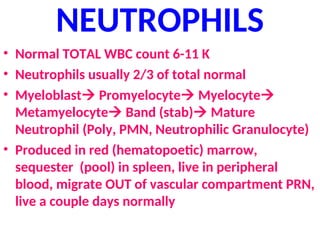
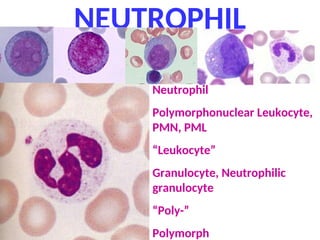
NEUTROPHILS
• Normal TOTALWBC count 6-11 K
• Neutrophils usually 2/3 of total normal
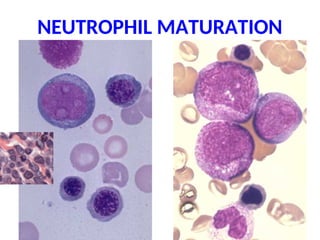
• Myeloblast Promyelocyte Myelocyte
Metamyelocyte Band (stab) Mature
Neutrophil (Poly, PMN, Neutrophilic Granulocyte)
• Produced in red (hematopoetic) marrow,
sequester (pool) in spleen, live in peripheral
blood, migrate OUT of vascular compartment PRN,
live a couple days normally
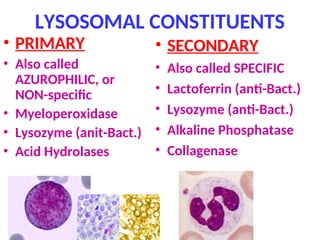
LYSOSOMAL CONSTITUENTS
• PRIMARY
•Also called
AZUROPHILIC, or
NON-specific
• Myeloperoxidase
• Lysozyme (anit-Bact.)
• Acid Hydrolases
• SECONDARY
• Also called SPECIFIC
• Lactoferrin (anti-Bact.)
• Lysozyme (anti-Bact.)
• Alkaline Phosphatase
• Collagenase
9.
FUNCTIONS
• Margination
• Rolling
•Adhesion
• Transmigration (Diapedesis)
• Chemotaxis
• Phagocytosis:
RecognitionEngulfmentKilling (digestion)
• Equilibrium with splenic pool
10.
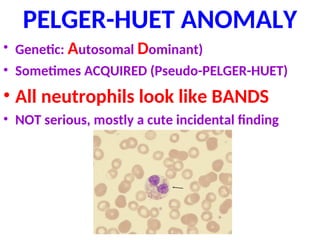
PELGER-HUET ANOMALY
• Genetic:Autosomal Dominant)
• Sometimes ACQUIRED (Pseudo-PELGER-HUET)
• All neutrophils look like BANDS
• NOT serious, mostly a cute incidental finding
11.
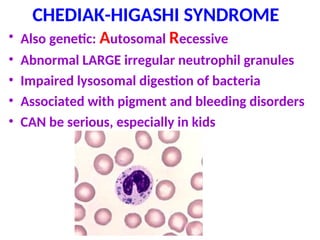
CHEDIAK-HIGASHI SYNDROME
• Alsogenetic: Autosomal Recessive
• Abnormal LARGE irregular neutrophil granules
• Impaired lysosomal digestion of bacteria
• Associated with pigment and bleeding disorders
• CAN be serious, especially in kids
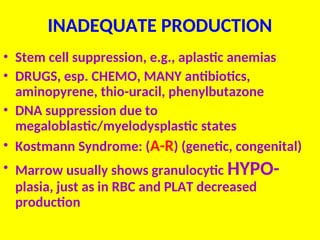
INADEQUATE PRODUCTION
• Stemcell suppression, e.g., aplastic anemias
• DRUGS, esp. CHEMO, MANY antibiotics,
aminopyrene, thio-uracil, phenylbutazone
• DNA suppression due to
megaloblastic/myelodysplastic states
• Kostmann Syndrome: (A-R) (genetic, congenital)
• Marrow usually shows granulocytic HYPO-
plasia, just as in RBC and PLAT decreased
production
14.
INCREASED DESTRUCTION
• Immunemediated
–By itself (idiopathic), or as in SLE
–After “sensitization” by many drugs
• Splenic sequestration, hypersplenism
• Increased peripheral demand, as in
overwhelming infections, esp. fungal
• Marrow usually shows granulocytic
HYPER-plasia, just as in RBC and PLAT
increased destructions
15.
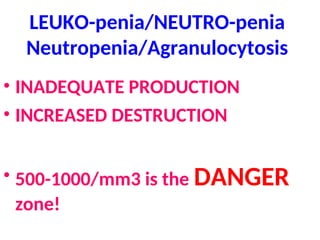
Leukocytosis/Neutrophilia
• Marrow andsplenic pool size
• Rate of release between pool and circulation
• Marginating pool
• Rate of WBCs (neutrophils/monocytes) leaving the
vascular compartment
• NON-vascular pools FIFTY times larger than the
vascular pools
• TNF/IL-1/cytokines stimulate T-cells to produce
CSF, the WBC equivalent of EPO
16.
