Functional Mobility ofthe
Functional Mobility of the
Floor of the Mouth
Floor of the Mouth
Neil’s Lateral Throat Form
Class I - > ½ ” MHR to RMF
(70%)
Class II – < ½ ” MHR to RMF
(25%)
Class III- complete mirror
displacement (5%)
Huang P-S, et al. Int J Prosthodont 2007;20;640-2.
2.
The Role ofthe Tongue in
The Role of the Tongue in
Retention
Retention
Desjardins RP. JADA 1974;88:814-22.
Amount of Saliva
Amountof Saliva
• Normal
• Excessive
• Insufficient
Ship JA, et al. J Am Geriatr Soc 2002;50:535-43.
20% of pop. 65+
2-3X incidence in
institutions.
8.
Xerostomia
Xerostomia
• 493 denturewearers
• Mean age 67
• Denture instability,
discomfort and
dissatisfaction
significantly related
to xerostomia
Ikebe K, et al. Oral Med Oral Pathol Oral Radiol 2005;99:704-10.
salivary output
.1ml/minute
9.
Xerostomia
Xerostomia
• 493 denturewearers
• Mean age 67
• Denture instability,
discomfort and
dissatisfaction
significantly related
to xerostomia
Ikebe K, et al. Oral Med Oral Pathol Oral Radiol 2005;99:704-10.
Sjogren’s Syndrome
Sjogren’s Syndrome
•Chronic inflammatory
disease of exocrine
glands
• 2nd
most common
autoimmune disease
• 9:1 female/male
• Salivary gland
enlargement 25%-67%
• Confirm diagnosis with
biopsy of minor salivary
glands.
Fox PC, et al. JADA 2008;1592-1601.
Attitude of Patient
Attitudeof Patient
Hysterical
previous poor
results
problem
insurmountable
personal tragedy.
17.
Attitude of Patient
Attitudeof Patient
Indifferent
little appreciation
resign easily
at the behest of
others.
19.
Is the HouseClassification
Is the House Classification
Too Narrow?
Too Narrow?
Gamer S, et al. J Prosthet Dent 2003;89:297-302.
20.
Diagnostic Findings
Diagnostic Findings
11-15mm residual mandibular bone height
Type C maxilla- minimally resists h/v movement
Muscle attachments do cause instability
Class II maxillomandibular relationship
PP surgery needed for pendulous tuberosities
Limited posterior interarch space
TMD, retruded tongue
Moderate psychosocial considerations.
21.
ACP Classification System
ACPClassification System
Class III
11-15 mm residual mandibular bone height
Type C maxilla- minimally resists h/v movement
Muscle attachments do cause instability
Class II maxillomandibular relationship
PP surgery needed pendulous tuberosities
TMD, retruded tongue, hyperactive gag reflex
Limited interarch space
Moderate psychosocial considerations
Pretreatment Confirmation Letter
PretreatmentConfirmation Letter
1. Salutation
2. Statement of problems
3. Outline of proposed therapy
4. Alternative therapy
5. Limitations
6. Consequences of therapy or no treatment
7. Fee and payment schedule
8. No guarantee clause
9. Duration of treatment
10. Realistic closing
Type 2 Diabetes
Type2 Diabetes
Cristina de Lima D, et al. J Prosthet Dent 2008;99:60-5.
10+% over 65 yrs.
Obesity/sedentariness
Sixth leading cause of
mortality among the
elderly
No sig. difference in
salivary flow, denture
retention, oral lesions
29.
Iatrosedative Interview
Iatrosedative Interview
Whatkind of difficulties are
you having?
I am awfully unhappy.
Unhappy?
I have grown into an old
woman long before my
time. The day they removed
my teeth I felt I aged 20
years.
The feeling must be quite
distressing, but you don’t
seem elderly to me.
Landesman HM. Boucher’s Prosthodontic Treatment for Edentulous Patients
30.
Exploring the Problem
Exploringthe Problem
Yes, everyone tells me that, but that’s
how I feel.
I agree with you, in the end, it is only how
we feel that matters… Aside from the
fact that the loss of teeth makes you
feel like an old woman, how are you
having difficulty with it?
It is uncomfortable, slips, and I have a
burning sensation, but I keep it in all
the time, because I hate the way I look
without it.
31.
As I understandit, you have had several
dentures made.
Yes, none of them worked. To be honest I don’t
know why I came to see you.
Why did you?
Well, I haven’t given up.
You were not happy with the previous
dentists?
Each one was quite confident they could
make a denture that fit.
But you were talking about your emotional
distress, mostly.
Exactly, you seem to appreciate what I am
going through.
32.
Post-examination
Post-examination
You mentioned thatyou hate wearing dentures.
Did your parents have them?
Yes, my mother did and she suffered terribly; I
was frightened it might happen to me.
Did you ever get used to the idea?
No, I will never forget the first sight of my mom
without dentures, so shrunken…
Did you tell the dentist how you felt?
Yes, he didn’t seem to care too much, and said
I should get used to it and get along fine.
How did that make you feel?
Angry and even more frightened…
33.
Interpretation
Interpretation
You may havelearned to fear having
dentures because of your mother’s
unhappy experience. But I want you to
know your feelings can change and
with that change we can expect you to
wear dentures with comfort. Although
tender, your gums are healthy. But the
stress of your unhappiness can affect
the way your gums tolerate the
pressure of dentures.
34.
Offering a Solution
Offeringa Solution
As we work together, I am encouraged that
your feelings about yourself and your
dentures will change so that you can live
with them comfortably.
It may take as long as 3-4 months.
Why so long?
It takes time to make dentures that you will be
able to function with properly.
The day I place them is the result of all our
preparation, but it is in essence the first day
of treatment and I will be available to help
make you comfortable.
35.
Response
Response
I really appreciatethat , doctor. The other
doctors were so impatient with me and didn’t
seem to realize that I was suffering so much
emotionally. I feel hopeful and would like us
to start.
Good, I am glad you are optimistic about our
working together. I would like you to bring
some photographs in to aid in the
arrangement of teeth.
I will start looking for them. I think I had some
wedding pictures when I had a big smile on
my face.
36.
Limited Adaptive Ability
LimitedAdaptive Ability
I am very concerned about your progress at this point.
We have done everything we can do together and
most patients would be able to manage these
dentures. I am confident the stress of losing your
teeth is still affecting you.
I think we should bring someone in to help us with
these stress factors.
No, I don’t think I am emotionally disturbed.
I did not mean to imply that you were an emotionally
disturbed individual. We all have specific areas in
our lives that are upsetting, but without solving this
emotional aspect, we chance failure again. Call me
next week and let’s discuss this over the phone.
Eitner S, et al. Int J Prosthodont 2007;20:538-45.
ACP Classification System
ACPClassification System
Class 1
>21 mm residual mandibular bone height
Type A maxilla-resists h/v movement
Muscle attachments do not cause
instability
Class I maxillomandibular relationship
39.
ACP Classification System
ACPClassification System
Class II
Residual bone height- 16-20mm
Maxillary RR- resists h/v movement
Muscle attachments-limited influence
Class I maxillomandibular relationship
Mild psychosocial, systemic disease
40.
ACP Classification System
ACPClassification System
Class III
11-15 mm residual mandibular bone height
Type C maxilla- minimally resists h/v movement
Muscle attachments do cause instability
Class I, II, III maxillomandibular relationship
Preprosthetic surgery needed
TMD, tongue hyperactivity, hyperactive gag/r
Limited interarch space, mod. oral manifestations
Moderate psychosocial considerations
41.
ACP Classification System
ACPClassification System
Class IV
10mm or less RRH on mandible
Class I, II, III maxillomandibular relationship
Max. RR no resistance to h/v movement
Significant denture base instability from
muscle attachments
Major preprosthetic surgery required, e.g. hard
tissue augmentation, correction of dental
facial deformities, complex implant
placement
Editor's Notes
#1
The importance of this assessment is that it indicates the amount of possible retromylohyoid flange which when available aids in retention by engaging the convexity of the tongue.
This will aid in impression extensions and will help with the assessment of the functional retromylohyoid fold
Int J Prosthodont. ;20 (6):640-2 18069375 (P,S,E,B)
The proportion of 3 classes of lateral throat form. Pei-Sheng Huang, Tsau-Mau Chou, Hong-Po Chang, Jen-Hao Chen, Huey-Er Lee, Hong-Sen Chen, Dorsey J Moore
The aim of this study was to investigate the proportion of 3 Neil's classifications of lateral throat forms and the difference in the length of the lateral throat form between the dentures and the patient's actual anatomy. The classification of lateral throat form was determined by the patient's functional movements, and an implant depth gauge was used to measure the length of the lateral throat form in the patient's mouth and compare it to that of the dentures. One hundred mandibular edentulous patients were measured. The proportion of Neil's Class I lateral throat form was 70%, the proportion of Class II was 25%, and the proportion of Class III was 5%. The mean difference between the actual lateral throat forms and the dentures was 6.7 +/- 2.9 mm at the anterior point of measurement (from the anterior part of the retromolar pad to the mouth floor) and 10.0 +/- 3.7 mm at the posterior point (from the middle of the retromolar pad to the mouth floor). The difference in length between the ridge height of the mouth and the denture was statistically significant (P < .001).
#2 Excessive bulk will deprive the tongue of its space. Here the convexity of the tongue facilitates retention by having available the lingual flange down to the base of the MBF.
The MLH attaches to the MLH ridge in an ascending direction posteriorly. The ridge is covered by very thin mucosa and may require relief. Note that in the molar region lingual flanges slope towards the tongue and extend in length below the attachment of the mylohyoid muscles on mylohyoid region. Slope of the lingual flange allows the mylohyoid to contract and raise floor of the mouth without raising the denture. Length of the lingual flange in the molar region allows it to reach mucolingual fold in tissl flange turns laterally toward mandible to fit inti the retromylohyoid fossa. This part of the denture guides the tongue onto the top of the lingual flange.ue of the floor of the mouth to maintain seal of lower denture.
#3 Surgical intervention of the frenular attachments is contraindicated in most cases.
#6 Ideally there should be a moderate amount of serous type of saliva, which is the prevailing finding. A saliva that is thick and ropy made up of heavy mucous secretions from the palatal glands under the maxillary denture. The very thickness of the saliva is sufficient to force the dentures out of their correct position.The thick ropy saliva also complicates impression taking as it creates voids in the impression. Gauze with Cetacaine wiped over the palatal glands can paralyze the glands and eliminate as much as possible this output.
#7 The amount and consistency of saliva will affect the retention and stability of dentures and the comfort with which patients can wear them. An excess of saliva will complicate impression making and be an annoyance to patients. This is usually much worse when dentures are new. They may feel like foreign objects and stimulate saliva flow. Patients need assurance regarding this acclimation process. Insufficient saliva or xerostomia presents more serious(serous!) problems. Moisture is necessary for adhesion, cohesion and capillary action and when salva is deficient or absent, problems ensue.Xerostomia also causes the cheeks and lips to stick to the denture base in an uncomfortable manner. Petroleum jelly applied over cameo surface can be helpful.
J Am Geriatr Soc. 2002 Mar;50(3):535-43. Links
Xerostomia and the geriatric patient.
Ship JA, Pillemer SR, Baum BJ.
Department of Oral Medicine, Bluestone Center for Clinical Research, New York University College of Dentistry, 345 East 24th Street, New York, NY 10010, USA. jonathan.ship@nyu.edu
Saliva is essential for the preservation of oral-pharyngeal health, and disorders of salivary physiology are associated with numerous oral and pharyngeal problems, particularly in older people. Although salivary function is remarkably intact in healthy aging, medical problems, medications, and head and neck radiotherapy can cause salivary dysfunction and complaints of xerostomia among older people. Sjögren's syndrome, an autoimmune exocrinopathy, is the most common medical disease associated with salivary dysfunction. Medications with anticholinergic side effects will impair salivary output, and head and neck radiotherapy for cancer will cause permanent destruction of salivary glands. Treatments for salivary problems are based upon establishing a diagnosis, protecting oral and pharyngeal health, stimulating remaining glands, and replacing lost salivary fluids.
Complaints of a dry, sore or "burning mouth" are common among the elderly, especially women -- sometimes due to the many medications taken. The incidence of xerostomia, to give dry mouth its medical name, is unknown. In recent surveys, 45-60 per cent of the elderly in institutions and 20 per cent of seniors at home complained of occasional xerostomia. Dry mouth can be a mere annoyance, but besides the discomfort it can also cause pain when eating and talking, and may lead to dental decay, periodontal (gum) and denture problems and an increase in fungal (yeast) infections. The condition should never be ignored. Good oral hygiene and brushing teeth three times daily, are a must. Smoking and excess alcohol consumption aggravate the disorder.
#8 Sj?ren’s Syndrome: This autoimmune disorder affects as many as one million persons in the U.S., with a 17:1 to 18:1 ratio of women to men affected.2,3 It is more likely to occur after age 50. Normal exocrine gland structures are displaced through lymphocytic infiltration. This destruction gradually renders the patient’s salivary and lacrimal glands useless. If manifestations are limited to these sites, the condition is termed primary Sj?ren’s syndrome. If it occurs in conjunction with other autoimmune diseases (e.g., systemic lupus erythematosus, rheumatoid arthritis, scleroderma, fibromyositis), it is known as secondary Sj?ren’s syndrome.4-6 There is no cure for Sj?ren’s; therapy is supportive.
Diabetes Mellitus: Although the results are by no means conclusive, some research has shown that patients with diabetes mellitus experience decreases in salivary flow rates. In addition, glucose levels in saliva rise and fall in concert with blood levels. Because patients with diabetes often experience hyperglycemia, higher than normal levels of glucose facilitate the growth of intraoral organisms.7
Medications: Xerostomia is one of the more common adverse effects of medications. Xerogenic medication classes include antidepressants, antipsychotics, anti-
histamine/decongestant combinations, gastrointestinals, anti-Parkinson agents, anticholinergics, urinary antispasmodics, diuretics, systemic bronchodilators, and beta-blockers.8 Specific medications that can cause xerostomia include methyldopa, clonidine, disopyramide, reserpine, and guanabenz. Use of certain nonprescription products—e.g., those that contain codeine (Schedule V cough preparations), ephedrine or epinephrine (asthma products), and antihistamines and/or decongestants (products for common cold/allergic rhinitis, menstrual symptoms, motion sickness and sleep aids)—also may result in xerostomia. Unfortunately, the medications most commonly used by the elderly are xerogenic.9
Aging: With aging, the salivary systems become less resistant to insult.10 This may be partly because cells that secrete saliva are gradually replaced by fibrous and adipose tissues.9 Consequently, salivary output can be reduced by as much as 30%?0%.
