
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Case Study On Ectopic Pregnancy..pdf....
Similar to Case Study On Ectopic Pregnancy..pdf.... (20)
Recently uploaded
Recently uploaded (20)
Case Study On Ectopic Pregnancy..pdf....
- 1. C M PATEL COLLEGE OF NURSING GANDHINAGAR SUBJECT: OBSTETRICS AND GYNECOLOGY NURSING TOPIC: CASE STUDY ON TUBAL ECTOPIC PREGNANCY BATCH: 2022-2024 YEAR: S.Y. MSc. NURSING SUBMITTED TO: SUBMITTED BY: Mrs Shalini Nair Rashmi Goswami Associate Professor Roll No. 04 C.M.P.C.O.N C.M.P.C.O.N Gandhinagar Gandhinagar SUBMITTED ON:
- 3. BIODATA OF THE CLIENT: Name: Jyotiben Sagar Age: 34 year Sex: Female Register No.: 126930 Ward: Gynec ward Bed No.: 09 Doctor’s unit: Dr Komal Admission date: 02/02/24 Education: 8th pass Occupation: Housewife Address: Gandhinagar Nationality: Indian Marital status: Married LMP: 19/12/23 EDD: 26/08/24 Obstetric score: G4P3L3A0 Diagnosis: Ectopic Pregnancy Surgery: Laparotomy with left Salpingectomy PRESENT HISTORY: Medical and Surgical history: Medical: Mrs Jagrutiben was having ectopic pregnancy. Surgical: Mrs Jagrutiben Sagar had undergone laparotomy with left salpingectomy on 03/02/24.
- 4. Past obstetrical history: Sr. no Year Full term Pre term Abortion Type of delivery Baby Remark Sex Alive Still birth Weight 1. 2004 Yes - - FTND M Yes - 2.7kg - 2. 2006 Yes - - FTND M Yes - 3kg - 3. 2007 Yes - - FTND F Yes - 2.5 - PRESENT OBSTETRICAL HISTORY: First trimester Second trimester Third trimester LMP:19/12/2023 Pregnancy diagnosed by UPT. Positive after 6 week of LMP Referred from PHC and diagnosed with Ectopic Pregnancy. No h/o fever, rashes, excessive vomiting, bleeding etc. -------- -------- CHIEF COMPLAINS: Mrs Jagrutiben having Abdominal pain h/o ruptured ectopic FAMILY HISTORY: Sr. no. Name of the family member Relationship with the patient Age Sex Education Occupation Health Status 1. Mr Maheshbhai Husband 35yr M 12th passed Farmer Healthy 2. Mr Sumit Son 19yr M BSc Student Healthy 3. Mr Shailesh Son 17yr M 12th std Student Healthy 4. Ms.Renuka Daughter 16yr F 11th std Student Healthy
- 5. SOCIOECONOMIC HISTORY: She belongs to a Nuclear family having 4 members. She is a housewife & her husband is an earning person in her family. Monthly income are 30,000/- . There is no history of any disease like TB, HTN, DM & hereditary disease, twin pregnancy in her family. MENSTRUAL HISTORY: Age of Menarche: 12 year Cycle: 30 days Duration: 5 days Regular/Irregular: Regular MARITAL STATUS: Type of marriage: Non consanguineous Duration of marriage: 13 years PRESENT PREGNANCY: Date of admission: 02/02/2024 Height: 156 cm Weight: 42 kg LMP: 19/12/23 HEAD TO TOE EXAMINATION: Head: Hairs were rough, No skull injury and infection, No any scar present Face: Face was looking anxious Eyes: Conjunctiva normal, Eyelids are normal Vision was normal Ear: No any discharge from the ear Hearing acuity was normal Nose: No any nasal deviation No any discharge from the nose Mouth: Lip was cracked
- 6. No gums bleeding No any tooth decay Neck: Normal ROM No Lymphadenopathy No thyroid abnormality Chest: Inspection – Breast were symmetrical Primary areola was present Nipple was erect Palpation – No lump was found Abdomen: Inspection – Striae Albicans was seen Scar: Present Palpation – Tenderness present Back: No Lordosis and no Kyphosis Extremities: Normal ROM Genital: Catherization is done VITAL SIGNS: Parameters Patient value Normal range Temperature 98 F 96.8-98.6 F Pulse 82 beats/min 70-90 beats/min Respiration 16 breaths/min 16-24 breaths/min Blood pressure 146/82 mmHg 120/80 mmHg