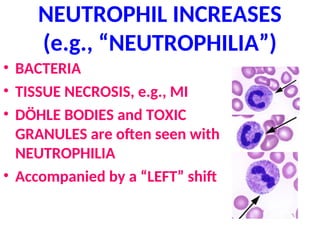
NEUTROPHIL INCREASES
(e.g., “NEUTROPHILIA”)
•BACTERIA
• TISSUE NECROSIS, e.g., MI
• DÖHLE BODIES and TOXIC
GRANULES are often seen with
NEUTROPHILIA
• Accompanied by a “LEFT” shift
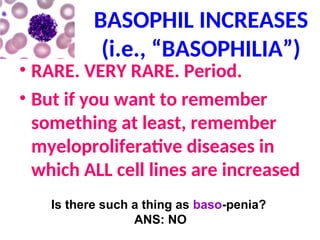
BASOPHIL INCREASES
(i.e., “BASOPHILIA”)
•RARE. VERY RARE. Period.
• But if you want to remember
something at least, remember
myeloproliferative diseases in
which ALL cell lines are increased
Is there such a thing as baso-penia?
ANS: NO
“MYELOPROLIFERATIVE”
disorders
• Also called“chronic” myeloproliferative disorders because
they last for years
• Differentiate: Myeloproliferative vs. Myelodysplastic
• ALL marrow cell lines are affected, splenomegaly
• Proliferating cells do NOT suppress residual marrow
production, and go OUTSIDE marrow, and EXPAND
marrow to fatty appendicular marrow
• Associated with EXTRA-medullary hematopoesis
– Chronic Myelogenous “Leukemia” (CML)
– P. Vera
– Essential Thrombasthenia (aka, Essential Thrombocytosis)
– Myelofibrosis
22.
CML
• NOT ATALL like an “acute” leukemia, but can
develop into an acute leukemia, as a condition
called a “blast crisis”
• Age: adult, NOT kids
• 90% have the “Philadelphia” chromosome, which
are aberrations on chromosome #9 (BCR) and #22
(ABL), the BCR-ABL “fusion”
23.
CML
• Marrow 100%cellular, NOT 50%
• ALL cell lines increased, M:E ratio massively
increased, 50K-100K neutrophils with
SIGNIFICANT “left shift”, but not more
than 10% blasts
• SIGNIFICANT SPLENOMEGALY!!!!!
• Significant breakthrough with BCR-ABL kinase
inhibitors!!! (90% remissions)
26.
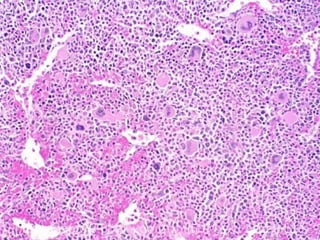
Polycythemia Vera
• Allcell lines increased, NOT just RBC
• HIGH marrow cell turnover stimulates
increased purines which often cause gout
(10%)
• BOTH thrombosis AND bleeding risks are
present because the increased platelets are
AB-normal
• Do not get “blast” crises, BUT can progress to
myelofibrosis
28.
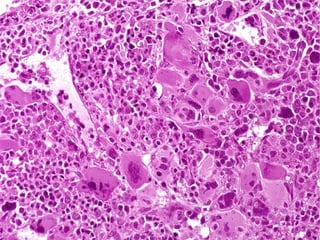
ESSENTIAL THROMOCYTOSIS
(THROMBASTHENIA)
• Plateletcount often near 1 million/mm3
• Often a diagnosis of exclusion.
• The RAREST of all myeloproliferative
disorders
• Giant platelets usually. Why? Ans: Quicker
release from marrow (RPW/RDW)
(MPV/MCV)
• Massively increased megakaryocytes in the
marrow
30.
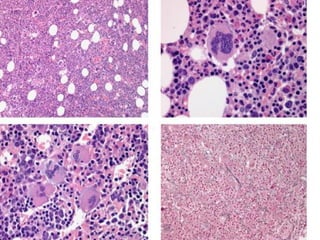
PRIMARY MYELOFIBROSIS
• Rapidprogressive marrow fibrosis
• Oldest age group of all the MPD’s, >60
• Can follow other MPD’s. Why?
• Usually the most extensive extramedullary
hematopoesis because the marrow is NOT
the primary site of hematopoesis
• LEUKOERYTHROBLASTOSIS
• Like CML, 10-20% can progress to AML
LEUKEMIAS
• DEF:MALIGNANT PROLIFERATIONSof
WHITE BLOOD CALLS
• In the case of myeloid precursors, the
primary process is marrow and peripheral
blood, but can involve any organ or tissue
which receives blood
• In the case of lymphocytes, there is an
intimate concurrence with malignant
lymphomas
34.
Leukemias vs. Lymphomas
•All leukemias of lymphocytes have lymphoma
counterparts
• Primary lymphomas can have “leukemic” phases, and
involve marrow, especially multiple myelomas
• Any myeloid leukemia can infiltrate a lymph node, or any
other site, but if/when it does it is NOT called a
lymphoma, but simply a myeloid infiltrate INTO a lymph
node
• ALL lymphomas are malignant proliferations of
lymphocytes, and usually start in lymph nodes but can
originate ANYWHERE there are lymphocytes!
• ALL leukemias involve bone marrow changes
35.