Further, the increased prevalence of chronic medical conditions with aging leads to a concomitant increase in the number of medications taken. Because of these factors, approximately 25% of the elderly suffer from xerostomia.11
Radiotherapy: As many as 50,000 new cases of head and neck cancers are diagnosed yearly.12 Radiotherapy remains one of the primary treatment modalities for these cancers, also serving as an adjunct to surgery. Unfortunately, it is difficult to irradiate tumors of the head and neck without also exposing the salivary glands.13
The rapidly proliferating cells of these sites are extremely vulnerable to radiation damage, which may reduce their output by as much as 90%. When some saliva remains, its pH is often decreased, and its viscosity increases. Some patients regain normal salivary cell function within 12?8 months after therapy is discontinued, but others may never recover preradiation salivary flow levels.
Sequelae
Xerostomia is the source of both minor and serious problems. For instance, in order to be swallowed easily, food must be softened by mastication (augmented by saliva). If food has not been sufficiently softened, the resultant difficulty swallowing may discourage patients from eating. Also, in order to taste (or smell) food, patients must be able to adequately solubilize portions of the food in saliva.4 Thus, a reduced or absent sensation of taste or smell may be due to xerostomia.
Difficulty in using oral appliances may result from dry mouth. This would be most evident in patients with dentures. Saliva is critical in maintaining the placement of dentures. A thin film of saliva lies between the dentures and alveolar bone; its viscosity helps prevent the denture from losing tight contact with the mandibular and/or maxillary bones. Therefore, xerostomia compromises the ability of the denture wearer to talk and masticate. He or she may also suffer lesions beneath the dentures as a result of xerostomia.11 If the lesions are severe, patients cannot wear the dentures, further compromising mastication and subsequent nutritional status.
When intraoral tissues become desiccated, the patient often experiences intraoral burning.4 This uncomfortable sensation can, in turn, inhibit eating and swallowing. The burning may, in fact, be an early manifestation of oral candidiasis, especially when the mucosa is fissured, erythematous, and has a macular appearance in areas over hard palate.
However, one of the most devastating effects of xerostomia concerns the effects on teeth. Saliva is a buffering substance whose pH is higher than that of the acids produced by oral microflora. It contains calcium phosphate, which aids in remineralization of dental enamel. Saliva also contains amylase, which helps break down food remaining in the oral cavity after a meal.11 It also prevents caries through the mechanical flushing of food from tooth surfaces. The absence of saliva compromises remineralization, allows cariogenic substances to remain in the mouth for longer periods, and contributes to a sustained low intraoral pH. A shift to more dangerous cariogenic bacterial microflora grad-ually occurs. The net effect of all these factors is the rapid and widespread onset of caries. Caries due to xerostomia affect the roots and crown of virtually all teeth.14 In the worst case, immediate care may be unable to save the teeth, usually necessitating full dentures.
Advising Patients with Xerostomia
Pharmacists can counsel on several points. This month’s patient information page focuses on dietary advice, suggesting that patients eat easily ingested foods. However, the pharmacist should caution patients not to rely solely on fried or fatty foods because doing so can cause them to exceed the recommendations for maximum dietary intake of fat and cholesterol.4
Patients with their natural teeth should be urged to adopt strict oral hygiene regimens, including flossing, careful and thorough brushing, and the use of a periodontal cleansing aid. Frequent dental appointments must be made to institute such measures as topical fluoride applications and pit and fissure sealants.
Patients with residual salivary function can be advised to stimulate flow using sugarless chewing gum or candy.15 Oral pilocarpine (Salagen) is also effective in some cases. Further, the value of attaining excellent overall body hydration through ingestion of adequate water every day is often overlooked.
Patients who experience complete lack of salivary function may be able to cope only by using saliva substitutes. These nonprescription products are water-based and include useful molecules, such as cellulose derivatives, to increase contact time with mucosa. TABLE 1 lists examples of saliva substitutes. Product labels direct patients to spray or apply as often as needed to ensure adequate oral moisture.
Patients also may be taught that certain habits, such as smoking, mouth-breathing and intake of caffeine-containing beverages, increase the risk of xerostomia.4 Decreasing or ceasing these practices, if possible, should have some impact on dry mouth.
What to do about dry mouthDry mouth is a common condition that has several causes, including aging, medications, radiation therapy for cancers of the head or neck, and
serious medical disorders, such as Sj?ren’s syndrome. If Sj?ren’s syndrome is the cause of your dry mouth, you may also experience dry eye, rheumatoid arthritis, and kidney disease. Thus, therapy will involve much more than dry mouth remedies. For this reason, it is a good idea to visit a doctor to be sure that your dry mouth is not a symptom
of another disease. A physician can check the overall state of your oral fluid production and can rule out any serious conditions.Dry Mouth Problems: Even when dry mouth is not due to a serious medical problem, it can be quite
a nuisance. Lack of saliva may result in problems with chewing, swallowing, talking, singing, and other normal activities. The insides of your cheeks may become sticky, so much so that they are difficult to move away from the outer surfaces of the teeth. If oral dryness continues long enough, you may also start getting a lot of cavities. This is because saliva helps prevent bacterial acids from dissolving tooth enamel. Bacteria may even gain access to the areas under fillings, so that restored teeth develop severe problems. In the worst case, longstanding dry mouth may result in loss of so many teeth that dentures become necessary. For these reasons, it is a good idea not to neglect dry mouth.
Managing Dry Mouth: There are several methods to deal with dry mouth. If you still have at least some salivary flow, sucking on sugarless candy or chewing sugarless gum will help stimulate the
salivary glands.
If these methods do not work, or if you have a total lack of salivary flow (perhaps caused by radiation therapy), you may need to use a saliva substitute. For advice about these products, consult your pharmacist. He or she can demonstrate their use, provide a choice of several dosage forms (such as gel, spray, or rinse), and can tell you more about dry mouth.
You can also institute several commonsense steps to make it easier to live with dry mouth. Your food choices can help you cope. Choosing foods that are prepared in a more liquid form can help. For instance, the moisture in mashed potatoes makes them easier to eat than potato chips, which are drier. Also, corn from the cob contains more moisture than dry popcorn. Some foods, such as crackers and biscuits, may simply be too dry to eat without taking frequent sips of water between bites.
Try not to take over-the-counter products that dry the mouth. Antihistamines are one of the most common groups of medications that can result in dry mouth. They are commonly found in allergy products and cold remedies. Ingredients you should watch out for include chlorpheniramine, doxylamine, dexbrompheniramine, triprolidine, brompheniramine, diphenhydramine, pyrilamine and phenindamine.
Age Ageing. 1998 Mar;27(2):123-8. Links
Xerostomia is a subjective complaint associated with salivary gland hypofunction.1 However, the symptom of dry mouth can occur without an actual reduction in salivary flow. Etiologies of xerostomia include both salivary and nonsalivary causes.2 Identifying those with true salivary hypofunction is key due to the risk of oral disease. A thorough review of systems and medication history is essential to determining the origin of xerostomia symptoms.2
Medications
More than 500 drugs are reported to cause xerostomia as a side effect, and medication use is the most frequent cause of xerostomia complaints, especially among the elderly.3,4 The severity of the xerostomia complaint often increases among the elderly due to a synergistic effect when taking multiple medications.3,5 Both stimulated and unstimulated salivary flow rates decrease with an increasing number of medications taken.6 The most common cause of drug-induced xerostomia is the altering of neural pathways that stimulate salivary gland secretion.7 These are drugs that have either an anticholinergic or sympathomimetic effect.4 Stimulation of the parasympathetic nerves (cholinergic action) produces an increase in fluid volume (serous saliva). Stimulation by the sympathetic nerves (sympathomimetic action) produces less volume and viscous saliva.4,8 Thus, drugs that have an anticholinergic action reduce the volume of serous saliva, including antihypertensives, antihistamines, antidepressants, antipsychotics, antiemetics, antispasmotics, and anti-parkinsonian drugs.3,4,7 Drugs with sympathomimetic actions produce a more viscous, mucinous saliva with less volume, such as decongestants, bronchodilators, appetite suppressants, and amphetamines.4 Drugs may also exert their neural effects in the higher centers of the brain; stimulation of certain adrenoreceptors in the frontal cortex can produce inhibitory effects on salivary nuclei.3 Drugs can also produce xerostomia without affecting the neural pathways. Inhaled medications produce the sensation of dryness but without any change in salivary flow.3 Interestingly, some anti-hypertensive medications produce the symptoms of xerostomia without actually decreasing salivary flow.9 How antihypertensive medications actually cause xerostomia is unknown, although it is hypothesized that xerostomia may result from decreased fluid volume and loss of electrolytes secondary to increased urination and dehydration.9 Diuretics produce alterations in electrolyte and fluid balance.3,7 Finally, drugs can also decrease salivary flow by causing vasoconstriction in the salivary glands.3
The list of medications associated with xerostomia continues to grow as new drugs are released. Other drug classes now known to cause xerostomia include the proton pump inhibitors, protease inhibitors and reverse transcriptase inhibitors for HIV infection, analgesics and narcotics for pain control, a variety of anti-infective agents, and some anti-neoplastic agents.4,7 Table 1 lists the drug classes that cause xerostomia. Dental professionals can work with their patients' physicians to address chronic dryness. When possible, the patient may be taken off a medication or switched to another that is less xerogenic. The dosing regimen can be altered so that peak plasma levels of the drug do not correspond with periods of maximum dryness, such as nighttime. Dosages can be split into smaller quantities and ingested more frequently to allow for natural periods of salivary stimulation, eg, eating, to counteract the drying effects of the drugs.3
Diseases of the Salivary Glands
Sjögren's syndrome (SS) is an autoimmune disorder characterized by intense lymphocytic infiltration of the exocrine glands. This infiltration destroys much of the glandular structure, making it difficult to produce fluids for normal function. Common symptoms include chronic dry eyes and dry mouth. There are two forms of the disease: primary SS not associated with any other autoimmune disease and secondary SS associated with other connective tissue diseases, including rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.4 International diagnostic criteria are published to assist with the diagnosis of the disease, which among others include measures of salivary gland inflammation, and the presence of specific autoantibodies in the serum.10 Biopsy of the labial minor salivary glands demonstrates a characteristic focal lymphocytic infiltration.11 Glandular swelling is characteristic of SS. However, persistent swelling of the parotid glands also may indicate bacterial infection or lymphoma.12 Lymphocytic invasion, causing local salivary tissue inflammation and fibrosis, combined with the autoimmune-mediated interference with neurotransmitter and receptor function appear to be responsible for the clinical manifestations of SS.12 Interestingly, labial salivary gland biopsies taken from patients with severe oral and ocular dryness reveal that as many as 50% of their glandular cells remain intact.13 This allows patients with SS to benefit from salivary stimulating medications.
Chronic salivary gland enlargement and xerostomia are also symptoms of sarcoidosis, HIV disease, and hepatitis C viral infection (HCV).4 HIV salivary gland disease occurs in up to 8% of infected individuals and most frequently affects the parotid glands with bilateral enlargement and xerostomia. It usually arises late in the course of HIV infection but occasionally may be the first manifestation of HIV disease. Kaposi's sarcoma and nonHodgkin's lymphoma associated with HIV infection may also cause salivary gland enlargement.4 Medications used to treat HIV disease also produce xerostomia.4 HCV salivary gland disease affects up to 33% of affected persons, with xerostomia as the predominant symptom.4 Histologically, the salivary gland changes with this disease resemble those seen with SS but with a lesser degree of inflammation. Other diseases that are associated with xerostomia include amyloidosis, cystic fibrosis, autoimmune thyroiditis, rheumatoid arthritis, chronic graft-versus-host disease, and diabetes.4,13-16 Medication use, elevated glycosylated hemoglobin levels, and elevated fasting blood glucose levels are identified as factors leading to dehydration and xerostomia in Type I diabetics.16
Table 1. Drug classes associated with causing xerostomia. Anorexiants
Antiacne Agents
Antianxiety Agents
Anticholinergics/Antispasmotics
Anticonvulsants
Antidepressants
Antidiarrheals
Antiemetics
Antihistamines
Antihypertensives
Anti-inflammatory Analgesics
Antinauseants
Antiparkinsonian Agents
Antipsychotics
Bronchodilators
Decongestants
Diuretics
Muscle Relaxants
Narcotic Analgesics
SedativesSource: USP DI® Drug Information for the Healthcare Professional. 24th ed. Englewood, Colo: Micromedix, Inc; 2004. Cancer Therapies
Salivary glandular tissues are highly sensitive to the radiation therapy used to treat oral carcinomas, and serous acinar cells found in the parotids are more radiosensitive than the mucous cell types.4,8 Serous cells may contain more heavy metals that absorb radiation energy, which promotes the release and action of free radicals.8 Amifostine is a chemoprotective drug used to reduce the incidence of moderate to severe xerostomia in patients undergoing radiation therapy that includes a significant portion of the parotid glands. The drug acts as a scavenger of free radicals found in the tissues.17
The degree of xerostomia is associated with the dose of radiation and the amount of salivary tissue affected. Whenever possible, a portion of the parotid gland should be spared from the radiation field. After 5 weeks of radiation, salivary flow is greatly reduced and rarely recovers completely.4,8 Patients may experience some recovery from radiation damage within the first year after treatment.8 Salivary flow from the contralateral glands may increase to compensate for radiation damage, although the recovery of the less radiosensitive mucous glands appears to be important for residual lubrication.8 After radiation, the saliva becomes more viscous and changes to a yellowish-brown color. Salivary buffering capacity is reduced, resulting in an acidic oral pH, compromised antimicrobial activities, and increased incidence of oral diseases.
Chemotherapy causes changes in salivary flow rates and composition during treatment, and the effects vary with the types of agents used and the duration of treatment.8 Chemotherapy causes systemic immunosuppression that alters the concentration of salivary immunoglobulins, resulting in oral mucositis, progression of gingival disease, caries, and opportunistic infections.8 A number of antineoplastic drugs cause xerostomia and the degree of xerostomia is related to the total number of chemotherapeutic agents used.4 The exact mechanisms by which these drugs damage salivary and other oral tissues are unknown. However, increased salivary drug concentration and prolonged contact of the drug-containing saliva with the oral epithelium is observed in patients with low flow rates. A high concentration of a biologically active drug may result in increased toxicity to oral tissues.8 Amifostine is also used to detoxify the reactive metabolites of cisplatin, a drug used to treat many cancers, including advanced ovarian, lung, and some head and neck cancers.4,8,17
Salivary Stimulation & Replacement Therapies
Salivary stimulation can be achieved mechanically by chewing sugarless gum and by chemical (gustatory) stimulation by sucking on sugarless candies or products that contain citric acid, such as vitamin C tablets, lemon drops, or lozenges.18 Caution must be used with citric acid due to its acidity. Sonic toothbrushing may also increase salivary flow in patients with SS.19
Artificial salivary substitutes can be recommended. They do provide short-term relief, however, compliance may be poor. Most products in this category contain sodium carboxymethylcellulose, which mimics the viscosity of natural saliva. Water-based moisturizing gels can be used intraorally as a saliva substitute and extraorally on the lips to provide 8 hours of relief from xerostomia symptoms.