- 7. INVESTIGATIONS: Sr. No. Name of investigations Patient value Normal value 1 Blood count: RBC WBC Platelet count 4.46x10/cmm 12100/cmm 298000/cmm 4.2-5.4/cmm 4000-12500/cmm 150000- 450000/cmm 2. RBC indices: Haemoglobin Haematocrit MCV MCH MCHC 11.08g/dL 25.60% 81.80fl 26.20pg 32g/dL 12-14g/dL 37-47% 80-99fl 27-31pg 32-36g/dL 3. Serum Electrolytes: Serum Sodium Serum Potassium 135mEq/L 4.04mEq/L 120-160mEq/L 2.8-6.2mEq/L 4. Blood group B positive 5. Blood sugar 89.10g/dL 70-160g/dL 6. HBsAg Negative
- 8. TREATMENT: Sr. No. Name of the drug Dose Route Frequency Action 1. Inj Metronidazole 100ml IV TDS Antimicrobial 2. Inj Ondansetron 1 Amp IV TDS Antiemetic 3. Inj Pantop 40mg IV BD Proton pump inhibitor 4. Inj Tranexa 1 Amp IV TDS Antifibrinolytic 5. Inj Cefosulbactum 2g IV BD Antibiotic 6. Inj Gentamicin 240mg IV OD Antibiotic 7. Tab 1A IV SOS Antiemetic 8. Inj Tramadol 1A IV SOS Opiate analgesic 9. Tab Nifedipine 20mg Oral BD Calcium channel blocker
- 9. ANATOMY & PHYSIOLOGY: Fallopian Tube The uterine tubes are paired structures, measuring about 10 cm and are situated in the medial three-fourth of the upper free margin of the broad ligament. Each tube has got two openings, one communicating with the lateral angle of the uterine cavity called uterine opening and measures 1 mm in diameter, the other is on the lateral end of the tube, called pelvic opening or abdominal ostium and measures about 2 mm in diameter. PARTS: There are four parts. From medial to lateral are- 1. Intramural or interstitial lying in the uterine wall and measures 1.25 cm in length and 1 mm in diameter 2. Isthmus-almost straight and measures about 3-4 cm in length and 2 mm in diameter 3. Ampulla -tortuous part and measures about 5 cm in length which ends in 4. Wide Infundibulum measuring about 1.25 cm long with a maximum diameter of 6mm. The abdominal ostium is surrounded by a number of radiating fimbriae (20- 25%), one of these is longer the rest and is attached to the outer pole of the ovary called ovarian fimbria. STRUCTURES It consists of 3 layers- 1) Serous consists of peritonnum on all sides except along the line of attachment of mesosalpinx . 2) Muscular-arranged in two layers outer longitudinal and inner circular.
- 10. 3) Mucous membrane has three different cell types and is thrown into longitudinal folds. The epithelium rests on a delicate vascular reticulum of connective tissue Mucous membrane is lined by i. Columnar ciliated epithelial cells that are most predominant near the ovarian end of the tube. These cells compose 25% of the mucosal cells ii. Secretory columnar cells are present at the isthmic segment and compose 60% of epithelial cells iii. Peg cells are found in between the above two cells. They are the variant of secretory cells FUNCTIONS: The important functions of the tubes are: i. Transport of the gametes ii. To facilitate fertilization and survival of zygote through its secretion BLOOD SUPPLY: Arterial supply is from the uterine and ovarian Venous drainage is through the Pampiniform plexus into the ovarian veins. LYMPHATICS: The lymphatics run along the ovarian vessels to Paraaortic nodes. NERVE SUPPLY: The nerve supply is derived from the uterine and ovarian nerves. The tube is very much sensitive to handling. DEVELOPMENT: The tube is developed from the upper vertical part of the corresponding Mullerian duct at about 6-10th week.
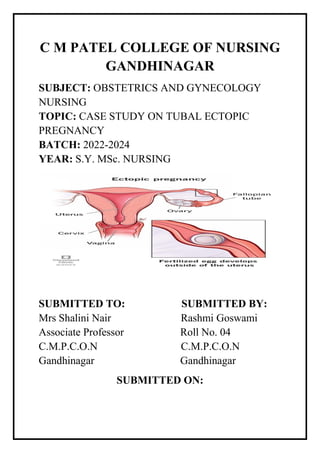
- 11. DISEASE CONDITION: Ectopic Pregnancy Definition: An ectopic pregnancy is one in which the fertilized ovum is implanted and develops outside the normal endometrial cavity. Sites of Implantation: Tubal pregnancy A tubal pregnancy the most common type of ectopic pregnancy happens when a fertilized egg gets stuck on its way to the uterus, often because the Fallopian tube is damaged by inflammation or is misshapen. Hormonal imbalances or abnormal development of the fertilized egg also might play a role.