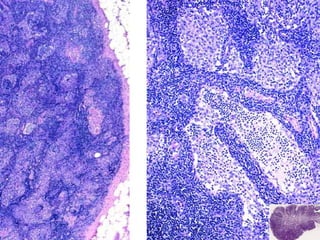
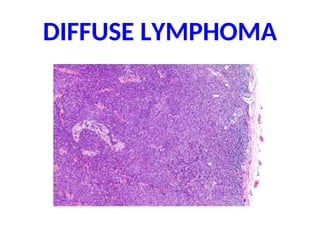
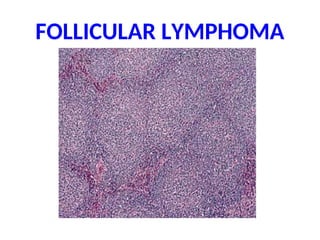
LYMPHOMAS
• NODAL orEXTRANODAL
• T or B
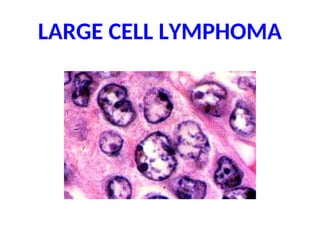
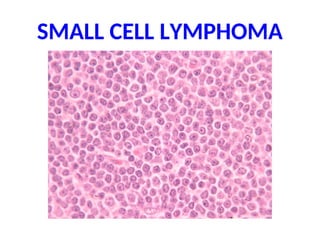
• SMALL or LARGE CELLS
• FOLLICULAR or DIFFUSE
• Hodgkins or NON-Hodgkins
• “F.A.B. classification” is currently popular
this week (FrenchAmericaBritish), for the
NON-Hodgkins lymphomas, also evolved into
the “International” classification
36.
LEUKEMIAS
• Acute (blasts)or Chronic (few or NO blasts)
• Myeloid (0-7) A/C or Lymphocytic A/C
• Childhood or Adult
• All involve marrow
• All ACUTE leukemias suppress normal
hematopoesis, i.e., have anemia, thrombocytopenia,
these are usually the presenting symptoms!
• Most have chromosomal aberrations
• Some can respond DRASTICALLY to chemo, most
notably ALL in children, even be cured (ALL) !!!!
37.
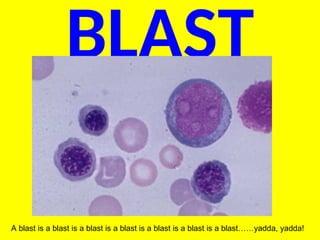
BLAST
A blast isa blast is a blast is a blast is a blast is a blast is a blast……yadda, yadda!
38.
WHITE CELL NEOPLASMSLeuk/Lymph, I
(Hematologic Malignancies)
• Many have chromosomal translocations,
predictable and characteristic, but not 100% of
the time
• Can arise in inherited and/or genetic diseases:
– Downs Syndrome (Trisomy 21)
– Fanconi’s anemia (hereditary aplastic anemia)
– Ataxia telangiectasia
• May have a STRONG viral relationship:
– HTLV-1 (lymphoid tumors)
– EBV (Burkitt Lymphoma)
– Human Herpesvirus-8 (B-Cell Lymphomas) (also KS)
39.
WHITE CELL NEOPLASMSLeuk/Lymph, II
• Can be caused by H. Pylori (gastric B-Cell
lymphomas)
• Can follow celiac disease (gluten
sensitive enteropathy T-Cell
lymphomas)
• Are common in HIV, B-Cell lymphomas,
CNS lymphomas
40.
A.L.L./LYMPHOMAS*
• SUDDEN ONSET
•ANEMIA, BLEEDING, FEVER
• Bone pain, adenopathy, hepatosplenomegaly
• CNS: headaches, vomiting, nerve palsies
• (*NB: These are pretty much the clinical symptoms of A.M.L. too and vice versa)
41.
A.L.L./LYMPHOMAS
• “Lymphoblasts” whichcan give rise either to T or B cells
are the cells of malignant proliferation
• All lymphocytic leukemias CANNOT be classified
independently of lymphomas because they all have
lymphoma counterparts
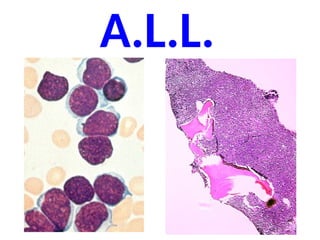
• A.L.L. mostly in children
• Most have chromosomal changes, hyperploidy,
Philadelphia chromosome, translocations
• SIGNIFICANT response to chemo: 90% remission, 75%
CURE!!!
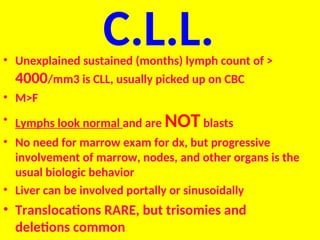
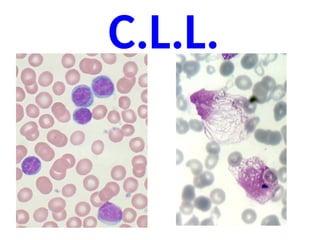
C.L.L.