Two prescription drugs have been approved by the Food and Drug Administration for the treatment of xerostomia: pilocarpine and cevimeline. These drugs are cholinergic agonists that produce parasympathetic stimulation of the exocrine glands to increase serous secretions. Pilocarpine is approved for use in both head and neck radiation therapy patients and patients with SS; cevimeline is approved for SS. Because these are systemic medications, they turn on secretions from all exocrine glands-an advantage for relieving multiple symptoms of SS. However, patients may experience adverse events related to their cholinergic effects, most notably excessive sweating. These drugs must be used with caution in patients with cardiovascular disease, chronic respiratory conditions, and kidney disease. Use of these medications is contraindicated in patients with narrow-angle glaucoma, uncontrolled asthma and liver disease. These are common disorders among the elderly who frequently present with xerostomia. Several clinical trials have demonstrated their efficacy in relieving xerostomia symptoms and increasing salivary flow in radiation therapy and SS patients.20
Current research is investigating the use of other medication classes that may relieve dry mouth symptoms, as well as biogenetic engineering technology to regenerate damaged tissues, and salivary transplantation.4,20 These discoveries will undoubtedly improve the oral health and quality of life of patients suffering from this chronic condition.
From Dimensions of Dental Hygiene. July 2005;3(7):22-24.
Associations between malnutrition, poor general health and oral dryness in hospitalized elderly patients.
Dormenval V, Budtz-Jørgensen E, Mojon P, Bruyère A, Rapin CH.
Department of Gerodontology and Removable Prosthodontics, University of Geneva, 19 rue Barthelemy-Menn, CH- 1205 Geneva, Switzerland.
OBJECTIVE: To obtain information about the possible relationship between symptoms and signs of oral dryness and malnutrition/poor general health in hospitalized older people. DESIGN: A cross-sectional clinical investigation with measurements of unstimulated salivary flow rates (USFR), stimulated salivary flow rates (SSFR), nutritional status, serum albumin concentration and an evaluation of symptoms of oral dryness and loss of appetite by a questionnaire. SUBJECTS AND METHODS: A cohort of 99 elderly, non-psychiatric patients hospitalized for medical reasons; collection of demographic and health data from medical files, collection of USFR and SSFR, measurements of body mass index (BMI), lean body mass, fat body mass, serum album in concentration; completion of a questionnaire related to symptoms of oral dryness and the patients' appreciation of their nutritional status. MAIN OUTCOME MEASURES: SSFR and USFR. RESULTS: Mean age of the 99 patients was 82.5 +/- 4.0 years. Anthropometric examinations indicated malnutrition of severe or intermediate degree in about 50% while 46% showed moderately and 40% severely reduced albumin. Loss of appetite was present in 54% and 51% complained of oral dryness; 17% had an USFR <0.1 ml/min and 26% a SSFR <0.5 ml/min. Significant associations were found between (i) reduced salivary flow rate, malnutrition and reduced serum albumin concentration, (ii) recent loss of appetite and low serum album in concentration and (iii)complaints of oral dryness and reduced salivary flow rates. There were also significant associations between complaints of oral dryness, loss of appetite and low BMI. CONCLUSION: Reduced salivary secretion and complaints of oral dryness could be signs of poor nutritional or general health status of elderly patients. Reduced salivary secretion and feeling of oral dryness could have a negative effect on alimentation, appetite and oral comfort.
PMID: 16296671 [PubMed - indexed for MEDLINE]
Impact of dry mouth on oral symptoms and function in removable denture wearers in Japan.
Ikebe K, Morii K, Kashiwagi J, Nokubi T, Ettinger RL.
Division of Oromaxillofacial Regeneration, Osaka University Graduate School of Dentistry, Suita, Japan. ikebe@dent.osaka-u.ac.jp
OBJECTIVE: The purpose of this study was to determine the association of dry mouth with oral symptoms and function, such as denture instability, discomfort, soreness in denture-bearing tissue, and dissatisfaction with chewing, tasting, or speaking in removable denture wearers. STUDY DESIGN: The subjects were 493 removable denture wearers with a mean age of 67.3 years. Perception of oral dryness was measured by a questionnaire. A multiple logistic regression analysis was used to determine the effect of the dry mouth on oral symptoms and function after controlling for age and gender. RESULTS: Oral dryness during eating was related to dissatisfaction with chewing (odds ratio, 10.5; P < .001) and speaking (odds ratio, 3.5; P < .05) and overall dissatisfaction (odds ratio, 6.3; P < .01) in complete denture wearers. Feeling of dry mouth was likely to be associated with soreness in denture-bearing tissues in both complete and removable partial denture wearers. CONCLUSIONS: There was a significant association of the perception of dry mouth among a group of denture wearers with oral symptoms and function.
#9
Patients tend to think of dry mouth as a medical condition in and of itself. Although dry mouth may be an isolated clinical entity, more often it reflects underlying pathology. Depression, uncontrolled hypertension, Alzheimer’s disease, Addison’s disease, alcoholic cirrhosis, hyperlipidemia, generalized dehydration, and salivary gland infection all can produce xerosto-mia. Xerostomia also may be part of Sj?ren’s syndrome or diabetes mellitus, a result of xerogenic medications, or a side effect of radiation therapy.
Sj?ren’s Syndrome: This autoimmune disorder affects as many as one million persons in the U.S., with a 17:1 to 18:1 ratio of women to men affected.2,3 It is more likely to occur after age 50. Normal exocrine gland structures are displaced through lymphocytic infiltration. This destruction gradually renders the patient’s salivary and lacrimal glands useless. If manifestations are limited to these sites, the condition is termed primary Sj?ren’s syndrome. If it occurs in conjunction with other autoimmune diseases (e.g., systemic lupus erythematosus, rheumatoid arthritis, scleroderma, fibromyositis), it is known as secondary Sj?ren’s syndrome.4-6 There is no cure for Sj?ren’s; therapy is supportive.
Diabetes Mellitus: Although the results are by no means conclusive, some research has shown that patients with diabetes mellitus experience decreases in salivary flow rates. In addition, glucose levels in saliva rise and fall in concert with blood levels. Because patients with diabetes often experience hyperglycemia, higher than normal levels of glucose facilitate the growth of intraoral organisms.7
Medications: Xerostomia is one of the more common adverse effects of medications. Xerogenic medication classes include antidepressants, antipsychotics, anti-
histamine/decongestant combinations, gastrointestinals, anti-Parkinson agents, anticholinergics, urinary antispasmodics, diuretics, systemic bronchodilators, and beta-blockers.8 Specific medications that can cause xerostomia include methyldopa, clonidine, disopyramide, reserpine, and guanabenz. Use of certain nonprescription products—e.g., those that contain codeine (Schedule V cough preparations), ephedrine or epinephrine (asthma products), and antihistamines and/or decongestants (products for common cold/allergic rhinitis, menstrual symptoms, motion sickness and sleep aids)—also may result in xerostomia. Unfortunately, the medications most commonly used by the elderly are xerogenic.9
Aging: With aging, the salivary systems become less resistant to insult.10 This may be partly because cells that secrete saliva are gradually replaced by fibrous and adipose tissues.9 Consequently, salivary output can be reduced by as much as 30%?0%.
Further, the increased prevalence of chronic medical conditions with aging leads to a concomitant increase in the number of medications taken. Because of these factors, approximately 25% of the elderly suffer from xerostomia.11
Radiotherapy: As many as 50,000 new cases of head and neck cancers are diagnosed yearly.12 Radiotherapy remains one of the primary treatment modalities for these cancers, also serving as an adjunct to surgery. Unfortunately, it is difficult to irradiate tumors of the head and neck without also exposing the salivary glands.13
The rapidly proliferating cells of these sites are extremely vulnerable to radiation damage, which may reduce their output by as much as 90%. When some saliva remains, its pH is often decreased, and its viscosity increases. Some patients regain normal salivary cell function within 12?8 months after therapy is discontinued, but others may never recover preradiation salivary flow levels.
Sequelae
Xerostomia is the source of both minor and serious problems. For instance, in order to be swallowed easily, food must be softened by mastication (augmented by saliva). If food has not been sufficiently softened, the resultant difficulty swallowing may discourage patients from eating. Also, in order to taste (or smell) food, patients must be able to adequately solubilize portions of the food in saliva.4 Thus, a reduced or absent sensation of taste or smell may be due to xerostomia.
Difficulty in using oral appliances may result from dry mouth. This would be most evident in patients with dentures. Saliva is critical in maintaining the placement of dentures. A thin film of saliva lies between the dentures and alveolar bone; its viscosity helps prevent the denture from losing tight contact with the mandibular and/or maxillary bones. Therefore, xerostomia compromises the ability of the denture wearer to talk and masticate. He or she may also suffer lesions beneath the dentures as a result of xerostomia.11 If the lesions are severe, patients cannot wear the dentures, further compromising mastication and subsequent nutritional status.
When intraoral tissues become desiccated, the patient often experiences intraoral burning.4 This uncomfortable sensation can, in turn, inhibit eating and swallowing. The burning may, in fact, be an early manifestation of oral candidiasis, especially when the mucosa is fissured, erythematous, and has a macular appearance in areas over hard palate.
However, one of the most devastating effects of xerostomia concerns the effects on teeth. Saliva is a buffering substance whose pH is higher than that of the acids produced by oral microflora. It contains calcium phosphate, which aids in remineralization of dental enamel. Saliva also contains amylase, which helps break down food remaining in the oral cavity after a meal.11 It also prevents caries through the mechanical flushing of food from tooth surfaces. The absence of saliva compromises remineralization, allows cariogenic substances to remain in the mouth for longer periods, and contributes to a sustained low intraoral pH. A shift to more dangerous cariogenic bacterial microflora grad-ually occurs. The net effect of all these factors is the rapid and widespread onset of caries. Caries due to xerostomia affect the roots and crown of virtually all teeth.14 In the worst case, immediate care may be unable to save the teeth, usually necessitating full dentures.
Advising Patients with Xerostomia
Pharmacists can counsel on several points. This month’s patient information page focuses on dietary advice, suggesting that patients eat easily ingested foods. However, the pharmacist should caution patients not to rely solely on fried or fatty foods because doing so can cause them to exceed the recommendations for maximum dietary intake of fat and cholesterol.4
Patients with their natural teeth should be urged to adopt strict oral hygiene regimens, including flossing, careful and thorough brushing, and the use of a periodontal cleansing aid. Frequent dental appointments must be made to institute such measures as topical fluoride applications and pit and fissure sealants.
Patients with residual salivary function can be advised to stimulate flow using sugarless chewing gum or candy.15 Oral pilocarpine (Salagen) is also effective in some cases. Further, the value of attaining excellent overall body hydration through ingestion of adequate water every day is often overlooked.
Patients who experience complete lack of salivary function may be able to cope only by using saliva substitutes. These nonprescription products are water-based and include useful molecules, such as cellulose derivatives, to increase contact time with mucosa. TABLE 1 lists examples of saliva substitutes. Product labels direct patients to spray or apply as often as needed to ensure adequate oral moisture.
Patients also may be taught that certain habits, such as smoking, mouth-breathing and intake of caffeine-containing beverages, increase the risk of xerostomia.4 Decreasing or ceasing these practices, if possible, should have some impact on dry mouth.
What to do about dry mouthDry mouth is a common condition that has several causes, including aging, medications, radiation therapy for cancers of the head or neck, and
serious medical disorders, such as Sj?ren’s syndrome. If Sj?ren’s syndrome is the cause of your dry mouth, you may also experience dry eye, rheumatoid arthritis, and kidney disease. Thus, therapy will involve much more than dry mouth remedies. For this reason, it is a good idea to visit a doctor to be sure that your dry mouth is not a symptom
of another disease. A physician can check the overall state of your oral fluid production and can rule out any serious conditions.Dry Mouth Problems: Even when dry mouth is not due to a serious medical problem, it can be quite
a nuisance. Lack of saliva may result in problems with chewing, swallowing, talking, singing, and other normal activities. The insides of your cheeks may become sticky, so much so that they are difficult to move away from the outer surfaces of the teeth. If oral dryness continues long enough, you may also start getting a lot of cavities. This is because saliva helps prevent bacterial acids from dissolving tooth enamel. Bacteria may even gain access to the areas under fillings, so that restored teeth develop severe problems. In the worst case, longstanding dry mouth may result in loss of so many teeth that dentures become necessary. For these reasons, it is a good idea not to neglect dry mouth.
Managing Dry Mouth: There are several methods to deal with dry mouth. If you still have at least some salivary flow, sucking on sugarless candy or chewing sugarless gum will help stimulate the
salivary glands.
If these methods do not work, or if you have a total lack of salivary flow (perhaps caused by radiation therapy), you may need to use a saliva substitute. For advice about these products, consult your pharmacist. He or she can demonstrate their use, provide a choice of several dosage forms (such as gel, spray, or rinse), and can tell you more about dry mouth.
You can also institute several commonsense steps to make it easier to live with dry mouth. Your food choices can help you cope. Choosing foods that are prepared in a more liquid form can help. For instance, the moisture in mashed potatoes makes them easier to eat than potato chips, which are drier. Also, corn from the cob contains more moisture than dry popcorn. Some foods, such as crackers and biscuits, may simply be too dry to eat without taking frequent sips of water between bites.
Try not to take over-the-counter products that dry the mouth. Antihistamines are one of the most common groups of medications that can result in dry mouth. They are commonly found in allergy products and cold remedies. Ingredients you should watch out for include chlorpheniramine, doxylamine, dexbrompheniramine, triprolidine, brompheniramine, diphenhydramine, pyrilamine and phenindamine.
