Background
Testicular cancer isthe most common malignancy in men aged 15 to 45
years and represents one of the most common curable malignancies
when identified promptly and treated with a multimodal approach. It
represents 1% of male tumors and 5% of urological malignancies.
Insiden
10% of
Newborns
♂>♀
5.
Objectives
• Identify thedefinition, etiology, clinical symptoms and
treatment of testicular cancer medical conditions and
emergencies.
• Summarize the appropriate evaluation of testicular cancer.
• Review the management options available for testicular
cancer.
Writing Method
This case report is prepared based on a literature study that
refers to several literatures.
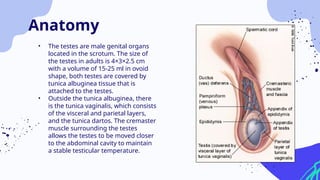
• The testesare male genital organs
located in the scrotum. The size of
the testes in adults is 4×3×2.5 cm
with a volume of 15-25 ml in ovoid
shape, both testes are covered by
tunica albuginea tissue that is
attached to the testes.
• Outside the tunica albuginea, there
is the tunica vaginalis, which consists
of the visceral and parietal layers,
and the tunica dartos. The cremaster
muscle surrounding the testes
allows the testes to be moved closer
to the abdominal cavity to maintain
a stable testicular temperature.
Anatomy
8.
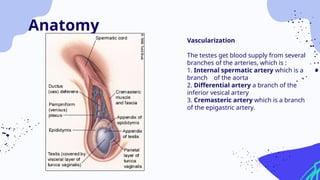
Vascularization
The testes getblood supply from several
branches of the arteries, which is :
1. Internal spermatic artery which is a
branch of the aorta
2. Differential artery a branch of the
inferior vesical artery
3. Cremasteric artery which is a branch
of the epigastric artery.
Anatomy
9.
The incidence oftesticular cancer shows different figures in each country, as well as in each
race and socioeconomic level. In Scandinavian countries, 6.7 new cases out of 100,000 men are
reported annually, while in Japan there are 0.8 out of 100,000 men. In the United States, 6900
new cases of testicular cancer are found each year.
The peak incidence of testicular tumor cases occurs in late adolescence to early adulthood (20-
40 years), in late adulthood. adults (over 60 years) and in children (0-10 years). Overall, the
highest incidence of testicular tumors occurs in young adult men, making this tumor the most
common noeplasma in men aged 20-34 years and the second most common tumor in men
aged 35-40 years in the United States and United Kingdom.
Epidemiology
10.
.Most testicular canceroccurs under the age of 40 years. The exact
cause is unknown, but there are several factors that contribute to the
development of testicular cancer:
1. Undescended testes (testes that do not descend into the scrotum)
2. Abnormal testicular development
3. Klinefelter syndrome (a sexual chromosomal disorder characterized
by low levels of male hormones, infertility, enlarged breasts
(gynecomastia) and small testicles).
Aetiology
11.
Testicular cancer isgrouped into:
1. Seminomas: 30-40% of all types of testicular tumors.
2. Usually found in men aged 30-40 years and limited to the testes.
3. Non-seminomas: constitute 60% of all testicular tumors. Divided into subcategories:
a) Embryonic carcinoma
b) Yolk sac tumors
c) Teratoma
d) Stromal cell tumors
Aetiology
12.
Symptoms include:
1. Thetesticles are enlarged or feel strange (unusual).
2. A lump or swelling in one or both testicles.
3. Dull pain in the back or lower abdomen – Gynecomastia.
4. Discomfort / pain in the testicles or scrotum feels heavy.
Clinical Manifestation
13.
But there mayalso be no symptoms at all. Symptoms develop very gradually
with a painless mass or lump in the testicle. Patients may complain of
tightness in the scrotum, inguinal area, or deep abdomen. Low back pain
(due to expansion of the retroperineal nodes), abdominal pain, weight loss,
and general weakness may result from metastases. Painless enlargement of
the testicle is a significant diagnostic finding.
14.
Diagnostic Evaluation carriedout to establish the diagnosis of testicular cancer:
1. Scrotal Ultrasound is used to determine the exact location of the tumor, the
characteristics of the lump whether it is a cyst or solid (solid), is a single form or a
collection of several tumors.