• Unexplained sustained(months) lymph count of >
4000/mm3 is CLL, usually picked up on CBC
• M>F
• Lymphs look normal and are NOTblasts
• No need for marrow exam for dx, but progressive
involvement of marrow, nodes, and other organs is the
usual biologic behavior
• Liver can be involved portally or sinusoidally
• Translocations RARE, but trisomies and
deletions common
MULTIPLE MYELOMA
• DEFINEDAS A MALIGNANT PROLIFERATION OF
PLASMA CELLS (i.e., former B-lymphocytes)
• Can have a “leukemic” phase, but the BONE
MARROW is the usual primary site of origin
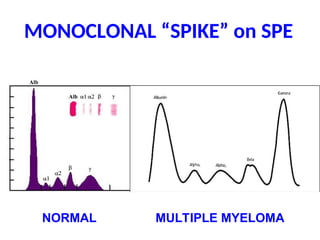
• Usually have MONOCLONAL GAMMOPATHIES
• Secrete Heavy and Light chains, and Light chains
in the urine is known as Bence-Jones protein
• Usually have elevated IL-6 (bad prognosis)
47.
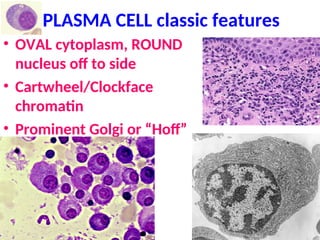
PLASMA CELL classicfeatures
• OVAL cytoplasm, ROUND
nucleus off to side
• Cartwheel/Clockface
chromatin
• Prominent Golgi or “Hoff”
MULTIPLE MYELOMA
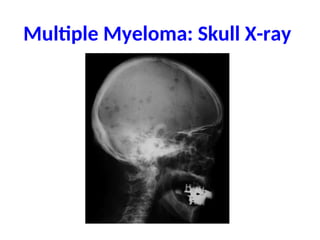
• BONEDESTRUCTION
• Various deletions and translocations
• Plasma cells usually 1-3% of marrow, but >20% or plasma
cells in SHEETS is diagnostic
• Plasma cells usually look normal
• IgG >> IgA, other immunoglobulins are rare
• Staph, Strep, E. coli infections
• Bleeding*
• Amyloidosis
• RENAL FAILURE
M.G.U.S.
• Monoclonal Gammopathyof Unknown
Significance, i.e., no plasma cell
proliferation is found
• Age related
• 1% of 50-year olds, 3% of 70-year olds, etc.
• Same chromosomal aberrations as MM, but
generally follow a BENIGN course
53.
Other “GAMMOPATHIES”
• Waldenstrom’sMACRO-globulinemia
IgM (associated with lymphomas)
• Heavy Chain Disease (associated with
lymphomas)
•AMYLOID, follows MM and/or chronic
granulomatous diseases
54.
A.M.L.
• GENETIC ABERRATIONSINHIBIT DIFFERENTIATION
• Many have various TRANSLOCATIONS
• F.A.B. classifies them as M0 M7
• MORE than 20% of BLASTS are needed in the
marrow for a diagnosis of acute leukemia!!! (i.e.,
ANY kind of BLAST
• NORMALLY, a marrow should have only about 1-2
% blasts
55.
A.M.L.
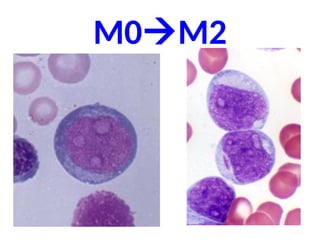
• M0 Minimallydifferentiated
• M1 AUER rods rare (COMMON)
• M2 AUER rods common (COMMON)
• M3 Acute PRO-myelocytic leukemia (Azurophilic, primary
nonspecific granules)
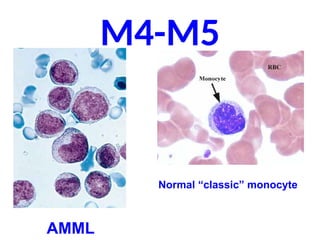
• M4 AMML (myelo-Mono cytic) (COMMON)
• M5 Monocytic
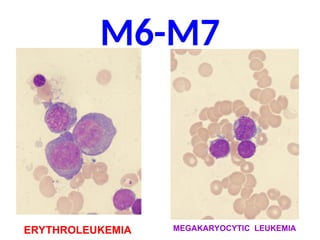
• M6 ErythroLeukemia
• M7 Acute Megakaryocytic leukemia
NOTE: Diagnosis is CONFIRMED by special markers, not just
visual identification
A.M.L.
• Anemia
• Thrombocytopenia(bleeding)
– Petechiae
– Ecchymoses
• Fever
• Fatigue
• Lymphadenopathy
• 60% respond, BUT only 20 % are free of remission
after 5 years, WORSE than A.L.L.
61.
MYELO-DYSPLASTIC SYNDROMES
• Increasedrisk of acute leukemias
• But, UNLIKE the myeloPROLIFERATIVE syndromes, NOT
a hypercellular marrow
• Spontaneous or drug (chemo) related (even > 5 yrs!)