Age Ageing. 1998 Mar;27(2):123-8. Links
Xerostomia is a subjective complaint associated with salivary gland hypofunction.1 However, the symptom of dry mouth can occur without an actual reduction in salivary flow. Etiologies of xerostomia include both salivary and nonsalivary causes.2 Identifying those with true salivary hypofunction is key due to the risk of oral disease. A thorough review of systems and medication history is essential to determining the origin of xerostomia symptoms.2
Medications
More than 500 drugs are reported to cause xerostomia as a side effect, and medication use is the most frequent cause of xerostomia complaints, especially among the elderly.3,4 The severity of the xerostomia complaint often increases among the elderly due to a synergistic effect when taking multiple medications.3,5 Both stimulated and unstimulated salivary flow rates decrease with an increasing number of medications taken.6 The most common cause of drug-induced xerostomia is the altering of neural pathways that stimulate salivary gland secretion.7 These are drugs that have either an anticholinergic or sympathomimetic effect.4 Stimulation of the parasympathetic nerves (cholinergic action) produces an increase in fluid volume (serous saliva). Stimulation by the sympathetic nerves (sympathomimetic action) produces less volume and viscous saliva.4,8 Thus, drugs that have an anticholinergic action reduce the volume of serous saliva, including antihypertensives, antihistamines, antidepressants, antipsychotics, antiemetics, antispasmotics, and anti-parkinsonian drugs.3,4,7 Drugs with sympathomimetic actions produce a more viscous, mucinous saliva with less volume, such as decongestants, bronchodilators, appetite suppressants, and amphetamines.4 Drugs may also exert their neural effects in the higher centers of the brain; stimulation of certain adrenoreceptors in the frontal cortex can produce inhibitory effects on salivary nuclei.3 Drugs can also produce xerostomia without affecting the neural pathways. Inhaled medications produce the sensation of dryness but without any change in salivary flow.3 Interestingly, some anti-hypertensive medications produce the symptoms of xerostomia without actually decreasing salivary flow.9 How antihypertensive medications actually cause xerostomia is unknown, although it is hypothesized that xerostomia may result from decreased fluid volume and loss of electrolytes secondary to increased urination and dehydration.9 Diuretics produce alterations in electrolyte and fluid balance.3,7 Finally, drugs can also decrease salivary flow by causing vasoconstriction in the salivary glands.3
The list of medications associated with xerostomia continues to grow as new drugs are released. Other drug classes now known to cause xerostomia include the proton pump inhibitors, protease inhibitors and reverse transcriptase inhibitors for HIV infection, analgesics and narcotics for pain control, a variety of anti-infective agents, and some anti-neoplastic agents.4,7 Table 1 lists the drug classes that cause xerostomia. Dental professionals can work with their patients' physicians to address chronic dryness. When possible, the patient may be taken off a medication or switched to another that is less xerogenic. The dosing regimen can be altered so that peak plasma levels of the drug do not correspond with periods of maximum dryness, such as nighttime. Dosages can be split into smaller quantities and ingested more frequently to allow for natural periods of salivary stimulation, eg, eating, to counteract the drying effects of the drugs.3
Diseases of the Salivary Glands
Sjögren's syndrome (SS) is an autoimmune disorder characterized by intense lymphocytic infiltration of the exocrine glands. This infiltration destroys much of the glandular structure, making it difficult to produce fluids for normal function. Common symptoms include chronic dry eyes and dry mouth. There are two forms of the disease: primary SS not associated with any other autoimmune disease and secondary SS associated with other connective tissue diseases, including rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.4 International diagnostic criteria are published to assist with the diagnosis of the disease, which among others include measures of salivary gland inflammation, and the presence of specific autoantibodies in the serum.10 Biopsy of the labial minor salivary glands demonstrates a characteristic focal lymphocytic infiltration.11 Glandular swelling is characteristic of SS. However, persistent swelling of the parotid glands also may indicate bacterial infection or lymphoma.12 Lymphocytic invasion, causing local salivary tissue inflammation and fibrosis, combined with the autoimmune-mediated interference with neurotransmitter and receptor function appear to be responsible for the clinical manifestations of SS.12 Interestingly, labial salivary gland biopsies taken from patients with severe oral and ocular dryness reveal that as many as 50% of their glandular cells remain intact.13 This allows patients with SS to benefit from salivary stimulating medications.
Chronic salivary gland enlargement and xerostomia are also symptoms of sarcoidosis, HIV disease, and hepatitis C viral infection (HCV).4 HIV salivary gland disease occurs in up to 8% of infected individuals and most frequently affects the parotid glands with bilateral enlargement and xerostomia. It usually arises late in the course of HIV infection but occasionally may be the first manifestation of HIV disease. Kaposi's sarcoma and nonHodgkin's lymphoma associated with HIV infection may also cause salivary gland enlargement.4 Medications used to treat HIV disease also produce xerostomia.4 HCV salivary gland disease affects up to 33% of affected persons, with xerostomia as the predominant symptom.4 Histologically, the salivary gland changes with this disease resemble those seen with SS but with a lesser degree of inflammation. Other diseases that are associated with xerostomia include amyloidosis, cystic fibrosis, autoimmune thyroiditis, rheumatoid arthritis, chronic graft-versus-host disease, and diabetes.4,13-16 Medication use, elevated glycosylated hemoglobin levels, and elevated fasting blood glucose levels are identified as factors leading to dehydration and xerostomia in Type I diabetics.16
Table 1. Drug classes associated with causing xerostomia. Anorexiants
Antiacne Agents
Antianxiety Agents
Anticholinergics/Antispasmotics
Anticonvulsants
Antidepressants
Antidiarrheals
Antiemetics
Antihistamines
Antihypertensives
Anti-inflammatory Analgesics
Antinauseants
Antiparkinsonian Agents
Antipsychotics
Bronchodilators
Decongestants
Diuretics
Muscle Relaxants
Narcotic Analgesics
SedativesSource: USP DI® Drug Information for the Healthcare Professional. 24th ed. Englewood, Colo: Micromedix, Inc; 2004. Cancer Therapies
Salivary glandular tissues are highly sensitive to the radiation therapy used to treat oral carcinomas, and serous acinar cells found in the parotids are more radiosensitive than the mucous cell types.4,8 Serous cells may contain more heavy metals that absorb radiation energy, which promotes the release and action of free radicals.8 Amifostine is a chemoprotective drug used to reduce the incidence of moderate to severe xerostomia in patients undergoing radiation therapy that includes a significant portion of the parotid glands. The drug acts as a scavenger of free radicals found in the tissues.17
The degree of xerostomia is associated with the dose of radiation and the amount of salivary tissue affected. Whenever possible, a portion of the parotid gland should be spared from the radiation field. After 5 weeks of radiation, salivary flow is greatly reduced and rarely recovers completely.4,8 Patients may experience some recovery from radiation damage within the first year after treatment.8 Salivary flow from the contralateral glands may increase to compensate for radiation damage, although the recovery of the less radiosensitive mucous glands appears to be important for residual lubrication.8 After radiation, the saliva becomes more viscous and changes to a yellowish-brown color. Salivary buffering capacity is reduced, resulting in an acidic oral pH, compromised antimicrobial activities, and increased incidence of oral diseases.
Chemotherapy causes changes in salivary flow rates and composition during treatment, and the effects vary with the types of agents used and the duration of treatment.8 Chemotherapy causes systemic immunosuppression that alters the concentration of salivary immunoglobulins, resulting in oral mucositis, progression of gingival disease, caries, and opportunistic infections.8 A number of antineoplastic drugs cause xerostomia and the degree of xerostomia is related to the total number of chemotherapeutic agents used.4 The exact mechanisms by which these drugs damage salivary and other oral tissues are unknown. However, increased salivary drug concentration and prolonged contact of the drug-containing saliva with the oral epithelium is observed in patients with low flow rates. A high concentration of a biologically active drug may result in increased toxicity to oral tissues.8 Amifostine is also used to detoxify the reactive metabolites of cisplatin, a drug used to treat many cancers, including advanced ovarian, lung, and some head and neck cancers.4,8,17
Salivary Stimulation & Replacement Therapies
Salivary stimulation can be achieved mechanically by chewing sugarless gum and by chemical (gustatory) stimulation by sucking on sugarless candies or products that contain citric acid, such as vitamin C tablets, lemon drops, or lozenges.18 Caution must be used with citric acid due to its acidity. Sonic toothbrushing may also increase salivary flow in patients with SS.19
Artificial salivary substitutes can be recommended. They do provide short-term relief, however, compliance may be poor. Most products in this category contain sodium carboxymethylcellulose, which mimics the viscosity of natural saliva. Water-based moisturizing gels can be used intraorally as a saliva substitute and extraorally on the lips to provide 8 hours of relief from xerostomia symptoms.
Two prescription drugs have been approved by the Food and Drug Administration for the treatment of xerostomia: pilocarpine and cevimeline. These drugs are cholinergic agonists that produce parasympathetic stimulation of the exocrine glands to increase serous secretions. Pilocarpine is approved for use in both head and neck radiation therapy patients and patients with SS; cevimeline is approved for SS. Because these are systemic medications, they turn on secretions from all exocrine glands-an advantage for relieving multiple symptoms of SS. However, patients may experience adverse events related to their cholinergic effects, most notably excessive sweating. These drugs must be used with caution in patients with cardiovascular disease, chronic respiratory conditions, and kidney disease. Use of these medications is contraindicated in patients with narrow-angle glaucoma, uncontrolled asthma and liver disease. These are common disorders among the elderly who frequently present with xerostomia. Several clinical trials have demonstrated their efficacy in relieving xerostomia symptoms and increasing salivary flow in radiation therapy and SS patients.20
Current research is investigating the use of other medication classes that may relieve dry mouth symptoms, as well as biogenetic engineering technology to regenerate damaged tissues, and salivary transplantation.4,20 These discoveries will undoubtedly improve the oral health and quality of life of patients suffering from this chronic condition.
From Dimensions of Dental Hygiene. July 2005;3(7):22-24.
Associations between malnutrition, poor general health and oral dryness in hospitalized elderly patients.
Dormenval V, Budtz-Jørgensen E, Mojon P, Bruyère A, Rapin CH.
Department of Gerodontology and Removable Prosthodontics, University of Geneva, 19 rue Barthelemy-Menn, CH- 1205 Geneva, Switzerland.
OBJECTIVE: To obtain information about the possible relationship between symptoms and signs of oral dryness and malnutrition/poor general health in hospitalized older people. DESIGN: A cross-sectional clinical investigation with measurements of unstimulated salivary flow rates (USFR), stimulated salivary flow rates (SSFR), nutritional status, serum albumin concentration and an evaluation of symptoms of oral dryness and loss of appetite by a questionnaire. SUBJECTS AND METHODS: A cohort of 99 elderly, non-psychiatric patients hospitalized for medical reasons; collection of demographic and health data from medical files, collection of USFR and SSFR, measurements of body mass index (BMI), lean body mass, fat body mass, serum album in concentration; completion of a questionnaire related to symptoms of oral dryness and the patients' appreciation of their nutritional status. MAIN OUTCOME MEASURES: SSFR and USFR. RESULTS: Mean age of the 99 patients was 82.5 +/- 4.0 years. Anthropometric examinations indicated malnutrition of severe or intermediate degree in about 50% while 46% showed moderately and 40% severely reduced albumin. Loss of appetite was present in 54% and 51% complained of oral dryness; 17% had an USFR <0.1 ml/min and 26% a SSFR <0.5 ml/min. Significant associations were found between (i) reduced salivary flow rate, malnutrition and reduced serum albumin concentration, (ii) recent loss of appetite and low serum album in concentration and (iii)complaints of oral dryness and reduced salivary flow rates. There were also significant associations between complaints of oral dryness, loss of appetite and low BMI. CONCLUSION: Reduced salivary secretion and complaints of oral dryness could be signs of poor nutritional or general health status of elderly patients. Reduced salivary secretion and feeling of oral dryness could have a negative effect on alimentation, appetite and oral comfort.
PMID: 16296671 [PubMed - indexed for MEDLINE]
Impact of dry mouth on oral symptoms and function in removable denture wearers in Japan.
Ikebe K, Morii K, Kashiwagi J, Nokubi T, Ettinger RL.
Division of Oromaxillofacial Regeneration, Osaka University Graduate School of Dentistry, Suita, Japan. ikebe@dent.osaka-u.ac.jp
OBJECTIVE: The purpose of this study was to determine the association of dry mouth with oral symptoms and function, such as denture instability, discomfort, soreness in denture-bearing tissue, and dissatisfaction with chewing, tasting, or speaking in removable denture wearers. STUDY DESIGN: The subjects were 493 removable denture wearers with a mean age of 67.3 years. Perception of oral dryness was measured by a questionnaire. A multiple logistic regression analysis was used to determine the effect of the dry mouth on oral symptoms and function after controlling for age and gender. RESULTS: Oral dryness during eating was related to dissatisfaction with chewing (odds ratio, 10.5; P < .001) and speaking (odds ratio, 3.5; P < .05) and overall dissatisfaction (odds ratio, 6.3; P < .01) in complete denture wearers. Feeling of dry mouth was likely to be associated with soreness in denture-bearing tissues in both complete and removable partial denture wearers. CONCLUSIONS: There was a significant association of the perception of dry mouth among a group of denture wearers with oral symptoms and function.
#10
ANTICHOINERGICS: USES: This medication slows the activity of the stomach and intestinal tract, thus relieving cramping and reducing acid secretion. It is used in the treatment of peptic ulcers.
HOW TO USE: This medication is usually taken 30 to 60 minutes before meals and at bedtime. Take this medication exactly as prescribed. Do not increase the dose or take it more frequently without consulting your doctor. Drink plenty of fluids while using this medication unless your doctor directs you otherwise.
SIDE EFFECTS: This medication may cause flushing of the face, problems sleeping, headache, blurred vision, drowsiness, increased sensitivity to light, constipation, dry mouth, decreased sweating or thirst. If any of these symptoms persist or worsen, inform your doctor. Notify your doctor if you develop: confusion, tremors, rapid/irregular heartbeat, difficulty urinating. In the unlikely event you have an allergic reaction to this drug, seek immediate medical attention. Symptoms of an allergic reaction include: rash, itching, swelling, dizziness, trouble breathing. If you notice other effects not listed above, contact your doctor or pharmacist.
PRECAUTIONS: Tell your doctor your medical history, especially of: liver or kidney disease, high blood pressure, an overactive thyroid, nervous system disorders, all stomach/intestinal problems, glaucoma, enlarged prostate, allergies. Because this medication may cause drowsiness, use caution when driving or performing tasks requiring alertness. This medication can reduce sweating which can lead to heat stroke in hot weather. Use caution engaging in strenuous activity in hot weather. Contact lens wearers may need to use appropriate lubricating solutions if this medication causes dry eyes. Elderly patients may be more sensitive to the effects of this drug and should use this medication cautiously. Children may be more sensitive to the effects of this drug and should use this medication cautiously. Tell your doctor if you are pregnant before using this medication. It is not known if this drug is excreted into breast milk. Consult your doctor before breast-feeding.
Ship JA et al. Safety and efficacy of Xerostom containing olive oil, betaine, xylitol in the form of toothpaste, mouthrinse, mouth spray and gel for polypharmacy-induced xerostomia. 40 adults for 1 week led to a sig. unstimulated salivary flow rates.
By some estimates, as many as one-sixth of elderly Americans suffer from clinical depression. Elderly patients are more likely than younger ones to feel the stigma of depression, report fatigue and other somatic symptoms instead of psychological ones, and prefer treatment by their primary care physicians (PCPs). In fact, primary care prescribing of antidepressants for elderly patients increased markedly between 1985 and 1999, according to a study supported by the Agency for Healthcare Research and Quality (HS09566).