- 12. Etiology: In Book In Patient In majority, causes are not known Possible causes are: Salpingitis and PID Contraception failure such as IUD, Sterilization operation, use of Progestin only pill etc. Tubal surgery Intrapelvic adhesion following pelvic surgery ART such as IVF Others such as - Previous ectopic pregnancy - Developmental defect Idiopathic (causes are not known) Signs and Symptoms: 1. Acute In Book In Patient Persistent unilateral uneasiness Absent Abdominal Pain Present Appearance of vaginal bleeding Present Vomiting and fainting attack Absent Pallor skin and becomes cold Absent Lower abdomen becomes tense and tender, no mass is felt Present Extreme tenderness on fornix Absent 2. Unruptured In Book In Patient Continuous uneasiness on one side of the flank/ colicky pain Not occurs because it ruptured Presence of delayed period 3. Sub-acute In Book In Patient Amenorrhea Amenorrhea Lower abdominal pain Not occur Vaginal bleeding is more dark
- 13. Diagnosis: In Book In Patient Blood examination such as Hb, Grouping & Rh typing, Total WBC count, Differential count. Done Culdocentesis Not done Urinary hCG test Done USG Done Laparoscopy Not done Complications: In Book In Patient Rupture Present Internal bleeding Present Maternal death Absent Management: In acute cases: In Book In Patient Hospitalization Done Ringer’s solution is started Started Blood transfusion Given Laparotomy with Salpingectomy, Oophrectomy, sub-total hysterectomy Laparotomy with left Salpingectomy done In sub-acute or chronic cases: In Book In Patient Hospitalization Management done according to acute type Laparotomy In unruptured cases: In Book In Patient Drugs such as Methotrexate, Prostaglandin are given for salpingocentesis Management done according to acute type Linear salpingectomy
- 14. NURSING PROCESS: List of nursing Diagnosis 1. Acute abdominal pain related to ruptured ectopic as evidenced by verbalization of pain. 2. Risk for deficient fluid volume related to bleeding from a ruptured ectopic pregnancy. 3. Deficient knowledge related to unfamiliarity with information resources as evidenced by inaccurate follow up of instructions. 4. Powerlessness related to early loss of pregnancy as evidenced by fainting. 5. Anxiety related to fear of prognosis as evidenced by restlessness.
- 15. Assessment Diagnosis Expected outcome Intervention Rationale Evaluation Subjective data: Client says that “I am having pain”. Objective data: Verbalization of pain. Acute abdominal pain related to ruptured ectopic as evidenced by verbalization of pain. The client will get relieve from pain. - Assess blood pressure and pulse every one hour. - Assess for signs of dehydration, skin turgor. - Position patient with comfort and assist with movement as needed. - Monitor intake and output. - Maintain NPO status insert catheter & maintain IV. - The patient may go into shock and will have rapid heart rate, rapid breathing and low BP. - Excessive blood loss and vomiting may cause hypovolemia and dehydration. - Patients should be positioned lying flat on the bed to reduce movement, stabilize vitals, and promote comfort. - To maintain renal function. - Helps in a surgery. Surgery has performed.
- 16. Assessment Diagnosis Expected outcome Intervention Rationale Evaluation Subjective data: ------ Objective data: -------- Risk for deficient fluid volume related to bleeding from a ruptured ectopic pregnancy. The client must maintain adequate fluid volume at a functional level. - Assess the clients vital signs and closely monitoring BP and pulse rate. - Monitor intake and output. - Ensure that the patient is comfortable with her position.. - Monitor the patient’s pain status. - To obtain baseline data. - To maintain adequate renal function.. - This attitude will relieve her symptoms. - To obtain baseline data -------
- 17. Assessment Diagnosis Expected outcome Intervention Rationale Evaluation Subjective data: Client says that” please provide me with the necessary information” Objective data: Inaccurate follow up of instruction. Deficient knowledge related to unfamiliarity with information resources as evidenced by inaccurate follow up of instructions. The client verbalizes understanding of the disease process and appropriate treatment plan. - Assess the client’s knowledge of the disease process. - Provide information about signs/sympto ms indicating worsening of the condition. - Inform the client about her health status and result of tests. - Reinforce the importance of adhering to treatment regimens. - Establishes a database and provides information. - Helps ensure that the client seeks timely treatment and may prevent complications. Instruct the client to report headache. - When the client understands the consequences of inadequate intervention and is motivated to achieve health. - Lack of engagement in the treatment plan will result for failure of therapy. The client is able to follow instructions and has got little knowledge about her condition.
