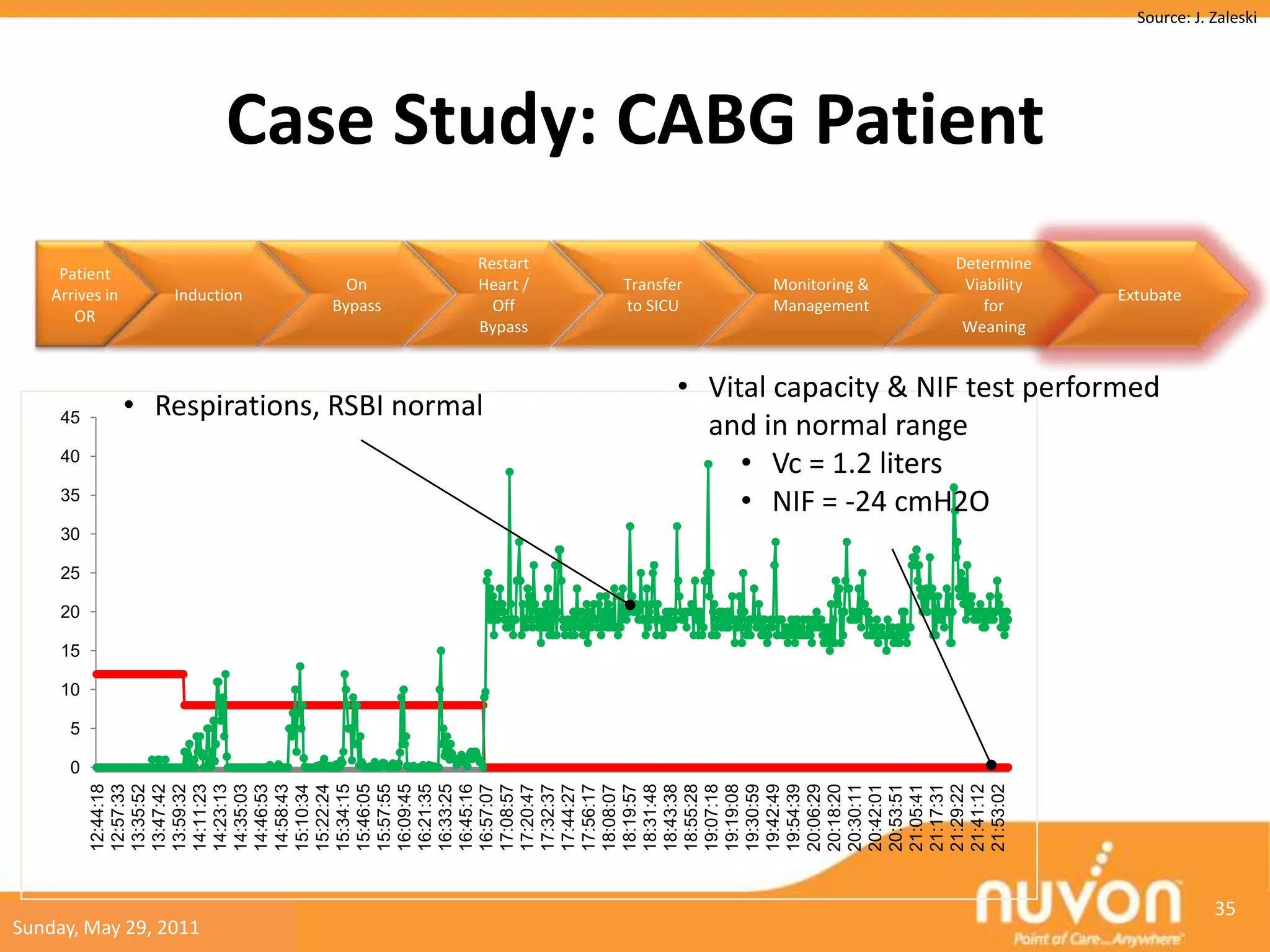
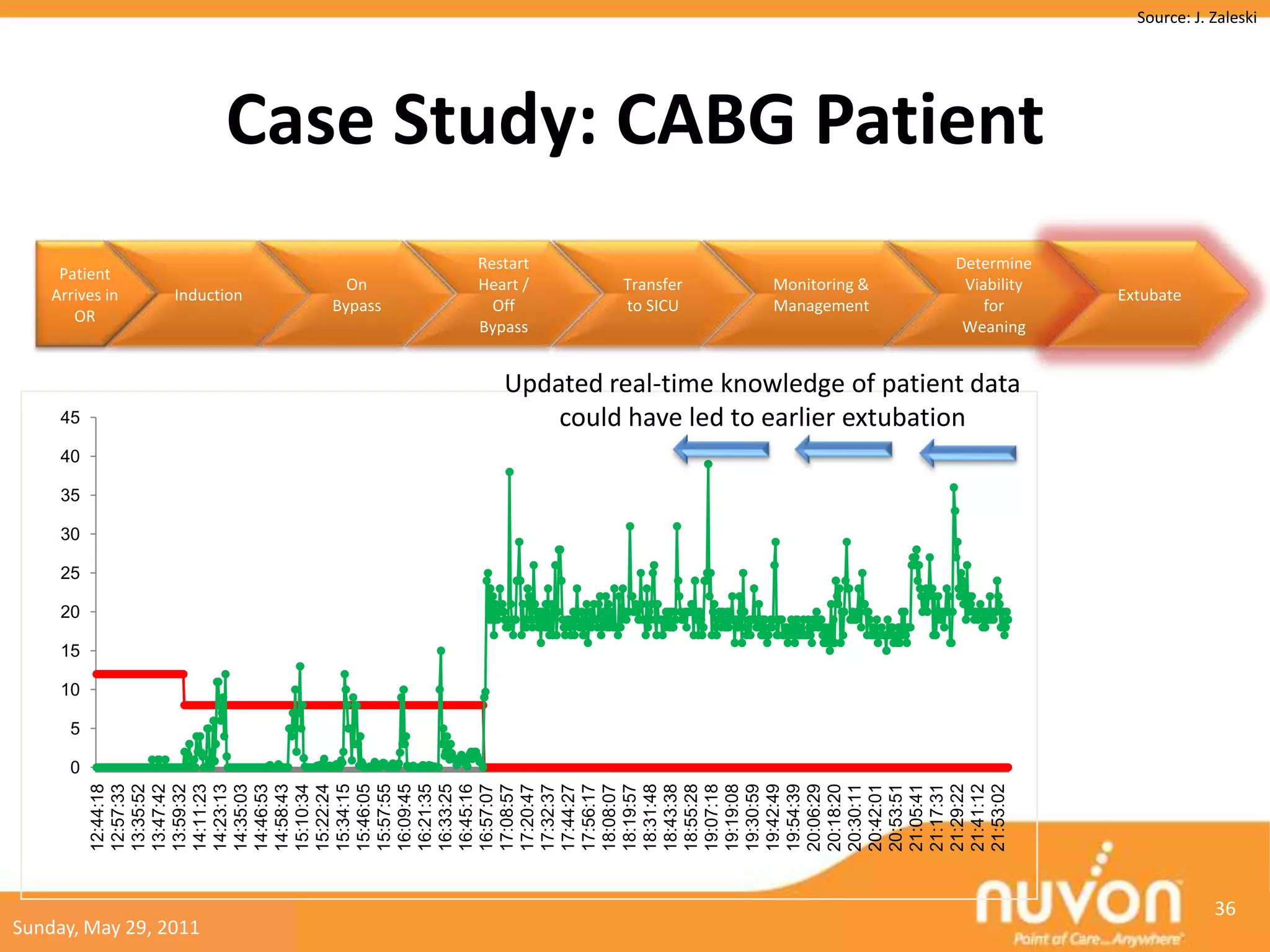
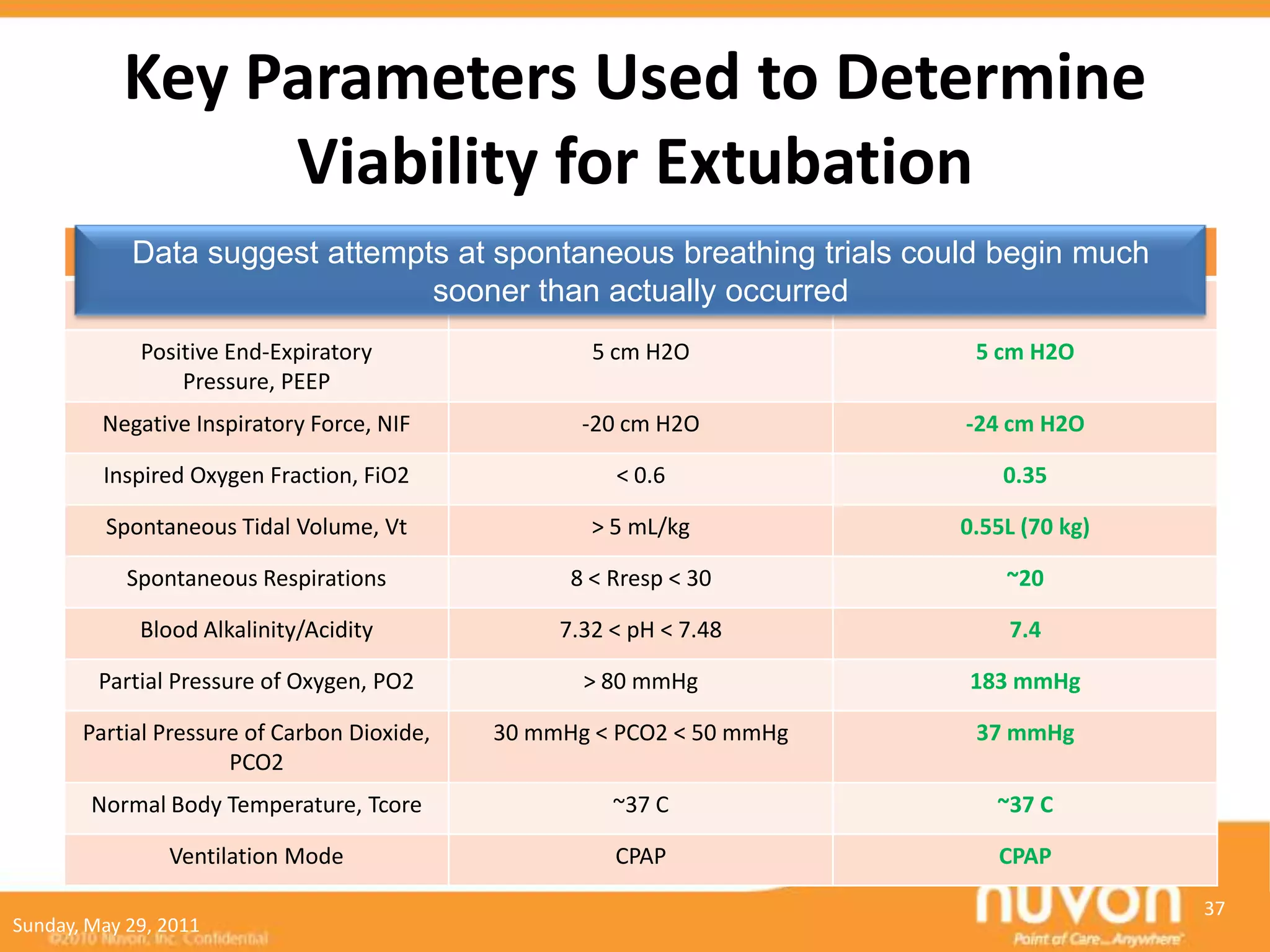

This case study describes a patient undergoing coronary artery bypass grafting (CABG) surgery who is now in the surgical intensive care unit (SICU) post-operatively on mechanical ventilation. Effective clinical decision support could help clinicians: 1. Monitor the patient's vital signs and other parameters to determine when spontaneous breathing trials should begin to assess viability for extubation. 2. Utilize guidelines and best practices for extubation readiness based on the patient's status and progress to safely discontinue mechanical ventilation as quickly as possible to reduce health risks and costs. 3. Provide alerts and recommendations during the weaning process based on continuous monitoring to prevent complications and optimize outcomes.