This was probably due to a combination of factors, says Stephen Crystal, Ph.D., of Rutgers University. These include: introduction of a new class of antidepressants in 1988—the selective serotonin reuptake inhibitors (SSRIs)—which have fewer side-effects than earlier antidepressants; increased recognition of depression by PCPs; and financial incentives leading to more reliance on antidepressants instead of more costly psychotherapy. Dr. Crystal and his colleagues used data from the National Ambulatory Medical Care Survey, a nationally representative annual survey of visits to physicians in office-based practices, to examine changes from 1985 to 1999 in diagnosis of depression and prescription of antidepressant medications during visits by elderly patients to PCPs, psychiatrists, and other specialists.
The majority of depression visits and visits where an antidepressant was prescribed were to PCPs in all time periods examined. Prescribing of antidepressants more than doubled between 1985 and 1998-1999 (from 2.4 percent of visits to 4.9 percent), with PCPs increasing their use of antidepressants from 3 percent to 6.3 percent of visits. Between 1993-1994 and 1997-1999, there was a significant increase in the rate at which SSRIs were prescribed during visits by elderly patients, with SSRIs accounting for over half (52 percent) of all antidepressants prescribed in 1997-1999.
More details are in "Trends in elderly patients' office visits for the treatment of depression according to physician specialty: 1985-1999," by Jeffrey S. Harman, Ph.D., Dr. Crystal, James Walkup, Ph.D., and Mark Olfson, M.D., M.P.H., in the July 2003 Journal of Behavioral Health Services & Research 30(3), pp. 332-341.
Daily use of the antidepressant medications known as selective serotonin reuptake inhibitors (SSRIs) by adults 50 years and older is associated with a doubled risk of some fractures, according to a report in the January 22, 2007 issue of Archives of Internal Medicine, one of the JAMA/Archives journals.
Depression affects about 10 percent of primary care patients in the United States, according to background information in the article. The use of SSRIs for the treatment of depressive symptoms is widespread due to the medication's presumed favorable adverse effect profile. Past studies have found the use of these antidepressants to be associated with an increased risk of clinical fragility fracture (fractures due to falling from bed, chair or standing height), but did not reliably examine such factors as falls and bone mineral density, the authors note.
J. Brent Richards, M.D., of McGill University, Montreal, Quebec, and colleagues evaluated 5,008 community-dwelling adults 50 years and older who were followed up for over five years for incident fractures. Researchers examined the relationships between SSRI use, bone mineral density (BMD) and falls. Participants who used the medication at the beginning of the study and at year five were considered to be recurrent users. BMD of the lower spine and hip were measured at the beginning of the study. Patients were then sent a yearly questionnaire to determine if they had experienced clinical fragility fractures and all reported fractures were confirmed radiographically. Other factors such as demographic information, history of falls and medication use were all assessed.
Daily use of SSRIs was reported by 137 participants with an average age of 65.1 years. The researchers found that "daily SSRI use remained associated with a two-fold increased risk of incident clinical fragility fracture even after adjustment for many potential confounding variables." These fractures occurred at the forearm (40 percent), ankle and foot (21 percent), hip (13 percent), rib (13 percent) femur (9 percent) and back (4 percent). Participants who used SSRIs at the beginning of the study had similar increased risks of fracture to those who used them at follow-up.
During the initial interview, the daily use of SSRIs was associated with an increased risk of falling. The effect was dose-dependent; doubling the daily dose of SSRIs increased the odds of falling 1.5-fold during the previous month. Daily use of SSRIs was also associated with a 4 percent decreased BMD at the total hip and a 2.4 percent decrease at the lumbar spine.
"Our results suggest that BMD and falls may be affected adversely by daily SSRI use but that fracture rates remain elevated despite adjustment for these two risk factors, indicating that other pathways, such as impaired bone quality leading to reduced bone strength, may be of particular relevance," the authors conclude. "In light of the high rate of SSRI use among the general population, and among elderly persons in particular, further studies that include controlled prospective trials are needed to confirm our findings."
----------------------------
Article adapted by Medical News Today from original press release.
Xerostomia is a subjective complaint associated with salivary gland hypofunction.1 However, the symptom of dry mouth can occur without an actual reduction in salivary flow. Etiologies of xerostomia include both salivary and nonsalivary causes.2 Identifying those with true salivary hypofunction is key due to the risk of oral disease. A thorough review of systems and medication history is essential to determining the origin of xerostomia symptoms.2
Medications
More than 500 drugs are reported to cause xerostomia as a side effect, and medication use is the most frequent cause of xerostomia complaints, especially among the elderly.3,4 The severity of the xerostomia complaint often increases among the elderly due to a synergistic effect when taking multiple medications.3,5 Both stimulated and unstimulated salivary flow rates decrease with an increasing number of medications taken.6 The most common cause of drug-induced xerostomia is the altering of neural pathways that stimulate salivary gland secretion.7 These are drugs that have either an anticholinergic or sympathomimetic effect.4 Stimulation of the parasympathetic nerves (cholinergic action) produces an increase in fluid volume (serous saliva). Stimulation by the sympathetic nerves (sympathomimetic action) produces less volume and viscous saliva.4,8 Thus, drugs that have an anticholinergic action reduce the volume of serous saliva, including antihypertensives, antihistamines, antidepressants, antipsychotics, antiemetics, antispasmotics, and anti-parkinsonian drugs.3,4,7 Drugs with sympathomimetic actions produce a more viscous, mucinous saliva with less volume, such as decongestants, bronchodilators, appetite suppressants, and amphetamines.4 Drugs may also exert their neural effects in the higher centers of the brain; stimulation of certain adrenoreceptors in the frontal cortex can produce inhibitory effects on salivary nuclei.3 Drugs can also produce xerostomia without affecting the neural pathways. Inhaled medications produce the sensation of dryness but without any change in salivary flow.3 Interestingly, some anti-hypertensive medications produce the symptoms of xerostomia without actually decreasing salivary flow.9 How antihypertensive medications actually cause xerostomia is unknown, although it is hypothesized that xerostomia may result from decreased fluid volume and loss of electrolytes secondary to increased urination and dehydration.9 Diuretics produce alterations in electrolyte and fluid balance.3,7 Finally, drugs can also decrease salivary flow by causing vasoconstriction in the salivary glands.3
The list of medications associated with xerostomia continues to grow as new drugs are released. Other drug classes now known to cause xerostomia include the proton pump inhibitors, protease inhibitors and reverse transcriptase inhibitors for HIV infection, analgesics and narcotics for pain control, a variety of anti-infective agents, and some anti-neoplastic agents.4,7 Table 1 lists the drug classes that cause xerostomia. Dental professionals can work with their patients' physicians to address chronic dryness. When possible, the patient may be taken off a medication or switched to another that is less xerogenic. The dosing regimen can be altered so that peak plasma levels of the drug do not correspond with periods of maximum dryness, such as nighttime. Dosages can be split into smaller quantities and ingested more frequently to allow for natural periods of salivary stimulation, eg, eating, to counteract the drying effects of the drugs.3
Diseases of the Salivary Glands
Sjögren's syndrome (SS) is an autoimmune disorder characterized by intense lymphocytic infiltration of the exocrine glands. This infiltration destroys much of the glandular structure, making it difficult to produce fluids for normal function. Common symptoms include chronic dry eyes and dry mouth. There are two forms of the disease: primary SS not associated with any other autoimmune disease and secondary SS associated with other connective tissue diseases, including rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.4 International diagnostic criteria are published to assist with the diagnosis of the disease, which among others include measures of salivary gland inflammation, and the presence of specific autoantibodies in the serum.10 Biopsy of the labial minor salivary glands demonstrates a characteristic focal lymphocytic infiltration.11 Glandular swelling is characteristic of SS. However, persistent swelling of the parotid glands also may indicate bacterial infection or lymphoma.12 Lymphocytic invasion, causing local salivary tissue inflammation and fibrosis, combined with the autoimmune-mediated interference with neurotransmitter and receptor function appear to be responsible for the clinical manifestations of SS.12 Interestingly, labial salivary gland biopsies taken from patients with severe oral and ocular dryness reveal that as many as 50% of their glandular cells remain intact.13 This allows patients with SS to benefit from salivary stimulating medications.
Chronic salivary gland enlargement and xerostomia are also symptoms of sarcoidosis, HIV disease, and hepatitis C viral infection (HCV).4 HIV salivary gland disease occurs in up to 8% of infected individuals and most frequently affects the parotid glands with bilateral enlargement and xerostomia. It usually arises late in the course of HIV infection but occasionally may be the first manifestation of HIV disease. Kaposi's sarcoma and nonHodgkin's lymphoma associated with HIV infection may also cause salivary gland enlargement.4 Medications used to treat HIV disease also produce xerostomia.4 HCV salivary gland disease affects up to 33% of affected persons, with xerostomia as the predominant symptom.4 Histologically, the salivary gland changes with this disease resemble those seen with SS but with a lesser degree of inflammation. Other diseases that are associated with xerostomia include amyloidosis, cystic fibrosis, autoimmune thyroiditis, rheumatoid arthritis, chronic graft-versus-host disease, and diabetes.4,13-16 Medication use, elevated glycosylated hemoglobin levels, and elevated fasting blood glucose levels are identified as factors leading to dehydration and xerostomia in Type I diabetics.16
Table 1. Drug classes associated with causing xerostomia. Anorexiants
Antiacne Agents
Antianxiety Agents
Anticholinergics/Antispasmotics
Anticonvulsants
Antidepressants
Antidiarrheals
Antiemetics
Antihistamines
Antihypertensives
Anti-inflammatory Analgesics
Antinauseants
Antiparkinsonian Agents
Antipsychotics
Bronchodilators
Decongestants
Diuretics
Muscle Relaxants
Narcotic Analgesics
SedativesSource: USP DI® Drug Information for the Healthcare Professional. 24th ed. Englewood, Colo: Micromedix, Inc; 2004. Cancer Therapies
Salivary glandular tissues are highly sensitive to the radiation therapy used to treat oral carcinomas, and serous acinar cells found in the parotids are more radiosensitive than the mucous cell types.4,8 Serous cells may contain more heavy metals that absorb radiation energy, which promotes the release and action of free radicals.8 Amifostine is a chemoprotective drug used to reduce the incidence of moderate to severe xerostomia in patients undergoing radiation therapy that includes a significant portion of the parotid glands. The drug acts as a scavenger of free radicals found in the tissues.17
#11 Affects 1% of population or 2 million individuals. Onset of symptoms typically at middle age. Dry mouth lasting longer than 3 months, dental caries and parotid gland swelling is often the presentation Second most common symptom was dry eyes. .Fungal infections also were common. Reported reduced quality of life. More than 50% use parasympathomimetics-pilocarpine, cevimeline but widespread use of complementary techniques.
ChrExperts estimate that 75 percent of all autoimmune-disease cases occur in women. Researchers can't pinpoint a reason, but many believe hormones play a role. Some autoimmune illnesses occur more frequently following puberty or menopause. Others improve during pregnancy and flare up again after delivery, while still others worsen during pregnancy. "Autoimmune diseases seem to hit women particularly in their most demanding years -- when they are starting their families and have young children at home," Rose says. onic lymphocytic infiltration of salivary and lacrimal glands. Second most common autoimmune disease next to rheumatoid arthritis. Over 1 million people suffer from this syndrome. During the 5-year interval between examinations, a history of dry eye developed in 322 of 2414 subjects, for an incidence of 13.3% (95% confidence interval [CI], 12.0%-14.7%). Incidence was significantly associated with age (P<.001). After adjusting for age, incidence was greater in subjects with a history of allergy or diabetes, who used antihistamines or diuretics, and with poorer self-rated health (P<.05). Age-adjusted incidence was less in subjects using angiotensin-converting enzyme inhibitors or consuming alcohol (P<.05). It was not significantly associated with sex, blood pressure, hypertension, serum total or high-density lipoprotein cholesterol level, body mass index, history of arthritis, gout, osteoporosis, cardiovascular disease, thyroid disease, or smoking, and use of caffeine, vitamins, antianxiety medications, antidepressants, calcium channel blockers, or anticholesterolemics.
Autoimmune disorders are diseases caused by the body producing an inappropriate immune response against its own tissues. Sometimes the immune system will cease to recognize one or more of the body’s normal constituents as “self” and will create autoantibodies – antibodies that attack its own cells, tissues, and/or organs. This causes inflammation and damage and it leads to autoimmune disorders.
The cause of autoimmune diseases is unknown, but it appears that there is an inherited predisposition to develop autoimmune disease in many cases. In a few types of autoimmune disease (such as rheumatic fever), a bacteria or virus triggers an immune response, and the antibodies or T-cells attack normal cells because they have some part of their structure that resembles a part of the structure of the infecting microorganism.
Autoimmune disorders fall into two general types: those that damage many organs (systemic autoimmune diseases) and those where only a single organ or tissue is directly damaged by the autoimmune process (localized). However, the distinctions become blurred as the effect of localized autoimmune disorders frequently extends beyond the targeted tissues, indirectly affecting other body organs and systems. Some of the most common types of autoimmune disorders include:
Systemic Autoimmune Diseases
Localized Autoimmune Diseases
Rheumatoid arthritis (RA) and Juvenile RA (JRA) (joints; less commonly lung, skin)Type 1 Diabetes Mellitus (pancreas islets)Lupus [Systemic Lupus Erythematosus] (skin, joints, kidneys, heart, brain, red blood cells, other)Hashimoto's thyroiditis, Graves' disease (thyroid)Scleroderma (skin, intestine, less commonly lung)Celiac disease, Crohn's disease, Ulcerative colitis (GI tract)Sjogren's syndrome (salivary glands, tear glands, joints)Multiple sclerosis*Goodpasture's syndrome (lungs, kidneys)Addison's disease (adrenal)Wegener's granulomatosis (blood vessels, sinuses, lungs, kidneys)Primary biliary cirrhosis, Sclerosing cholangitis, Autoimmune hepatitis (liver)Polymyalgia Rheumatica (large muscle groups)Temporal Arteritis / Giant Cell Arteritis (arteries of the head and neck)Guillain-Barre syndrome (nervous system)
#12 30 mg 3x a day cevimeline parasympathomimetic adverse interactions with uncontrolled
Asthma and narrow angle glaucoma.
Pilocarpine or Salagen tablets 5mg 4x a day.
Ship evaluated the safety and efficacy of a group of a topical dry mouth products (Xerostom), containing olive oil, betaine, and xylitol. Were developed to reduce xerostomia. The results were significantly greater increase in unstimulated salivary flow rates in the form of toothpaste, gel, spray and mouth rinse.
Gustatory and masticatory stimuli as sugar free candies. Pilocarpine and Cevimiline are 2 cholinergic agonist drugs. Pilocarpine 5mg 4x day. Contraindicated for patients with narrow angle glaucoma,iritis and uncontrolled asthma. Cevimeline has alonger half life and may less side effects with more gradual action. Mouthkote and Oral balance gel often keep tissues moist for longer period of time. Biotene product available.