2. CT Scan is used to determine the presence of metastases, especially the location of the
metastases.
3. Blood tests are also done to identify and confirm the specifications, signs and size of the
tumor. AFP Alpha 1 feto protein, Beta-HCG, and LDH are blood tests to identify the
type of testicular tumor.
Diagnostic Evaluation
15.
According to theTNM Classification of Malignant Tumors as published in the AJCC
Cancer Staging Manual, testicular cancer is divided into three (3) levels:
1. Stage 1: the tumor is still localized in the testes
2. Stage 2: The tumor has spread to the testes and has metastasized to the retroperitoneal
and/or paraaortic lymph nodes (lymph nodes under the diaphragm).
3. Stage 3: The tumor grows and spreads in the testes and metastasizes to more than the
retroperitoneal cavity and/or paraaortic lymph nodes.
Management
16.
Treatment of testiculartumors basically consists of three types :
1. Surgical procedure.The most common testicular tumor surgery is an orchidectomy.
2. Radiotherapy. Radiation is usually used to treat testicular tumors, which are grade 2
seminomas, but also in cases with grade 1 seminomas to minimize growth and prevent
tumor spread
3. Chemotherapy is the standard treatment for nonseminoma cancer when the cancer
has spread to several parts of the body (stage 2 and stage 3). There are three standard
protocols of chemotherapy, which consist of Bleomycin – Etoposide – Cisplatin (BEP)
Management
17.
A hard intratesticularmass is a diagnostic of testicular cancer unless proven
otherwise. However, some other diagnoses to consider while evaluating a
testicular mass include:
1. Epididymo-orchitis
2. Hematoma
3. Inguinal hernia
4. Hydrocele
5. Spermatocele or epididymal head cyst
6. Varicocele
7. Lymphoma (the most common finding in bilateral testis lesions in older
men)
8. Metastasis from other cancers (eg, lung cancer, melanoma, prostate
cancer)
9. Syphilitic gumma
Diferential Diagnosis
18.
Complications due totesticular malignancy can be broadly classified into two
groups:
Complications secondary to the disease itself:
1. Chronic fatigue
2. Anxiety disorders
3. Metastatic complications
4. Venous thromboembolism
Complication
19.
Prognosis
Prognosis is majorlydetermined by the histology, extent of distant tumor spread, and extent of tumor marker
elevations. For men with disseminated seminomas, the main adverse prognostic variable is the presence of
metastases to visceral organs other than the lungs. A tumor that originated in the mediastinum has a worse
prognosis when compared to a tumor that originated within the testicle. Nonetheless, even patients with
widespread metastases at presentation, including those with brain metastases, may have a curable disease and
should be treated with this intent.
Patient’s Identity
Identity Patient
Name: B.Bryan
Age
N.MR
: 4 years old
: 166388
Sex
Profession
: Male
: -
Marriage status
Ethnic
: -
: Minang
Religion
Address
: Islam
: Tanjung Barlulak
Admitted on : 13 September 2022
22.
. Abdominal pain,mild backpain and a big testis on left side.
Chief Complain
23.
Severe abdominalpain
Mild backpain
Swelling on left side of testis past 2 years
Did not came at early stage due to financial issue.
History of Present Illness
24.
No pasthistory of any disease of medical importance
Patient do not suffer from any allergies
History of Past Illness
25.
History On anyMedication or Drug Use
Patient does not on any medication.
Family History
Patient’s mother suffers from vaginal tumor when she was 19 years
old
Riwayat Pekerjaan, Sosial, Ekonomi
Middle class and Average Social Economy status
Riwayat Alergi
Does not have any allergies
26.
Status Internus
Hair :Black in colour
Skin and Nail : Good skin turgidity, no sign of sianosis
Head : Normocephal, trauma (-), hematoma (-)
Eyes : AC (- / -). IS (- / -)
Nose : No abnormalities found
Ears : No abnormalities found
Neck : JVP 5+2 cmH2O, Mass (-), an enlarged lymph node found on
the left side of neck
27.