• Has marrow ABERRATIONS
– REFRACTORY ANEMIAS
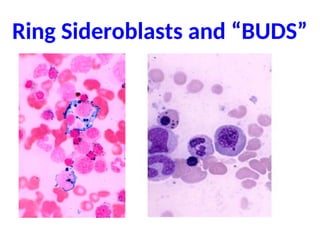
– RINGED SIDEROBLASTS (Fe in mitochondria)
– Nuclear “BUDDING”
– EXCESS BLASTS, but LESS than 20%
– About, say, 25% develop into acute leukemias
Definition of TERMS
•Lymphadenopathy
• Lymphadenitis
• Dermatopathic
• Normal size?
• Palpation
• What to do if a lymph node is enlarged?
• Diffuse/Follicular
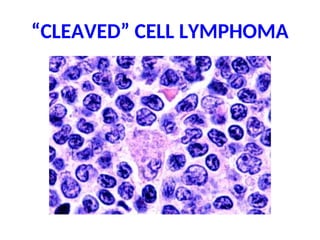
• T/B/NK, Small/Large, Cleaved/Non-cleaved
• Precursor/Peripheral
• HD/Non-HD
67.
BENIGN ENLARGEMENT
• Alsocalled LYMPHADENITIS, and HYPERPLASIA
• Can be ACUTE (tender), or CHRONIC (non-tender)
• Usually SUBSIDE in, say, less than 6 weeks
• FOLLICULAR HYPERPLASIA is enlargement of the cortical
secondary follicles and increase in number of the cortical
secondary follicles
• SINUS HISTIOCYTOSIS is prominence in medullary sinuses
(also called “reticular” hyperplasia)
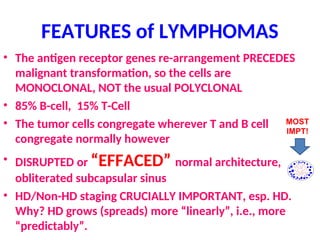
FEATURES of LYMPHOMAS
•The antigen receptor genes re-arrangement PRECEDES
malignant transformation, so the cells are
MONOCLONAL, NOT the usual POLYCLONAL
• 85% B-cell, 15% T-Cell
• The tumor cells congregate wherever T and B cell
congregate normally however
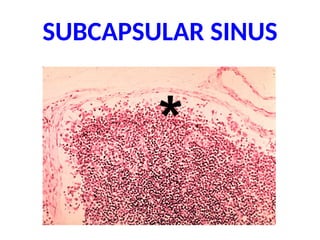
• DISRUPTED or “EFFACED” normal architecture,
obliterated subcapsular sinus
• HD/Non-HD staging CRUCIALLY IMPORTANT, esp. HD.
Why? HD grows (spreads) more “linearly”, i.e., more
“predictably”.
MOST
IMPT!
STAGING, HD &NHD
• I ONE NODE or NODE GROUP
• II MORE than ONE, but on ONE side of diaph.
• III BOTH sides of diaph., but still in nodes only
• IV OUTSIDE of NODES, e.g., liver, marrow, etc.
• A No systemic symptoms
• B fever and/or night sweats and/or 10% weight loss
87.
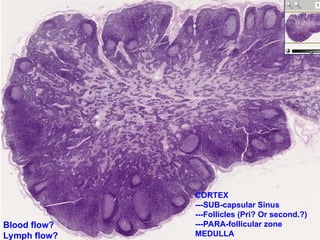
METASTATIC CARCINOMA
• Perhapsthe single most important staging and
prognostic feature of tumors
• The metastatic cells FIRST enter into the
SUBCAPSULAR SINUS
• The tumor may replace the entire node and
enlarge it
• The tumor may be focal
• The tumor usually looks the same as it’s primary
or other metastases
• The tumor usually ENLARGES the node, eventually
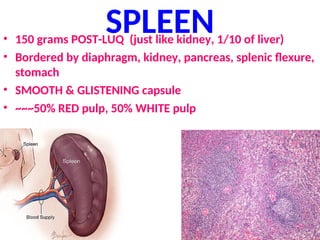
SPLENIC FUNCTION
• REMOVEOLD BLOOD CELLS
• MAJOR SECONDARY ORGAN of the IMMUNE
SYSTEM
• HEMATOPOIESIS
• SEQUESTER (POOL) BLOOD CELLS
• 15% of body’s PHAGOCYTIC activity is in the
spleen (liver has >80)
PRIMARY TUMORS (RARE)
•HEMANGIOMA
• LYMPHANGIOMA
• fibroma
• osteoma
• chondroma
•LYMPHOMA
Not surprising, because there are NO
epithelial cells native to the spleen!
100.
MISC
• Congenital Absence(very rare)
• “Accessory” spleens (very very
common, especially with
splenomegaly!)
•RUPTURE
101.
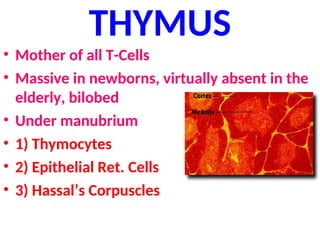
THYMUS
• Mother ofall T-Cells
• Massive in newborns, virtually absent in the
elderly, bilobed
• Under manubrium
• 1) Thymocytes
• 2) Epithelial Ret. Cells
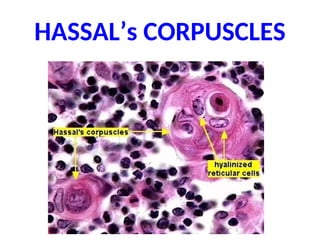
• 3) Hassal’s Corpuscles
DISEASES
•HYPOPLASIA/APLASIA
– DiGeorge Syndrome(i.e., velocardiofacial, 22q11.2 deletion)
•CYSTS (incidental)
•THYMOMAS
• Oldage atrophy (involution) is so common,
you can hardly call it a disease
104.
