Stromal of themarrow:
• Stromal cells
• Fat cells
• Blood vessels
• Fibroblasts
• Endothelial cells
• Iron deposits
• Osteoblast and osteoclasts.
4.
Normal Erythropiesis:
Proerythroblast: 12-20microns, nucleus with stippled chromatin and 1-
2 nucleoli and have basophilic cytoplasm.
Early erythroblast: 12-16 microns, nuclear chromatin condenses,
nucleoli are lost and there is light basophilic cytoplasm.
Intermediate erythroblast: 10-12 microns, nucleus is condensed,
reddish tinge in the cytoplasm.
Late erythroblast: Nucleus is densely pyknotic with well hemoglobinized
reddish cytoplasm
6.
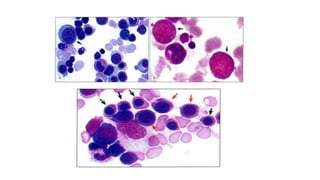
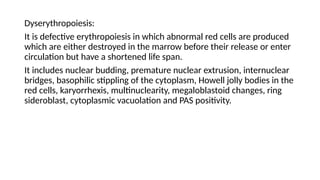
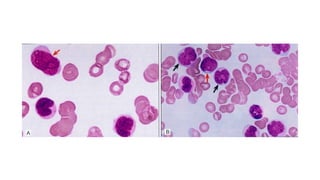
Dyserythropoiesis:
It is defectiveerythropoiesis in which abnormal red cells are produced
which are either destroyed in the marrow before their release or enter
circulation but have a shortened life span.
It includes nuclear budding, premature nuclear extrusion, internuclear
bridges, basophilic stippling of the cytoplasm, Howell jolly bodies in the
red cells, karyorrhexis, multinuclearity, megaloblastoid changes, ring
sideroblast, cytoplasmic vacuolation and PAS positivity.
8.
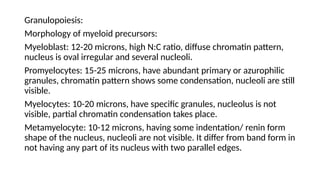
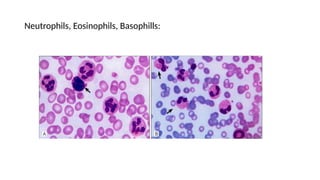
Granulopoiesis:
Morphology of myeloidprecursors:
Myeloblast: 12-20 microns, high N:C ratio, diffuse chromatin pattern,
nucleus is oval irregular and several nucleoli.
Promyelocytes: 15-25 microns, have abundant primary or azurophilic
granules, chromatin pattern shows some condensation, nucleoli are still
visible.
Myelocytes: 10-20 microns, have specific granules, nucleolus is not
visible, partial chromatin condensation takes place.
Metamyelocyte: 10-12 microns, having some indentation/ renin form
shape of the nucleus, nucleoli are not visible. It differ from band form in
not having any part of its nucleus with two parallel edges.
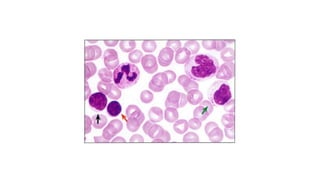
Lymphopoiesis:
Lymphoblast: 12-20 microns,centrally placed nucleus with 1-2 nucleoli,
chromatin is coarser than that of myeloblast, thin rim of pale blue
cytoplasm.
Large lymphocyte: 10-15 microns, central/eccentric nucleus, clear pale
blue cytoplasm, no nucleoli, nuclear chromatin is less condensed as
compared to that of small lymphocytes.
Small lymphocyte: 7-9 microns, slightly larger than mature RBCs, nuclear
chromatin is densely coarse with thin rim of pale blue cytoplasm.
Large granular lymphocyte: These are large lymphocytes with abundant
cytoplasm containing few azurophilic granules. These are NK cell or
cytotoxic T cells.
14.
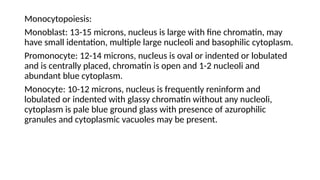
Monocytopoiesis:
Monoblast: 13-15 microns,nucleus is large with fine chromatin, may
have small identation, multiple large nucleoli and basophilic cytoplasm.
Promonocyte: 12-14 microns, nucleus is oval or indented or lobulated
and is centrally placed, chromatin is open and 1-2 nucleoli and
abundant blue cytoplasm.
Monocyte: 10-12 microns, nucleus is frequently reninform and
lobulated or indented with glassy chromatin without any nucleoli,
cytoplasm is pale blue ground glass with presence of azurophilic
granules and cytoplasmic vacuoles may be present.