Lungs
• Inspection :Simmetric, bilateral equal air entry
• Palpation : Fremitus left = rigt
• Percussion : No abnormalities found
• Auscultation : Normal vesicular breathing, rhonki -/-,
wheezing -/-
28.
Heart
• Inspection :ictus cordis not visible
• Palpation : Ictus cordis palpable 2 fingers medial
line mid clavicula sinistra ICS V
• Percussion : No abnormalities found
• Auscultation : S1-S2 reguler, murmur (-),
gallop (-)
29.
Abdomen
• Inspection :Distension (-), no other abnormalities
• Palpation : No organomegali or asitesor bruit
• Percussion : Timpani
• Auscultation : Bowel sound (+) normal
• Genitalia : left scrotom was big (about 1 x 1 x 0.5 cm)
with a round and firm testis.
• Anus : No
abnormalities found
• Extremities : Warm, CRT < 2 s
Findings : Noabnormalities found in heart and lungs
Thorax X-ray Image PA
34.
Ultrasonagraphy Image
Interpretation :The size of the testicles enlarges.
Inhomogenic parencymal ecoscult. Calsified solid
lesion filled the testicles (s) with fluid. Vascular
flow in the testicular parenchyma increases.
Findings:
Left testicular solid calcified mass, DD/ Teratoma, Germ
cell tumor
Hydrocele Sinistra
35.
Definitive Diagnosis
Hydrocele Sinistra+ Sus Testicular Cancer+Mild Anemic
Differential Diagnosis
Orchio epididymitis, Spermatokel, Hematoma and Torsio
testicles
List of the problems
• An enlarged lymph node found on the left side of neck.
• Abdominal pain
• Anemic
• Hidrocele
36.
Therapy :
• Observationand follow up on vital sign
• Bed Rest
Medication :
• IVFD KA EN 1B 500 mL
• Paracetamol Syr 3x1 ½ Cth
• Transfusion of PRC 1x 200
• Medical procedures
Radical Inguinal Orchiectomy
Biopsi
Radiotherapy and Kemotherapy
Management/ Therapy
37.
Patient Education :
Educate patient’s condition and risk factors to the patients family
Self Higiene
38.
Prognosis
1. Quo advitam : bonam
2. Quo ad sanam : bonam
3. Quo a functionam : bonam
39.
• 13 September2022
S/ Left side of the testicle enlarged, Abdominal pain (+)
O/ Size of the left side scrotum as big as marble.
A/ Suspek Hidrocele
P/ Konsult dr. Roza Child Specialist : Transfusion 1 PRC 1x 200cc,
VFD KA EN IB 12gtt/I and Paracetamol Syr 3x1.5 cth
• 14 September 2022
S/ Left side of the testicle enlarged, Abdominal pain (+)
O/ There is no changes in size of the scrotum, Vital signs are in normal
condition. After the USG examination, result: Calsified solid lesion filled the
testicles (s) with fluid.
A/ Hidrocele + Sus. Testicles Cancer
P/ Paracetamol Syr 3x1.5 Cth
Follow Up Data
40.
• 15 September2022
S/ Left side of the testicle enlarged, Abdominal pain (+), an enlarged lymph node found
on the left side of neck.
O/ Vital signs are in normal level. There is a new enlarged lymph node and it could be a
sign of metastases. Patient suffers in pain.
A/ Hidrocele Sinistra + Sus. Testicle Cancer
P/ Pronalges Suppositoria 1/2, Ketorolac 2x1/2, Transfusion 1 PRC, PCT Syrup 3x1/2 cth
• 16 September 2022
S/ Left side of the testicle enlarged, Abdominal pain (-), an enlarged lymph node found
on the left side of neck.
O/ Vital signs are in normal level. Patient seems to be relax. Post transfusion PRC.
Request for HB lab test.
A/ Hidrocele Sinistra + Sus. Testicle Cancer
P/ Pronalges Suppositoria 1/2, Ketorolac 2x1/2, PCT Syrup 3x1/2 cth
Follow Up Data
41.
• 17 September2022
S/ Left side of the testicle enlarged, Abdominal pain (-), an enlarged lymph node found
on the left side of neck.