THYMOMAS
• ALL (most)thymomas show counterparts of
BOTH lymphoid as well as epithelial reticular
cells, hence, the classic name
“LYMPHOEPITHELIOMA”
–Benign thymoma: (encapsulated)
–Malignant Thymoma I: (locally invasive)
–Malignant Thymoma II: (easily metastasizable)
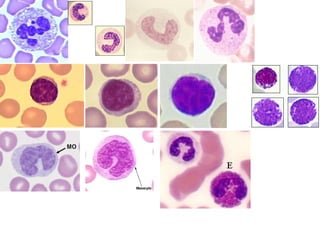
#7 ALL blasts look the same on routine stains, whether they are myeloblasts, lymphoblasts, monoblasts, etc.
A blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast is a blast!
Please remember you have all been conditioned to think a NUCLEOLUS is darker than the rest of the NUCLEUS, as it is on H&E, but in the usual stains we stain bone marrow smears or peripheral smears with, i.e., Wright or Giemsa respectively, the nucleoli are LIGHTER!!!
#8 MYELOPEROXIDASE stains are often use to identify cells believed to be of MYELOID origin, such as blastic looking cells, because you cannot really tell for sure on Wright’s or Giemsa stains.
Are these substances part on innate or learned immunity? ANS: INNATE
#12 Notice the parallel with anemia and thrombocytopenia.
#16 TOXIC GRANULES are EXAGGERATIONS of the marrow’s normal granularity, DOHLE bodies are fragments of remaining dilated rough ER.
Neutrophilia can be viewed as a NONSPECIFIC index of acute infection, especially bacterial, but also tissue necrosis. The causes of NEUTROPHILIA can be said to be as the same causes of ACUTE INFLAMMATION!
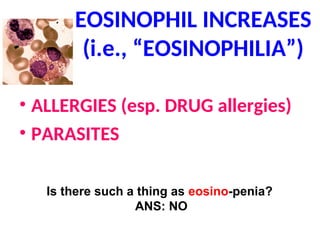
#17 Following activation by an immune stimulus, eosinophils degranulate to release an array of cytotoxic granule cationic proteins that are capable of inducing tissue damage and dysfunction. These include:
1) major basic protein (MBP)
2) eosinophil cationic protein (ECP)
3) eosinophil peroxidase (EPO)
4) eosinophil-derived neurotoxin (EDN)
#18 Not only are basophils RARE to find normally, but pure “basophilia” is also VERY rare.
When activated, basophils degranulate to release histamine, proteoglycans (e.g. heparin and chondroitin), and proteolytic enzymes (e.g. elastase and lysophospholipase). They also secrete lipid mediators like leukotrienes, and several cytokines
#19 Why would monocytosis be linked to granulomatous diseases? Answer: Monocytes are macrophages in circulation, and granulomatous diseaseas are macrophage diseases. Is it surprising that many classical granulomatous diseases are also characterized by monocytosis, because macrophages are the CHIEF cells of granulomas? Answer: NO, not surprizing, it would be logical even!
#20 Would it be a fair statement to say that whereas, neutrophilia is characterized by bacterial infections, lymphocytosis can be an index of many viral infections? Answer: Yes, it is fair, but there are many exceptions.
#21 EXTRAMEDULLARY HEMATOPOESIS is most common in the spleen, liver, and lymph nodes.
Now we move from increases of peripheral blood leukocytes to increases of marrow in general, increases in cellularity (one dimension of expansion), increases from axial to appendicular skeleton (second dimension of expansion), and increases into other organs which do not normally make marrow in adults, such as liver and spleen and lymph nodes (third dimension of expansion).
#22 CML is the CLASSIC prototype of all myeloproliferative diseases.
#23 If a CML had much more than 10% blasts, you might suspect that the patient was going into a “blast crisis”.
What is a LEUKEMOID REACTION? Ans: Extremely high benign elevations of WBCs looking like a leukemia!
#24 This marrow is virtually 100% cellularity!!! This is the HALLMARK of CML, and all the cells are still marrow cells although blasts are INCREASED, i.e., more than 1-2 %. The “spaces” are NOT fat, they are blood vessels.
This marrow is virtually 100% cellularity!!! This is the HALLMARK of CML, and all the cells are still marrow cells although blasts are INCREASED, i.e., more than 1-2 %. The “spaces” are NOT fat, they are blood vessels.
#25 This marrow is virtually 100% cellularity!!! This is the HALLMARK of CML, and all the cells are still marrow cells although blasts are INCREASED, i.e., more than 1-2 %. In this CML megakaryocytes are proliferating so what OTHER myeloproliferative disease could this be confused with? Ans: essential thrombocythemia (also called essential thrombocytosis)
#27 This marrow is about 90% cellular and looks a lot like CML. This is P. vera
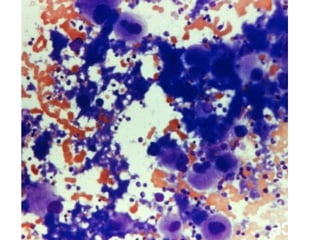
#29 Note that this is NOT a marrow biopsy but a smear, so TRUE marrow cellularity cannot be assessed, however MOST of the cells are megakaryocytes!