#14 The philosophic patient is a positive person often with a zest for life like Mae. They are usually in good health, well balanced type of person and have success with past denture service or have no experience and do not anticipate any special difficulties. They have realistic goals and they realize there is a partnership between their dentist and themselves in attaining success. They beieve their dentist is equipt to perform a satisfactory denture serviceand appreciates his intent, expertise and caring personality. If there is a problem during the adjustment phase, they are patient and non-blaming. They do not expect immediate results.
#15 The exacting or critical patient will find fault with everything that is done for them. They were never happy with their previous dentists, and this is because the dentist never quite followed THEIR instruction. They will bring with them a collection of dentures made by different dentists and will tell the new dentist what was wrong and sometimes with diagrams that have draftsman-like rendering. Careful observation will reveal that the mistakes had been made as a result of trying to follow the directions of these patients often at the expense of prosthodontic principles. A FIRM CONTROL OF THESE PATIENTS IS CRITICAL. They actually do well with a firm hand and boundaries.
#16 They have had bad results with previous treatment and are doubtful that anyone can treat them. They have a sense that there problems are insurmountable. Often they have had a series of personal tragedies such as business problems, loss of spouse and other disappointments not related to their denture problem. They think the world is against them and they are often angry. A careful and thorough exam can be the start of successful treatment. The dentist should take extra time than usual since care and attention to detail will help to develop confidencein the new dentist. One may choose to recommend counseling or NOT to treat the patient.
#17 Indifferent-They have little appreciation for the efforts of their dentists and have little concern for their teeth, oral health or appearance. They often seek treatment at the insistence of their family. They will give up easily if problems are encountered in the treatment. More time is needed in the instruction of the value and care of dentures.
#19 J Prosthet Dent. 2003 Mar;89(3):297-302. Links
The House classification pertains to a patient in isolation. How does the observer affect the observed??? The patient’s behavior is codetermined by the personality and behavior of the dentist. The dentist may play a role as a parent who demands submission or one who wishes to be pleased or a cooperative relationship.
Landesman and Friedman spoke of the alliance that is critical in successful complete denture therapy and peer review has demonstrated the number 1 reason for disgruntled patients is poor communication. :Lastly technically sound dentures do not guarantee satisfied patients and dentures lacking in well executed principles of construction may be well accepted by patients.
M. M. House mental classification revisited: Intersection of particular patient types and particular dentist's needs.
Gamer S, Tuch R, Garcia LT.
School of Dentistry, Department of Restorative Dentistry, University of Southern California, Los Angeles, USA. sgamerdds@aol.com
Fifty-three years ago, M. M. House devised a classification of patients on the basis of how they behaved in response to the prospect of becoming edentulous and on how they subsequently adapted to wearing complete dentures. Although House's system was an important contribution, it failed to consider the dentist's emotional reaction to a patient's behavior as part of an understanding of how the patient and doctor cope with the dental treatment. This article presents an expansion of the House classification to include the behavior of the dentist as a codeterminer of the patient's behavior. This expanded classification system is based on empiricism and awaits scientific validation or clinical application to determine its ultimate validity, reliability, and effectiveness.
#27 The cuspid eminence is the highest point along the border of the maxillary denture and it is necessary to reproduce this eminence on the labial surface even if the patient has significant resorption here.