O/ Vital signs are in normal level. The corrected HB level is 12.2 gr/dl
A/ Hidrocele Sinistra + Sus. Testicle Cancer
P/ Due to complications this patient refer to Department of Urology Central General
Hospital Dr.M. Djamil.
• A malepatient named B.B aged 4 years old from Tanjung Barlulak
presented chief complain with an enlarged scrotum by the left side,
abdominal pain and mild back pain to surgical policlinic RSUD Prof Dr.
Hanafiah, Batusangkar. We insist patient’s parents to make USG
examination and blood test as a first step. Before that we asked the history
of current illness and as well as we did physical examination. From the
physical examination we found an enlarged left side of the scrotum. So we
made a working diagnosis as Suspek Hidrocele Sinistra.
44.
• A hydroceleis an abnormal collection of serous fluid between the two layers of tunica
vaginalis of testis. It can either be congenital or acquired.
• The majority of patients with hydrocele present with the complaint of painless scrotal
swelling rendering the testes impalpable with positive transillumination and
fluctuation. The examiner should look at this swelling in both the supine and upright
positions. common predisposing factor for hydrocele is residing in a warm climate. As
it is painless, it acquires a prodigious size before the patient seeks medical attention.
In contrast, the secondary hydrocele is generally smaller, with the exception of filarial
hydrocele.
45.
1. As permention above, the patient does not feel any pain when examined
patient’s testis yet patient’s abdominal area still in pain. From the
interpretation USG result we have found that the size of the testicles
enlarges. Inhomogenic parencymal ecoscult. Calsified solid lesion filled
the testicles (s) with fluid. Vascular flow in the testicular parenchyma
increases. In the findings they have mentioned left testicular solid
calcified mass, DD/ Teratoma, Germ cell tumor and Hydrocele Sinistra.
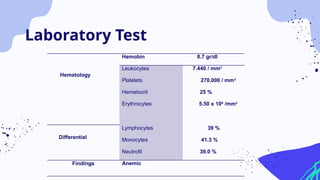
Then the lab test result findings mentioned the patient suffering mild
anemia as well. So we consult child specialist for opinion. Later we correct
the hemoglobin level with 1 unit of PRC. At the same time,we planned
pain management on this patient because patient still suffering
abdominal pain. So Pronalges Suppositoria 1/2, Ketorolac 2x1/2 and PCT
Syrup 3x1/2 cth as pain management medication.
46.
There is anew enlarged lymph node found when we did physical examination and it
could be a sign of metastases.
The size of the enlarged lymph node as big as a marble, consistency soft and spongy
found on left side of the patient’s neck. The classic presentation of testicular tumor is a
swollen, painless and hard testis in a man in the third of fourth decade of his life.
Depending on the amount of disease, clinical stage and the presence of metastases, the
presentation can vary such as: Dull ache or heaviness in lower abdomen, acute scrotal
pain (10%), lower limb swelling (5%), neck mass, anorexia, vomiting, cough, back ache,
gynecomastia (5%) and infertility (rarely).
In the early stage, patients may have no symptoms at all and their cancer may be found
incidentally during routine physical exams. The clinical symptoms has indicates that it
could be testicular cancer. The diagnosis of testicular cancer is based on physical exams
and ultrasound findings.
47.
At first, weplanned to do hydrocelectomy after corrected hemoglobin level of
the patient if there is no complication found in USG findings. But now we
suspect that this patient might suffering from testicular cancer. Some
imaging tests can be used to detect abnormalities in testicle including,
Scrotal Ultrasound, Chest X-ray, Computed Tomography (CT), Magnetic
Resonance Imaging (MRI), Positron Emission Tomography (PET).
We can use some medical procedures for diagnosis Testicular cancer which is
Radical inguinal orchiectomy and biopsy followed by a tailored oncological
follow-up. Radical inguinal orchiectomy is the procedure testis and spermatic
cord are removed through an incision in the groin. Then the testis is
examined by a pathologist. Biopsy used when the cancer diagnosis is
uncertain, this procedure used to remove a sample of tumor tissue and test
te sample wheather benign or malignant tumor.