#30 Leukoerythroblastosis is an anemic condition resulting from space-occupying lesions in the bone marrow and characterized by the presence of immature granular leukocytes and nucleated erythrocytes in the circulating blood. Also called myelophthisic anemia.
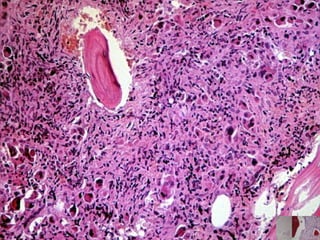
#31 Note most of the marrow looks “fibrotic”. What stain could help you confirm that this is fibrous tissue? (trichrome would stain collagen green)
#33 CHRONIC leukemias, are essentially DIFFERENT from ACUTE leukemias, sorta.
#37 The most life saving thing you can learn today is how to recognize a blast!
HUGE NUCLEUS
NUCLEOLI (stain LIGHTER not DARKER than the rest of the nucleus on Wright stain), How many nucleoli does that one blast cell have? Answer: 3
NO cytoplasmic differentiation
NOBODY IS GETTING OUT OF THIS ROOM ALIVE UNTIL THEY CAN IDENTIFY A BLAST CELL!
#38 Ataxia-Telangiectasia is characterised by:
Early-onset progressive cerebellar ataxia (difficulty with control of movement)
Ocular apraxia (difficulty following objects across visual field)
Telangiectasias of the eyes and skin
Immunodeficiency, low immunoglobulin concentrations
Chromosomal instability
Hyper-sensitivity to ionizing radiation
Increased incidence of malignancies (primarily hematologic).
Raised alpha-fetoprotein levels.[4]
Absent thymic shadow on X-ray.
Ovarian dysgenesis
#42 Are the lymphoid nuclei large? Are nucleoli present?
#43 You can usually diagnose CLL simply from a CBC printout, but should verify the cells visually.
CLL does NOT go into a blast crisis, like CML does!
#44 Many cells from CLL have a “smudge” or “basket” appearance. If you know what a NORMAL lymphocyte looks like, you can diagnose CLL purely by numbers! No marrow exam needed!
#45 Why would a CLL have hypogammaglobulinemia? ANS: LYMPHS are the precursors of plasma cells!
#47 Please memorize those THREE diagnostic features of plasma cells, the malignant plasma cells of MM look like normal plasma cells usually.
Ironically, most myelomas are recognized because they look like NORMAL plasma cells! Stand again?
#48 Normal on left, myeloma on right. Batman sign?
#49 *The presence of large proliferations of monoclonal immune proteins are believed to interfere with normal coagulation.
#50 Note the “lytic” lesions. Often the term “punched out” is used also.
#51 What if you have a plasmacytoma but NO monoclonal gammopathy?
#52 What if you have a monoclonal gammopathy but NO demonstrable proliferation of plasma cells?
#53 What is the difference between a monoclonal and a polyclonal gammopathy? (monoclonals usually show a SPIKE on serum protein electrophoresis, SPE). Monoclonals are the result of malignant proliferations, polyclonals are generally the result of chronic inflammation.
#54 Well, after CML, CLL, and ALL, all that is left is the BIG ONE!
Lets make this REAL easy…..ALL blasts look alike!!!! Why? Because there is NO cellular differentiation beyond the primitive stem cell appearance!
#55 AML’s are classified according to where the arrest occurs, i.e., the cells which proliferate in marrow and peripheral smear, and organs.
#56 Blasts, blasts with AUER rods. Auer rods are clumps of azurophilic granular material that form elongated needles seen in the cytoplasm of leukemic blasts. They are composed of fused lysosomes and contain peroxidase, lysosomal enzymes, and large crystalline inclusions.
#57 Acute promyelocytic leukemia, remember promyelocytes have BOTH nucleoli AND nonspecific granules, true BLASTS do NOT have granules.
Do you remember that M3 has a high degree of association with DIC?
#58 In AMML, M4, many of the peripheral leukemic cells look like monocytes, while in M5, Acute Monocytic Leukemia, MOST of them look like monocytes. M5 has also been called “Schilling”-type leukemia. (NOT the same Schilling of the B12 Schilling test)
#59 In M6, many of the cells may resemble erythroid cells, in M7, many of the cells may resemble megakaryocytes. But in reality you would probably never think the blasts of M7 are related to megakaryocytes.
#60 Note AMAZING similarity to ALL, clinically.
Surprised? Ans: NO
#61 Know the difference between a myelo-”proliferative” and a myelo-”dysplastic” disease.
#65 Why does the phrase “effaced architecture” appear on my pathology reports of malignant lymphomas?
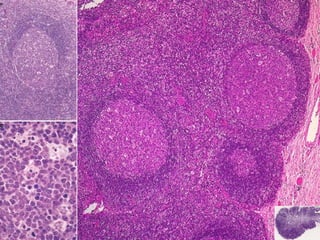
#68 BENIGN FOLLICULAR HYPERPLASIA. Larger and more numerous than normal follicles. MEDULLA may be compromised.
