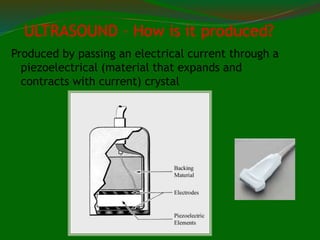
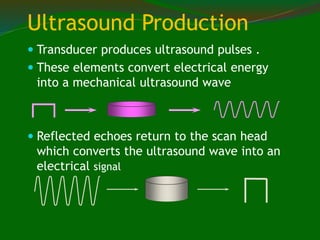
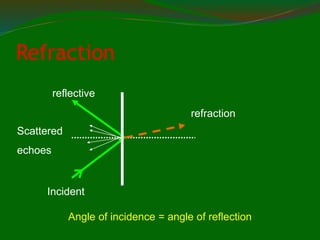
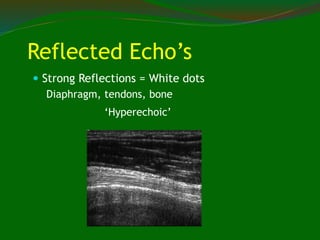
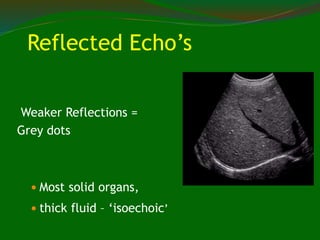
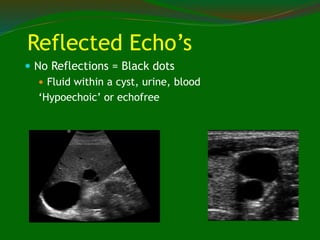
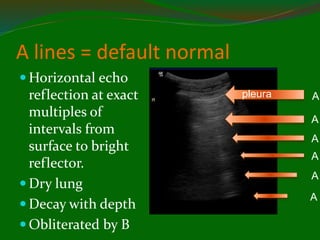
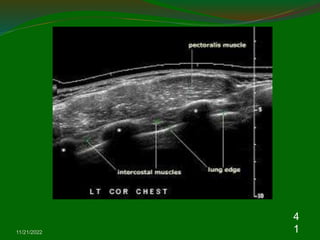
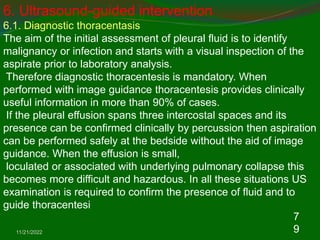
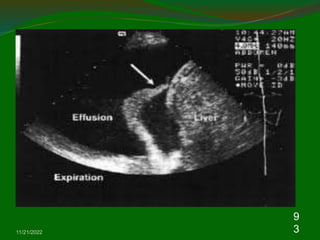
Ultrasound (US) is a cost-effective, portable imaging tool that assists in diagnosing chest diseases, particularly pleural conditions and peripheral pulmonary lesions. It operates by producing mechanical waves that reflect off various tissues, allowing visualization of lung and pleural structures, and thus helping in diagnosing conditions like pleural effusions and pneumothorax. Key techniques for effective use include selecting appropriate transducer frequencies and positioning patients to avoid obstructions from the chest wall.


















![USG THORAX [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/usgthoraxautosaved-220404152154-thumbnail.jpg?width=640&height=640&fit=bounds)
































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