16.
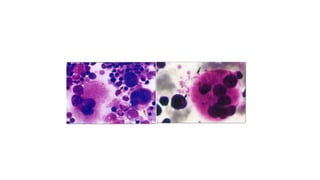
Thrombopoiesis:
Megakaryoblast: 10-15 microns,blue nongranular cytoplasm and single
irregular nucleus with many nucleoli.
Promegakaryocyte: 15-25 microns, lower N:C ratio with dark blue
cytoplasm and a dense nonlobulated or partly lobulated nucleus with
heavy chromatin.
Intermediate form: Intermediate form of megakaryocytes is larger than
promegakaryocyte. Lobulation of nucleus has begun and cytoplasm
contains some azurophilic granules.
Mature megakaryocyte: 25-120 microns, single large multilobed
nucleus with increased density as its matures. The cytoplasm varies in
colour from blue to pink and contains a variable number of
characteristics azurophilic granules at first in the perinuclear zone.
18.
INDICATION OF BONEMARROW ASPIRATION
• Unexplained cytopenia
• Unexplained polycythemia, leucocytosis, thrombocytosis
• Evaluation of iron stores for diagnosis of IDA or to distinguish it from
anemia of chronic disease, demonstration of ringed sideroblasts in
myelodysplastic syndrome or sideroblastic anemia.
• Suspected acute leukemia
• Suspected myelodysplastic syndrome
• Suspected myeloproliferative disorder
• Suspected plasma cell dyscrasia
19.
• Suspected chroniclymphoid leukemias
• Investigation of pyrexia of unknown origin
• Suspected storage disorder like Gaucher’s disease or Neimann disease
• Suspected infection like kala-azar, miliary tuberculosis or
histoplasmosis
• For ancillary investigation like flow cytometry, cytogenetics or
molecular analysis
• To monitor response to therapy and to assess remission or relapse
20.
INDICATIONS OF BONEMARROW BIOPSY
• Repeated failure of aspiration (Dry tap)
• Suspected aplastic anemia
• Suspected myelofibrosis
• Suspected focal lesions like granuloma, metastatic deposit, or
infiltrate of lymphoma
• Suspected bone disorder e.g osteoporosis
• Staging of lymphoma
Bone marrow aspirationprovides following information:
• Assessment of morphology of bone marrow cells.
• Assessment of nature of hematopoiesis (normal, dyshematopoiesis).
• Cytogenetic analysis.
• Immunophenotyping of abnormal cells in leukemias.
• Cytochemistry for typing of leukemia.
• Iron stains for assessing iron stores and sideroblasts.
• Microbial culture e.g for tuberculosis.
24.
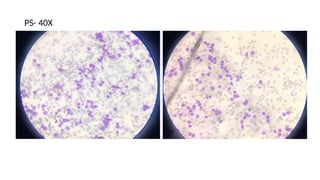
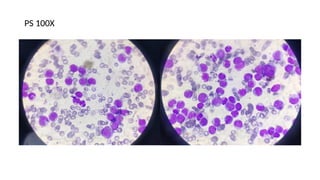
Bone marrow aspirationsmears
Peripheral blood smear in conjunction with routine hemogram should
be examine first before assessing bone marrow smears and finding
should be interpreted in the light of clinical feature and relevant
laboratory data and detailed clinical history with features like pallor,
liver and spleen size, lymphadenopathy, history of drug intake, bone
pain, bleeding etc.
25.
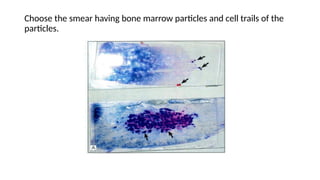
Choose the smearhaving bone marrow particles and cell trails of the
particles.
26.
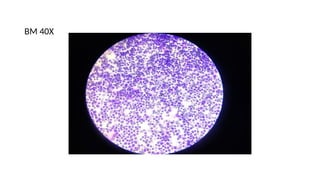
Romanowsky- stained smearsare first examined under low power objective
(x10) to assess:
• Cellularity of marrow particles.
• Number of megakaryocytes
• Focal metastatic deposits
• Cell distribution and selection of suitable area for detailed cytologic
examination.
Megakaryocytes are found in the tail of the smear or near the marrow
particles. About 1-3 megakaryocytes are seen normally per low power field.
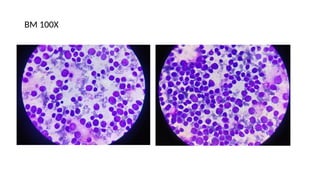
Cellular trails are examined under high power (x 40) and oil immersion
objective (x100) for differential count and assessing erythroid and myeloid
maturation. For differential count, at least 500 cells should be counted in
cellular trails of particles.