#69 BENIGN SINUS HISTIOCYTOSIS. The cortical area may be compromised. SINUS HISTIOCYTOSIS may be seen in reaction to cancer, even if there are NO tumor cells in the lymph node.
#70 Mention Steve Swerdlow and link to his father!
#75 Why does the pathologist often use the word “buttocks” cell, to describe a “cleaved” cell lymphoma?
#76 “HAIRY” cell leukemia/lymphoma consists of lymphocytes which look hairy, but remember, on SEM ant TEM they all look hairy!
#77 “Effacement” means any pattern in which follicles in the cortex and cords/sinuses in the medulla cannot be recognized because they are “effaced” or “obliterated”
#78 Most pathologists HATE lymphoma classifications with a passion!
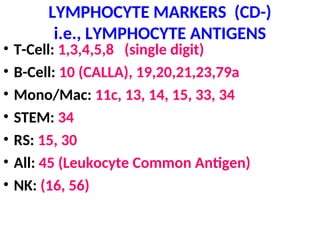
#83 If you feel the need to memorize this fine, but better to remember:
T markers <10
B markers 19-23
Mono/Mac teens
RS 15, 30
#84 Prognosis of HD disease is related directly of percentage of lymphocytes and inversely to number of RS cells.
Prognosis of HD disease is related directly of percentage of lymphocytes and inversely to number of RS cells.
Prognosis of HD disease is related directly of percentage of lymphocytes and inversely to number of RS cells.
Prognosis of HD disease is related directly of percentage of lymphocytes and inversely to number of RS cells.
Prognosis of HD disease is related directly of percentage of lymphocytes and inversely to number of RS cells.
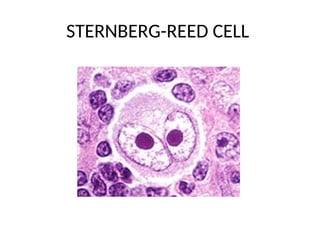
#85 STERNBERG REED cells are called “lacunar” cells in one of the most common forms of HD called NODULAR SCLEROSING
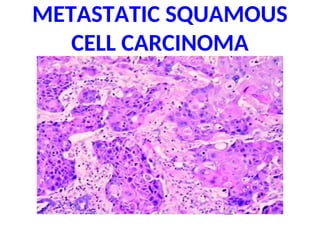
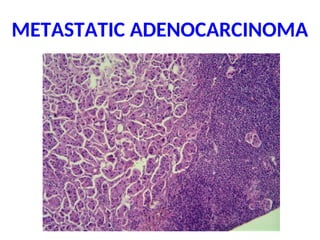
#89 If there was only one tiny microscopic focus of metastatic tumor cells in this lymph node, where would it most likely be?
#90 The subcapsular sinus of the lymph node is the FIRST place you will spot a metastatic tumor nest!
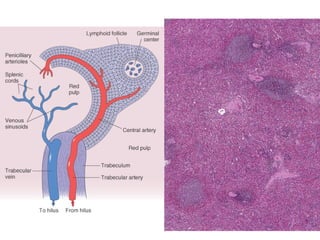
#92 We can also use the 50/50 principle generally for the spleen too: 50% “red” pulp, 50% “white” pulp.
RED PULP = RBCs (grossly and microscopically)
WHITE PULP = LYMPHS (grossly only, BLUE, microscopically)
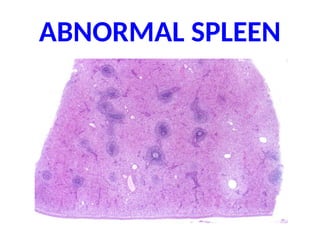
#93 Notice the “confluence” of WHITE pulp? Could this be lymphoma involvement? Ans: Yes Could this be granulomas? Ans: YES
#94 Portal hypertension, prominence of RED pulp, i.e., red pulp >> 50%
#97 What 3 malignancies have the highest preference for splenic metastases?
malignant melanoma
lymphomas
testicular germ cell tumors
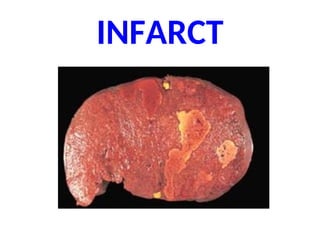
#98 Why is a splenic infarct a “pale” infarct? Answer: single end-artery blood source
#99 Note all these are benign, except fot the lymphoma. The commonest MALIGNANT tumor primary to the spleen is a LYMPHOMA, by far!
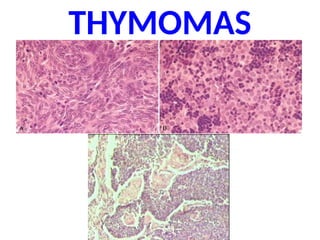
#102 Hassal’s corpuscles are fused epithelial reticular cells
#105 Benign (encapsulated), Malignant I (invasive), and Malignant II (easily metastasizable)
Note that the classification of thymomas has little to do with the appearance of the cells, but in the BEHAVIOR of the tumor grossly:
1) Encapsulated
2) Invasive
3) Metastatic





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