Optical harmonies with many dissimilar forms are best accomplished by using curves because curves are much harder to discern than a straight line.
Velature technique was noted by nuclear accelerator technique- no palate , the colors built color by color on canvass.
To make a tooth appear smaller make it darker. This will allow a posterior tooth to recede appropriately into the arch.
#28 (formerly called insulin-dependent diabetes or juvenile diabetes) occurs when the person's own immune system attacks and destroys the cells of the pancreas that produce insulin. Children with type 1 diabetes need insulin to help keep their blood sugar levels within a normal range.
Type 2 diabetes (formerly called non-insulin-dependent diabetes) is different. In contrast to someone with type 1 diabetes, someone with type 2 diabetes still produces insulin. But the body doesn't respond to the insulin normally. Glucose is less able to enter the cells and do its job of supplying energy (doctors call this insulin resistance). This causes the blood sugar level to rise, making the pancreas produce even more insulin. Eventually, the pancreas can wear out from working overtime to produce extra insulin. Then, the pancreas may no longer be able to produce enough insulin to keep a person's blood sugar levels within a normal range.
Oral manifestations of diabetes mellitus in complete denture wearers.
Cristina de Lima D, Nakata GC, Balducci I, Almeida JD.
STATEMENT OF PROBLEM: The oral mucosa has been reported to show a variety of changes in subjects with diabetes mellitus. PURPOSE: The purpose of this study was to compare diabetic and nondiabetic subjects wearing complete dentures with regard to salivary flow, salivary buffering capacity, denture retention, and oral mucosal lesions. MATERIAL AND METHODS: Sixty subjects, 30 with and 30 without a diagnosis of diabetes, were matched for gender, race, and age. Salivary flow, salivary buffering capacity, glycemia, blood pressure, presence of mucosal lesions, denture retention, use of medications, and behavioral factors (controlled or uncontrolled diet, alcohol consumption, and smoking) reported by the subjects, were evaluated. For the salivary buffering capacity test, 1 mL of saliva was pipetted into a test tube containing 3 mL 0.005 N of hydrochloric acid, and the pH was measured with indicator strips. Group differences were statistically analyzed using the Student t test and the Mann-Whitney test for quantitative variables and the chi-square test for qualitative variables (alpha =.05). RESULTS: Mean (SD) salivary flow was 1.14 (0.87) mL/min in the nondiabetic subjects and 0.95 (0.61) mL/min in the diabetic subjects. Evaluation of self-reported denture retention revealed no significant difference between groups. Denture retention was observed in 66.7% (20/30) of the control group and in 50% (15/30) of the diabetic group. The prevalence of mucosal lesions was 90% (27/30) in the control group and 83.3% (25/30) in the diabetic group. Salivary buffering capacity was 5.80 (0.85) in the control group and 5.26 (0.83) in the diabetic group (P=.017). CONCLUSIONS: Within the limitations of this study, no significant differences were observed in salivary flow, denture retention, or oral lesions in diabetic and nondiabetic subjects.
Salivary flow, denture retention, oral lesions are no different in diabetic and non-diabetic patients, despite the susceptibility of to erosion and ulceration of mucosa where it comes into contact with denture. The prevalence of diabetes continues to increase steadily as more people live longer and grow heavier. The overall prevalence of diagnosed cases of type 2 diabetes rises from 1.4 percent between the ages 25 of 44 years to 3.6 percent between the ages of 45 and 54 years, 7.8 percent between the ages of 55 and 64 years, and over 10 percent over the age of 65 years [1]. The prevalence may be well over 20 percent among frail elderly people living in nursing homes [2]. There are probably similar numbers of undiagnosed patients at all ages.
The prevalence of known cases of type 2 diabetes is likely to increase further with the adoption of new diagnostic criteria and the recommendation to screen all adults over age 45 years at least once every three years by measuring fasting blood glucose [3]. (See "Diagnosis of diabetes mellitus" and see "Screening for diabetes mellitus").