27.
Examination of marrowsmear consists of assessment of following
features:
• Cellularity
• Differential count
• Myeloid : Erythroid ratio
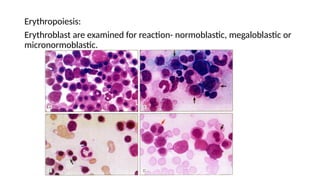
• Erythroid series: Maturation sequence, type of maturation
( normoblastic, micronormoblastic, megaloblastic), cytologic
abnormalities.
• Myeloid series: Maturation sequence, cytologic abnormalities.
• Megakaryocyte series: Number, abnormal forms.
• Lymphocyte series
28.
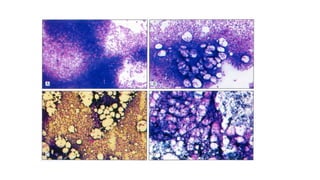
• Plasma cellseries
• Abnormal cells: Blasts, carcinoma cells and necrotic cells
• Parasites: Malaria parasites, microfilaria, Leishmania donovani, and
Histoplasma
• Iron content of marrow (on iron stain).
29.
CELLULARITY:
Assessment of cellularityis based on examination of several marrow
particles. Cellularity refers to the proportion of hematopoietic cells as
compared to the fat cells in a marrow particle. Cellularity can also be
assessed by examining the density of hematopoietic cells in cellular
trails behind the marrow particles. Cellularity can be expressed either
in percentage or stating whether marrow particles are normocellular,
hypercellular, or hypocellular for age.
Infant marrow- 95-100% cellular
Children- 75-80%
Adult- 50-60%
Old age- 20-40%
M:E Ratio:
It isthe ratio of all granulocytes and their precursors to all erythroid
precursor cells.
• Increased M:E ratio is observed when myeloid series is hyperplastic as
in infection and myeloproliferative disorders (chronic or acute
myeloid leukemia) or when erythroid series is suppressed as in
aplastic crisis of hemolytic anemia.
• Reduced M:E ratio is observed when myeloid series is depressed and
in erythroid hyperplasia (e.g hemolytic anemia).
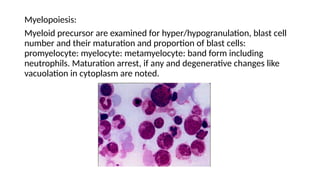
Myelopoiesis:
Myeloid precursor areexamined for hyper/hypogranulation, blast cell
number and their maturation and proportion of blast cells:
promyelocyte: myelocyte: metamyelocyte: band form including
neutrophils. Maturation arrest, if any and degenerative changes like
vacuolation in cytoplasm are noted.
35.
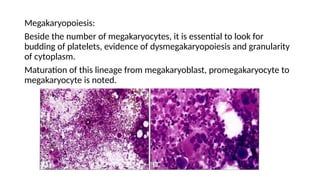
Megakaryopoiesis:
Beside the numberof megakaryocytes, it is essential to look for
budding of platelets, evidence of dysmegakaryopoiesis and granularity
of cytoplasm.
Maturation of this lineage from megakaryoblast, promegakaryocyte to
megakaryocyte is noted.
36.
Lymphocytes and plasmacells:
• Lymphocytes in adult are <10%
• Lymphocytes in children vary between 10-40%
• Plasma cells in adult are <4%
Marrow should be examined for other hematopoietic cells-
macrophages, mast cells, osteoblasts and osteoclasts.
37.
Case Presentation
42 yearold male, came to OPD with complain of-
Generalized bodyache and weakness since 1week, Intermittent fever
since 3 days, fatigue and weight loss since 15 days.
On examination-
Right axillary lymphadenopathy 2x2cm, Right inguinal
lymphadenopathy 3x2cm.
Hepatomegaly (2cm below costal margin).
Splenomegaly, mediastinal mass- not palpable.
6 year oldmale, came to OPD with complain of-
Fever, cough cold on and off since 1 ½ month, generalized weakness
and decrease appetite since 1month, increase paleness all over the
body since 1 month, breathing difficulty and abdominal pain since
3days, swelling over right parotid region since 2days.
H/O one unit blood transfusion.
On examination-
Pallor +++, icterus +
Hepatomegaly, Splenomegaly








































![Hemangiblastoma CNS PPT.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hemangiblastomacnsppt-251005155615-644fd7bd-thumbnail.jpg?width=640&height=640&fit=bounds)






























