INDICATIONS
• Diagnose adisease
• Monitor response
• Detect pre-analytical or analytical error in output of automated
analyzer
• Correlate instrument flag
3.
• Macroscopic examination
1.Assess whether the spreading technique was satisfactory
2. Judge its staining characteristics
3. Presence of any abnormal particles-
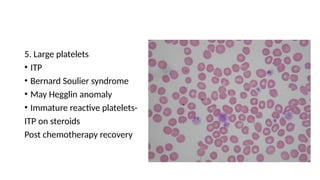
Large platelet aggregates
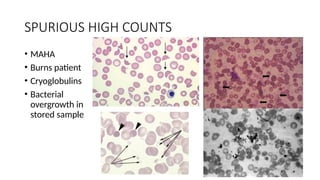
Cryoglobulin deposits
• Clumps of tumour cells
5.
• Well preparedand well stained smear
• Tongue shaped smear
• No irregularities
• No serrations at tail end
• No air bubbles
6.
• Low power10 x:
1)Quality of film and staining
2) Location and selection of proper field
3)Approx. no. of RBCs
4)Microfilaria like parasites
7.
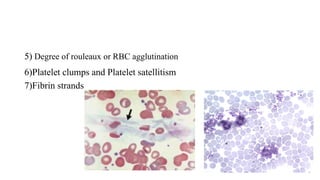
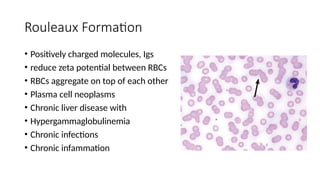
5) Degree ofrouleaux or RBC agglutination
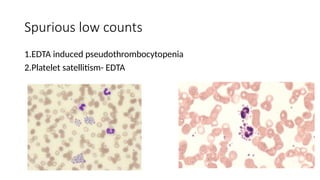
6)Platelet clumps and Platelet satellitism
7)Fibrin strands
8.
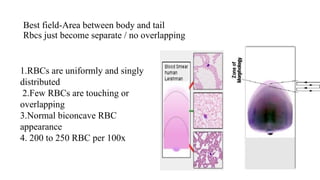
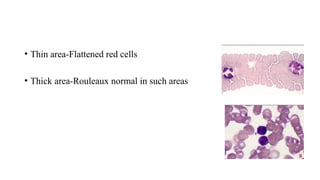
Best field-Area betweenbody and tail
Rbcs just become separate / no overlapping
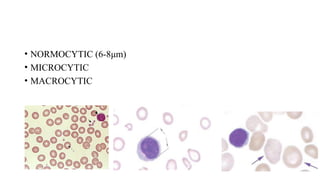
1.RBCs are uniformly and singly
distributed
2.Few RBCs are touching or
overlapping
3.Normal biconcave RBC
appearance
4. 200 to 250 RBC per 100x
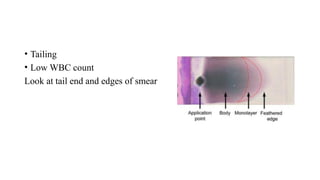
• Tailing
• LowWBC count
Look at tail end and edges of smear
11.
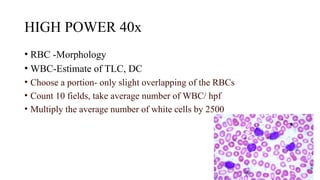
HIGH POWER 40x
•RBC -Morphology
• WBC-Estimate of TLC, DC
• Choose a portion- only slight overlapping of the RBCs
• Count 10 fields, take average number of WBC/ hpf
• Multiply the average number of white cells by 2500
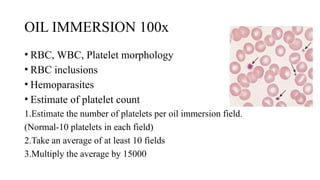
OIL IMMERSION 100x
•RBC, WBC, Platelet morphology
• RBC inclusions
• Hemoparasites
• Estimate of platelet count
1.Estimate the number of platelets per oil immersion field.
(Normal-10 platelets in each field)
2.Take an average of at least 10 fields
3.Multiply the average by 15000
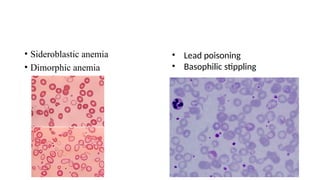
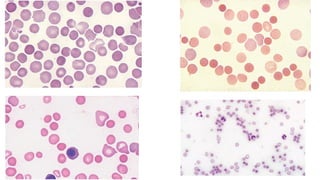
DIMORPHIC ANEMIA
• Twodifferent population of RBC
–Macrocytes + normocytes
–Microcytes with normocytes
–Macrocytes with microcytes
•MCV –low, normal or high
23.
Causes of Dimorphicanemia
• Response to iron or vitamin therapy
• Blood transfusion in a pt. with microcytic/macrocytic anemia
• Myelodysplastic syndromes
• Sideroblastic anemias
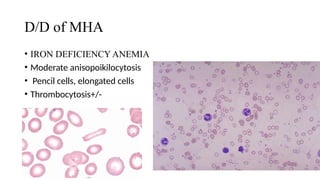
• Well-made films
•<10% are definitely oval shaped
• Percentage of ‘pyknocytes’ (irregularly contracted cells) and
schistocytes :
• Adults does not exceed 0.1%
• Full-term infants - Higher-0.3–1.9%
• Premature infants still higher- up to 5.6%
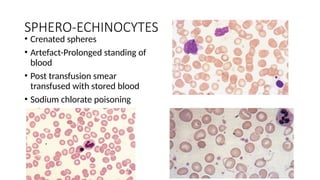
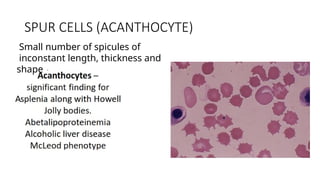
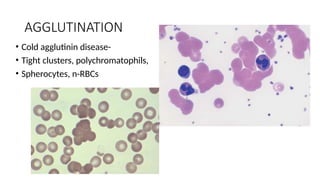
SPHERO-ECHINOCYTES
• Crenated spheres
•Artefact-Prolonged standing of
blood
• Post transfusion smear
transfused with stored blood
• Sodium chlorate poisoning
31.