Older adults with diabetes are at risk of developing macrovascular and microvascular complications similar to their younger counterparts with diabetes and as a result, suffer excess morbidity and mortality compared with elderly individuals without diabetes [4]. In addition, they are at higher risk for polypharmacy, functional disabilities and common geriatric syndromes that include cognitive impairment, depression, urinary incontinence, falls and persistent pain [5]. This topic will review diabetes management in elderly patients and how management priorities and treatment choices may differ between elderly and younger patients.
INDIVIDUALIZING MANAGEMENT — Older adults with diabetes are a heterogeneous population that includes persons residing independently in communities, in assisted care facilities or nursing homes. Thus older adults with diabetes can be fit and healthy or frail with many co-morbidities and functional disabilities.
Type 2” diabetes is the most common form of diabetes (90-95% of diabetes patients). It is also referred to as non-insulin dependent diabetes and presents as high blood glucose levels despite an initial abundance of the hormone insulin. The cells of the body ignore the insulin and do not allow glucose to enter the body's cells. This insulin resistance leads to high levels of glucose in the bloodstream, and eventually to beta-cell failure, where the beta-cells of the pancreas are no longer able to release insulin in response to high blood glucose levels. Type 2 diabetes usually appears in those over 40, and is treated by diet alone, or by diet and oral medications.
#29 Henry Collett JPD 1961;11:608-16. Development of Maladjustment Attitudes: When the patient was a child he/she may have been rejected and as a survival mechanism has developed attention-seeking devices which become deeply embedded in the personality and is likely to use them throughout his life. The patient obtains a certain amount of attention from the dentist by seeking unnecessary adjustments. Overprotection by parents can also lead to maladjustments. This results in a lack of confidence and the patient seeks constant reassurance that the denture will be serviceable and will not cause harm. When these demands of reassurance are not met, the patient can become adversarial.
When
#35 The patient is now involved in the fabrication of the new dentures which adds another increment of relationship building. If after a considerable amount of treatment, it becomes apparent that the patient’s adaptive ability is not increasing sufficiently, it would be in her best interest and the doctor’s to address the issue. Most patients reject the initial suggestion, but with a strong relationship, an initial rejection may change to acceptance.
#36 There is a small percentage of patients who can not adapt because they need their symptoms. Patients maintain symptoms for a variety of reasons. The symptoms may represent a way of rationalizing other problems, manipulating people, and may be an exhibitionist attempt to draw sympathy from other people. These symptoms may be absolutely necessary to maintain a precarious psychological equilibrium. If the patient cannot relinquish such symptoms, the dentist will fail.
A study by Eitner et al tested to see if there were intraoral/sensorimotor causes in patients with psychologic diagnosis of psychogenic prosthesis incompatibility. No correlation between functional/anatomic aspects of stereognostic ability and the clinical picture of psychogenic prosthesis incompatibility.
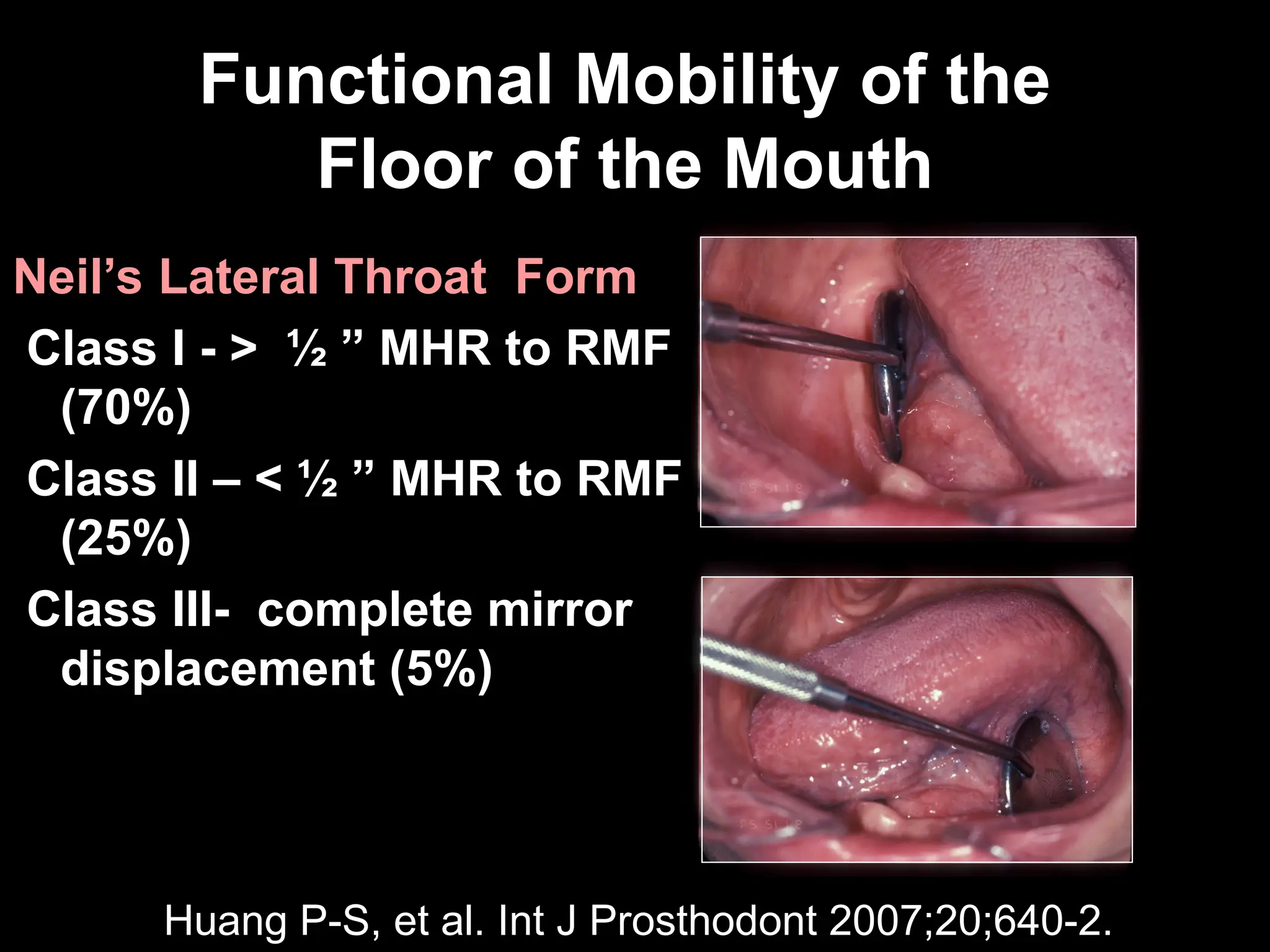
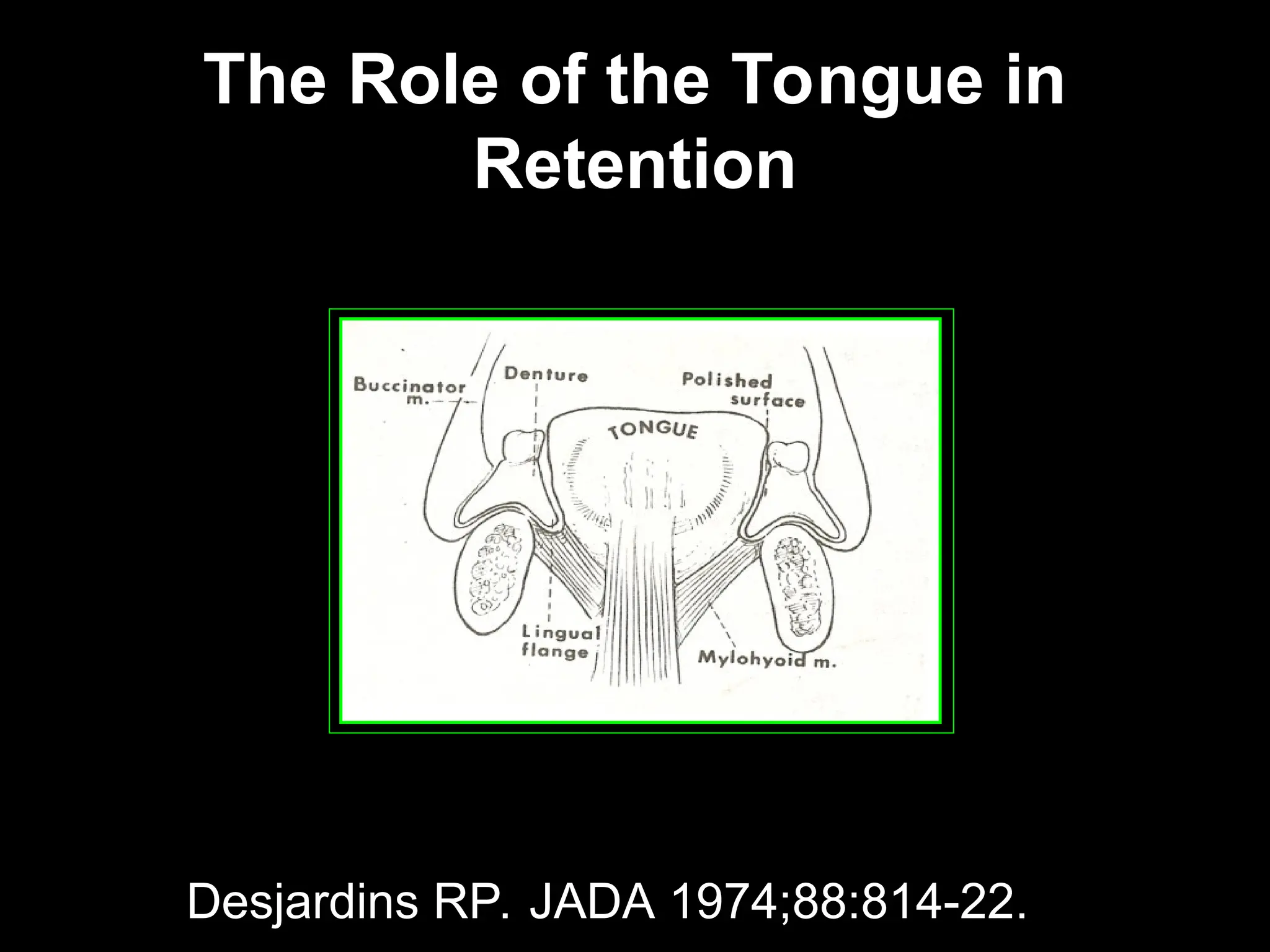
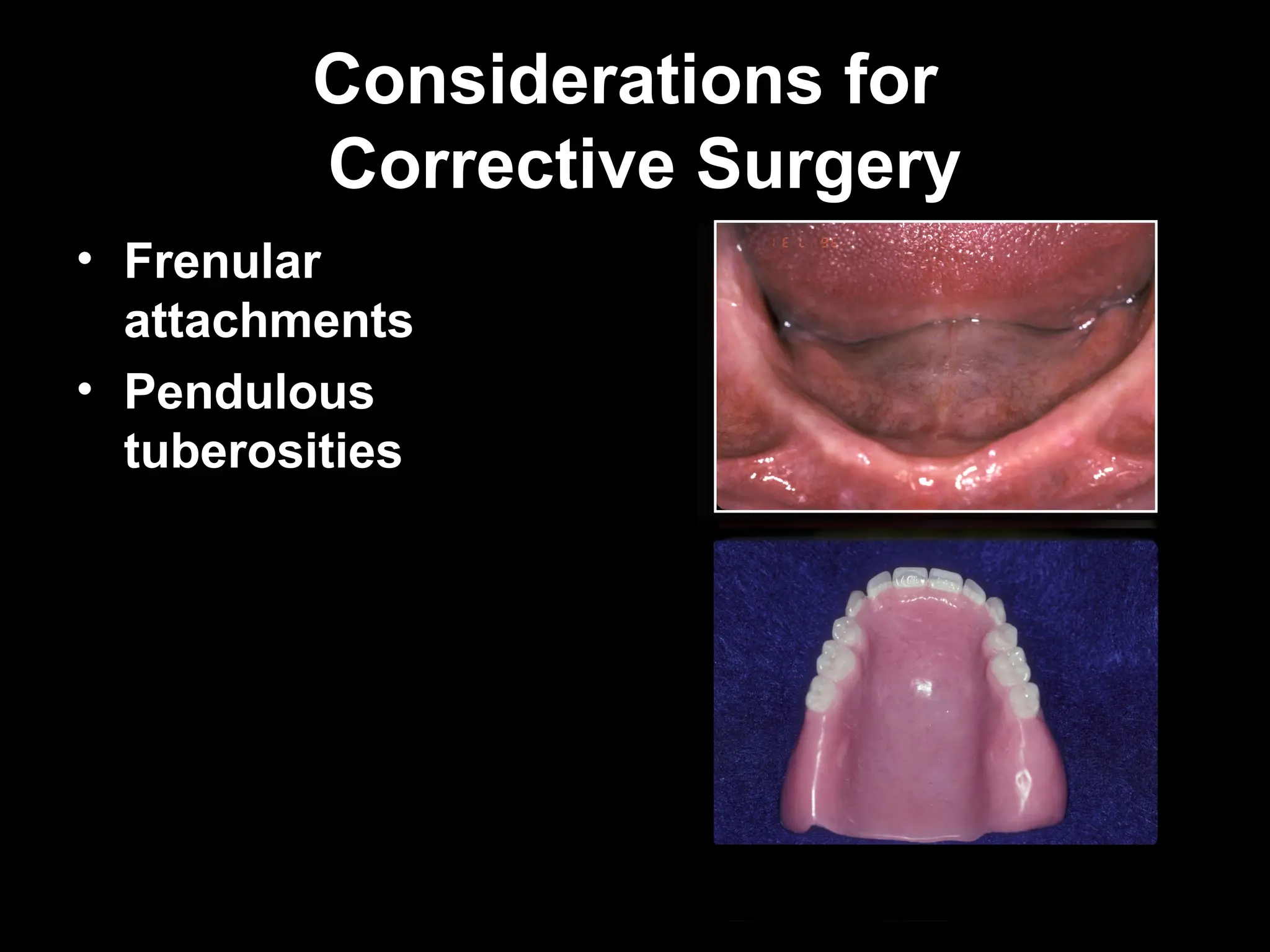
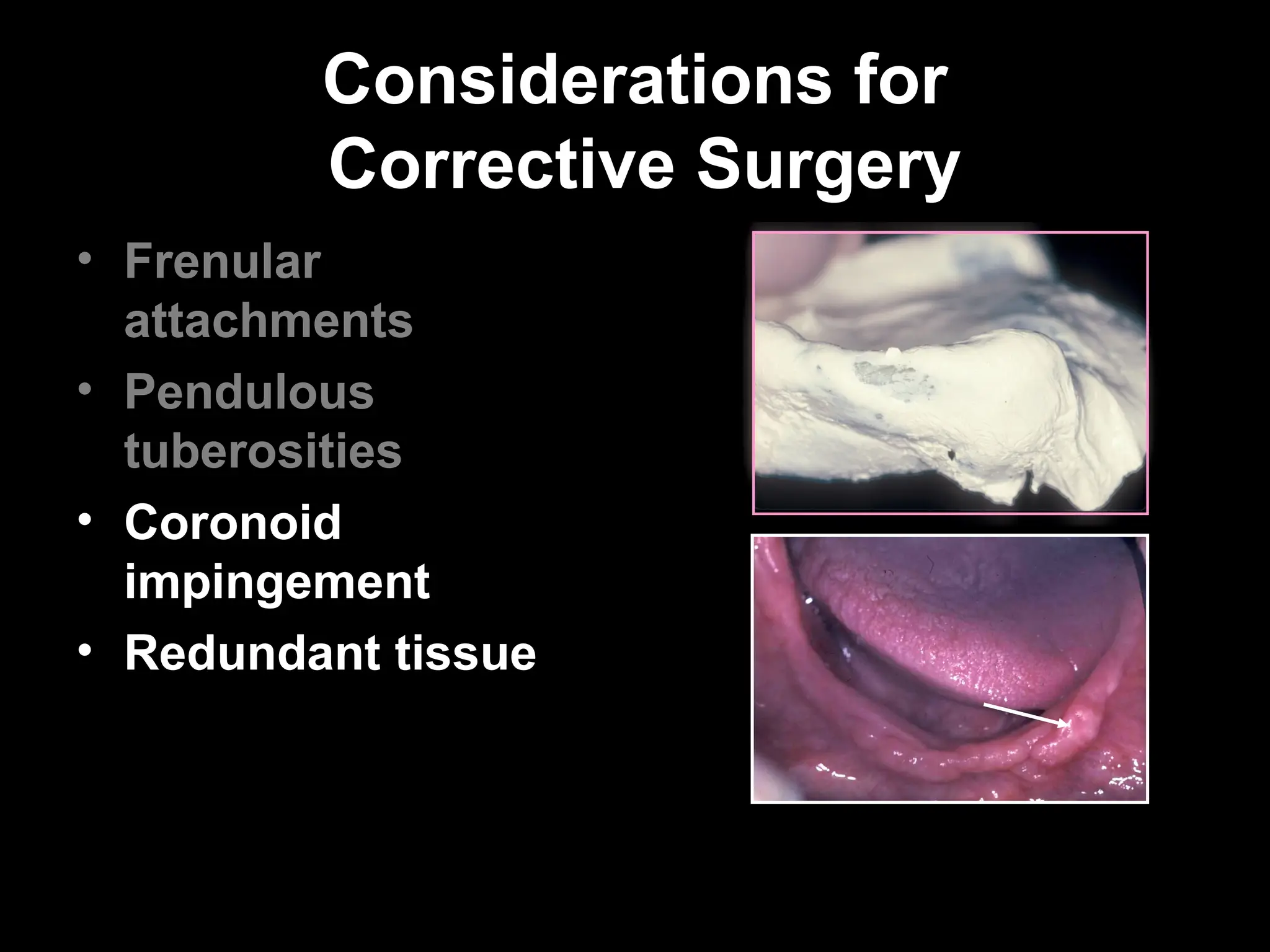
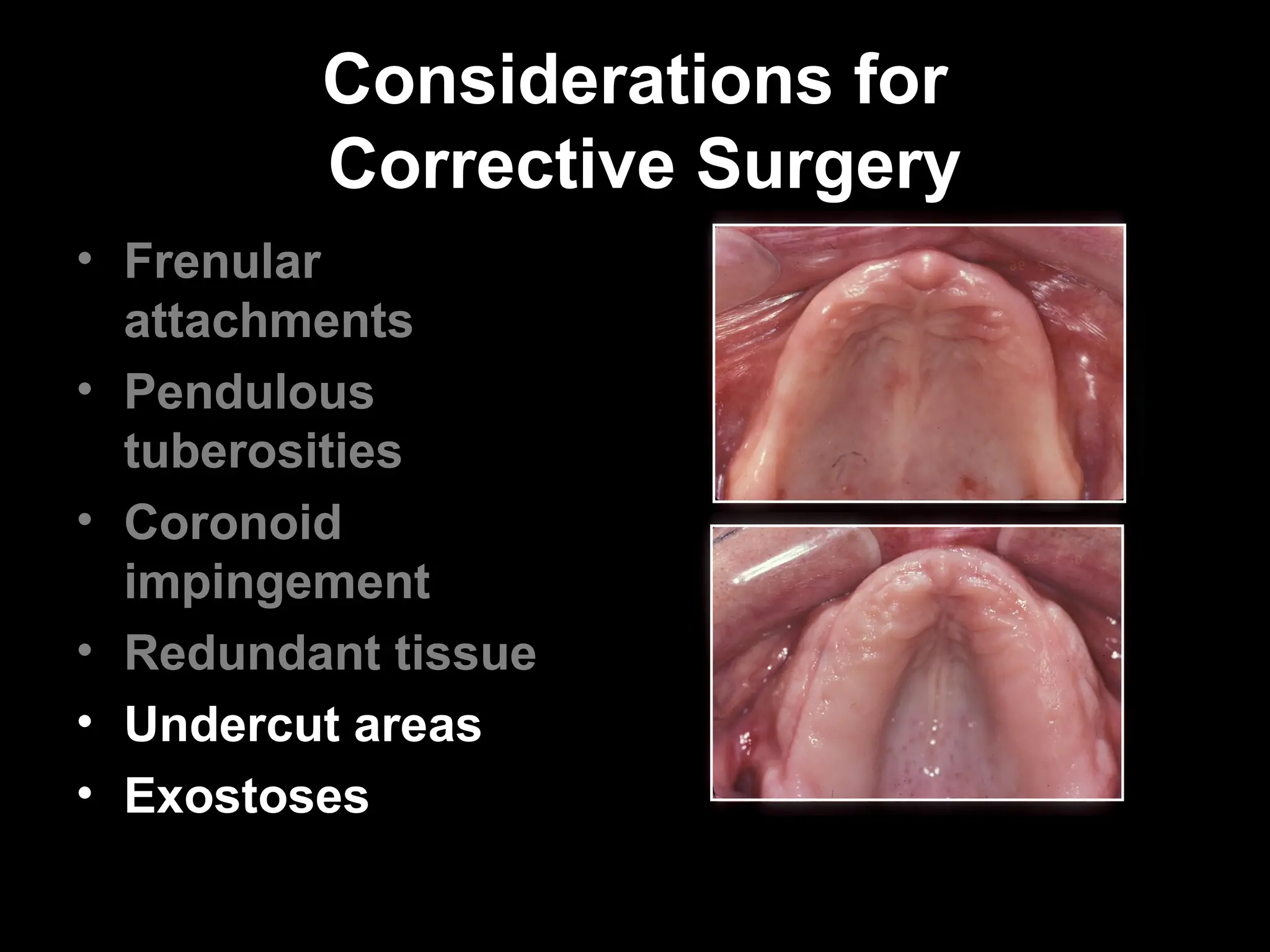
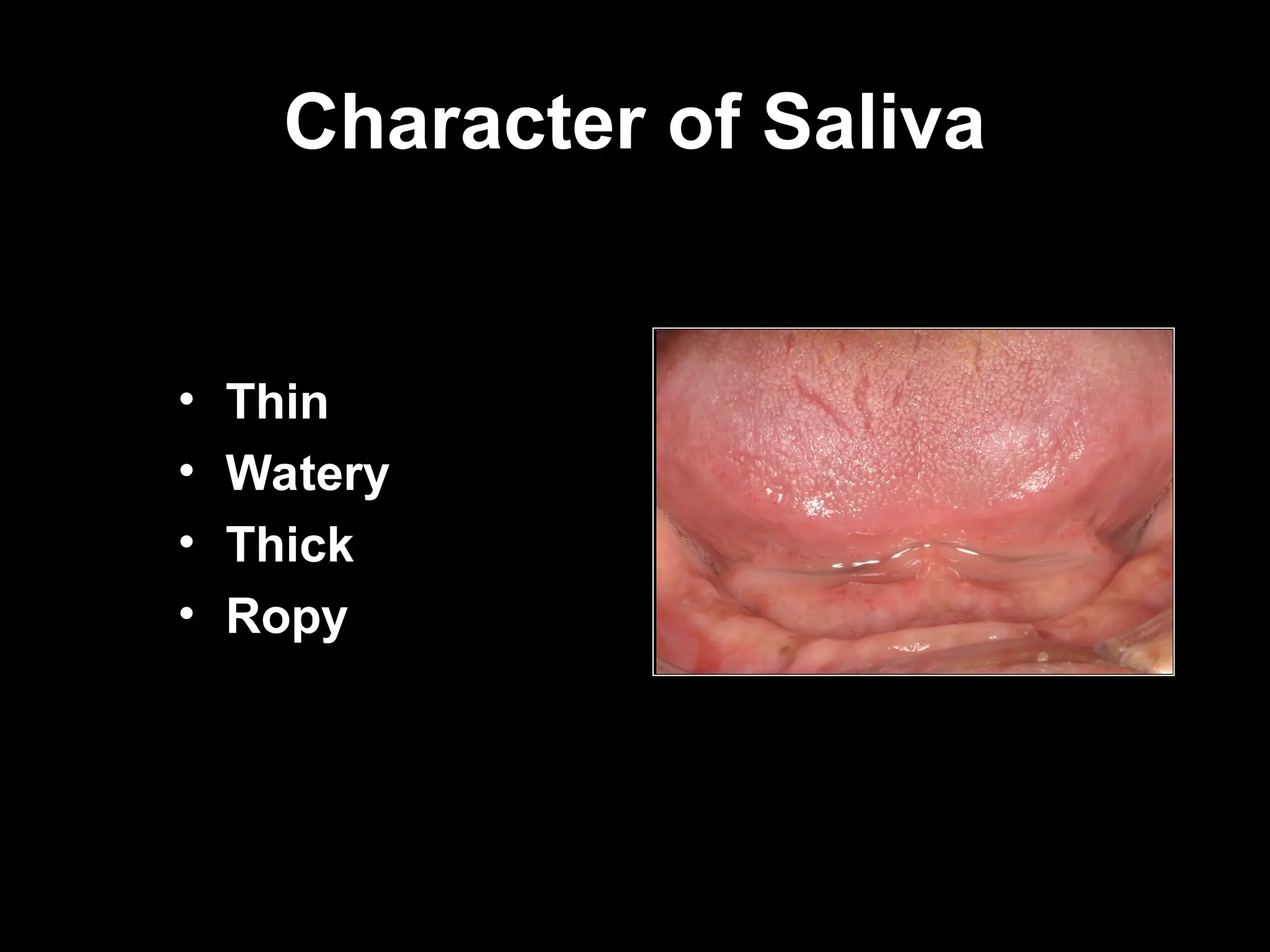
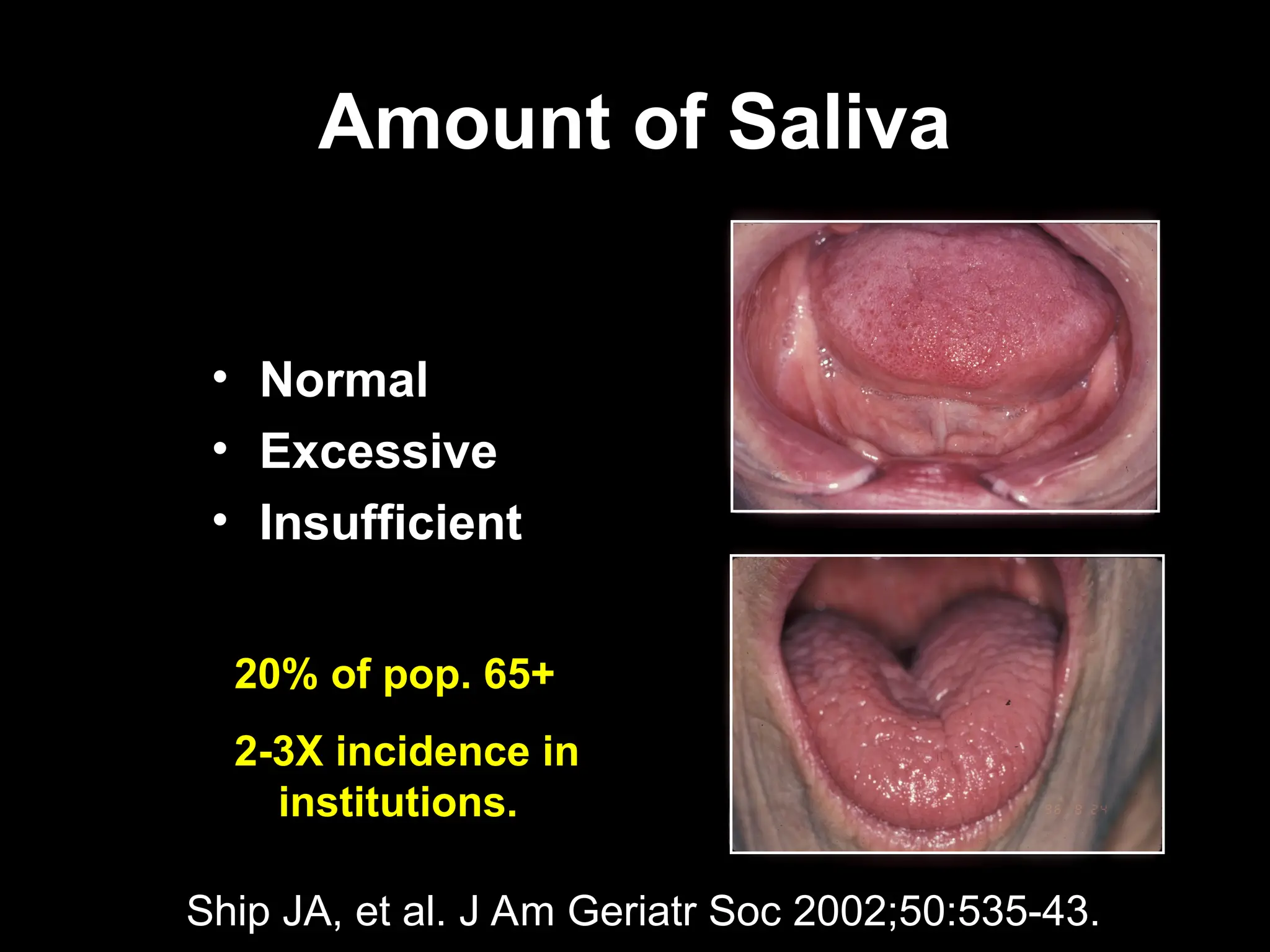



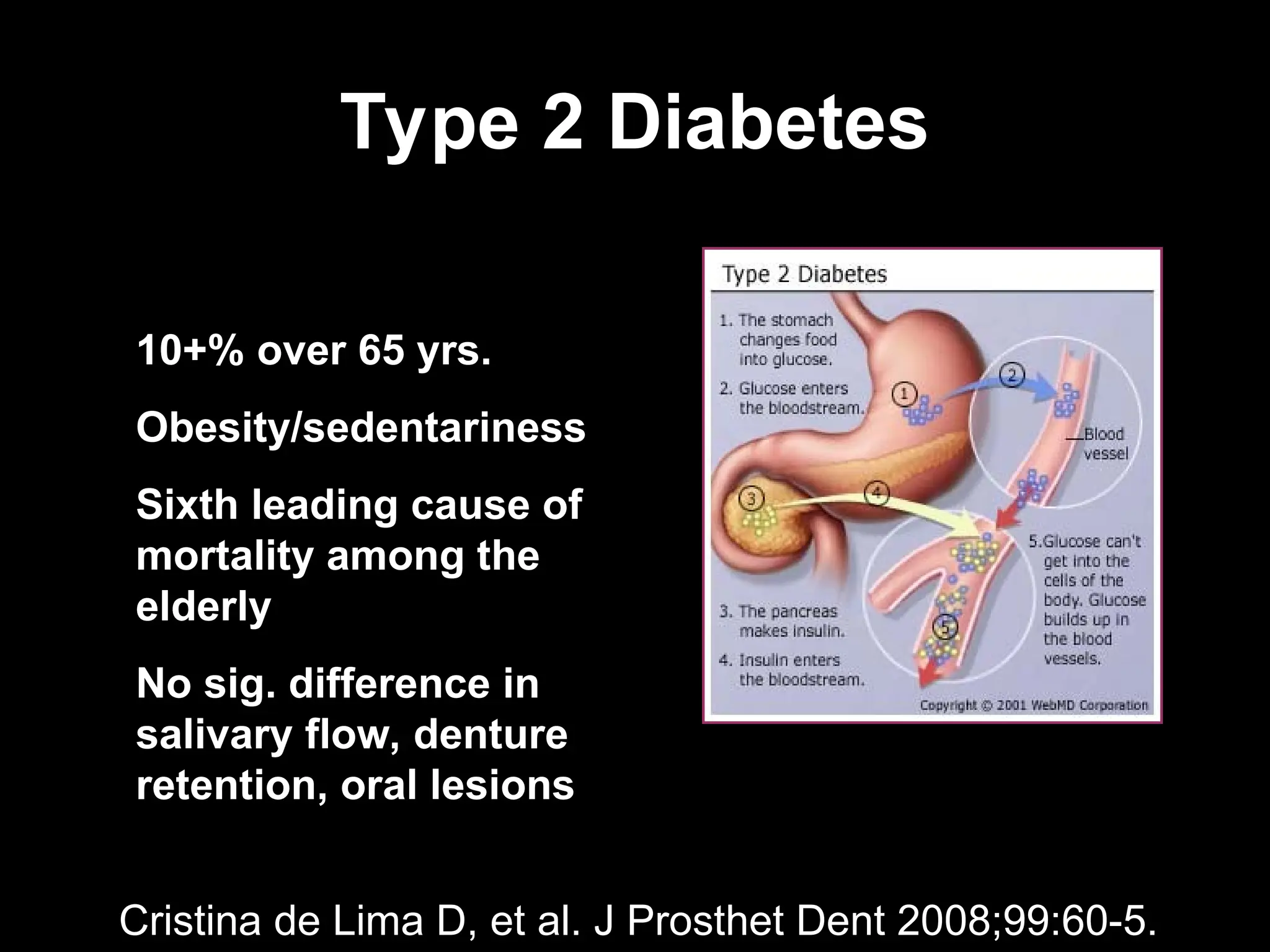
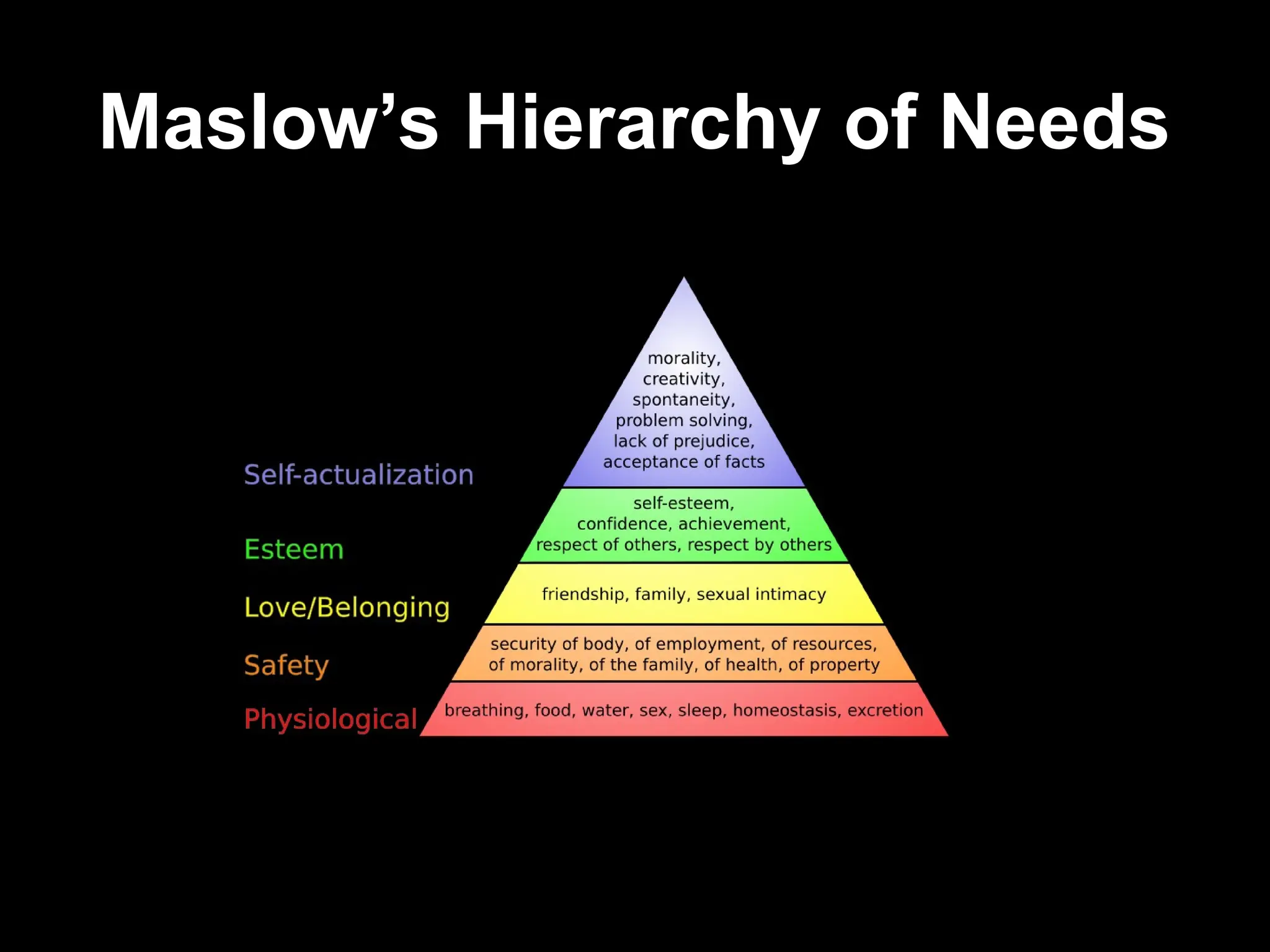










![HISTORY TAKING IN COMPLETELY EDENTULOUS PATIENTS [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/historytakingincompletelyedentulouspatientsautosavedautosaved-250408092503-84de7c34-thumbnail.jpg?width=640&height=640&fit=bounds)




