- 19. HEALTH EDUCATION: Activity: (Do’s and Don’ts) Rest for a week after the surgery. Avoid doing heavy exercise. Avoid sexual intercourse about a week. Don’t lift anything heavier to prevent straining of incisions. Walk as often as you can. Other home care activity: Continue with the coughing and deep breathing exercises. To prevent constipation - Eat fruits, vegetables and whole grains. - Drink 6 to 8 glasses of water everyday. Wash your incision with mild soap and water. Pat it dry. Don’t use oils, powders, or lotions on incision. Shower as normal. Follow up care: Make a follow up appointment.
- 20. PROGRESS NOTES: Day:-1 My client Jagrutiben was admitted in civil hospital Gandhinagar with complains of abdominal pain, and history of ectopic rupture. She was taken for emergency laparotomy with left salpingectomy. During time of admission her vital sign was: Vital signs Patient value Normal value Temperature 98 F 98.6 F Pulse 76bpm 70-90bpm Respiration 18bpm 18-24bpm Blood pressure 150/95mmHg 120/80mmHg Day 2: Jagrutiben was feeling fatigue and was having abdominal pain. Advise to rest and sleep. Vital signs were recorded Vital signs Patient value Normal value Temperature 98 F 98.6 F Pulse 72bpm 70-90bpm Respiration 16bpm 18-24bpm Blood pressure 135/100mmHg 120/80mmHg Same medicine was continued on the second day. Day 3: On 3rd day, her health improved much better. She was fully co-operative in all the procedures. Advise her for ambulation. The same medications were continued on the third day. Following vital sign recorded on 3rd day. Vital signs Patient value Normal value Temperature 98 F 98.6 F Pulse 80bpm 70-90bpm Respiration 22bpm 18-24bpm Blood pressure 150/90mmHg 120/80mmHg
- 21. SUMMARY My Patient came with complain of abdominal pain and ruptured ectopic. Patient is 4th gravid women. On admission she is having abdominal pain and came with the history of ruptured ectopic so she is taken for emergency laparotomy and left Salpingectomy. After providing 4 days care with health education to her she is maintaining stable vital parameters, so doctors gave discharge to my client.
- 22. CONCLUSION: During my clinical posting in civil hospital in antenatal ward, I got chance to provide care to, Mrs Jagrutiben with diagnosis of Ectopic pregnancy by this study I learn in detail about Ectopic definition, causes and its management. I thank my client for her cooperation and my clinical coordinator for her valuable guidance.
- 23. BIBLIOGRAPHY Basvanthappa B.T : “TEXT BOOK OF MIDWIFERY AND REPRODUCTIVE HEALTH NURSING”; 1st edition 2006, Jaypee brother publication, New Delhi. Dutta D.C : “TEXT BOOK OF OBTETRICS” ; 7th Edition , 2004; New central book agency publication, Calcutta. Page no: 177 -185 Jacob Anamma : “A COMPREHENSIVE TEXT BOOK OF MIDWIFEREEY”;1st edition 2005; Jaypee brother medical publication; New Delhi, Kumari Neelam; (2010); 1st edition; “MIDWIFERY AND GYNAECOLOGICAL NURSING”; S.vikas and company; Jalandhar city Myles: “ TEXT BOOK OF MIDWIVES” ; 14th edition,2003 Elsevier publisher, Philadelphia. Rao Kamini “TEXT BOOK OF MIDWIFERY AND OBSTETRICS FOR NURSES”; First edition, 2011, Elsevier publisher, Philadelphia REFERENCES https://medicoapps.org/ectopic-pregnancy-4/ https://www.scribd.com/document/401805305/Case-Presentation- on-Ectopic-Pregnancy-New https://www.saintlukeskc.org/health-library/after-laparoscopic- treatment-ectopic- pregnancy#:~:text=Don't%20lift%20anything%20heavier,longer %20taking%20prescription%20pain%20medicine.