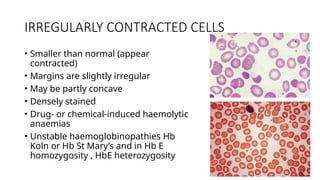
IRREGULARLY CONTRACTED CELLS
•Smaller than normal (appear
contracted)
• Margins are slightly irregular
• May be partly concave
• Densely stained
• Drug- or chemical-induced haemolytic
anaemias
• Unstable haemoglobinopathies Hb
Koln or Hb St Mary’s and in Hb E
homozygosity , HbE heterozygosity
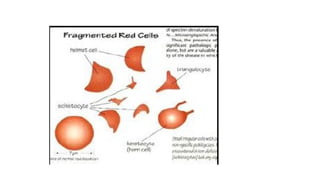
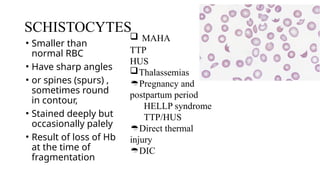
SCHISTOCYTES
• Smaller than
normalRBC
• Have sharp angles
• or spines (spurs) ,
sometimes round
in contour,
• Stained deeply but
occasionally palely
• Result of loss of Hb
at the time of
fragmentation
TTP
HUS
Thalassemias
Pregnancy and
postpartum period
HELLP syndrome
TTP/HUS
Direct thermal
injury
DIC
MAHA
38.
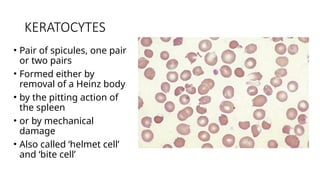
KERATOCYTES
• Pair ofspicules, one pair
or two pairs
• Formed either by
removal of a Heinz body
• by the pitting action of
the spleen
• or by mechanical
damage
• Also called ‘helmet cell’
and ‘bite cell’
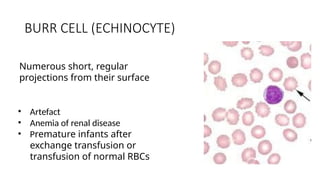
BURR CELL (ECHINOCYTE)
•Artefact
• Anemia of renal disease
• Premature infants after
exchange transfusion or
transfusion of normal RBCs
Numerous short, regular
projections from their surface
41.
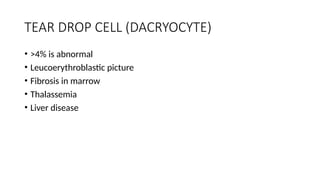
TEAR DROP CELL(DACRYOCYTE)
• >4% is abnormal
• Leucoerythroblastic picture
• Fibrosis in marrow
• Thalassemia
• Liver disease
42.
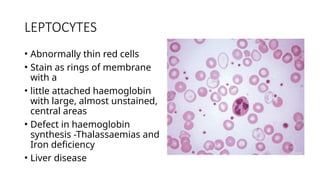
LEPTOCYTES
• Abnormally thinred cells
• Stain as rings of membrane
with a
• little attached haemoglobin
with large, almost unstained,
central areas
• Defect in haemoglobin
synthesis -Thalassaemias and
Iron deficiency
• Liver disease
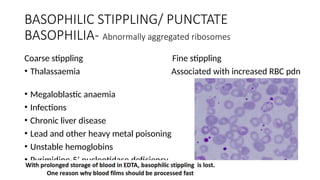
BASOPHILIC STIPPLING/ PUNCTATE
BASOPHILIA-Abnormally aggregated ribosomes
Coarse stippling Fine stippling
• Thalassaemia Associated with increased RBC pdn
• Megaloblastic anaemia
• Infections
• Chronic liver disease
• Lead and other heavy metal poisoning
• Unstable hemoglobins
• Pyrimidine-5’ nucleotidase deficiency
45.
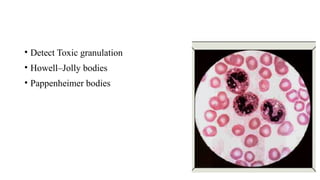
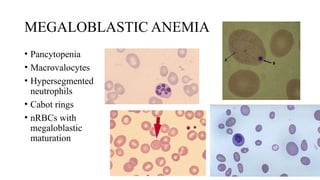
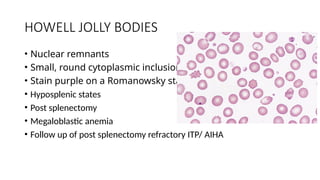
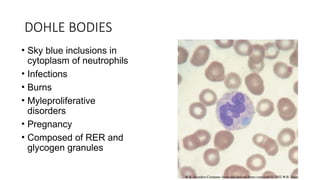
HOWELL JOLLY BODIES
•Nuclear remnants
• Small, round cytoplasmic inclusions
• Stain purple on a Romanowsky stain
• Hyposplenic states
• Post splenectomy
• Megaloblastic anemia
• Follow up of post splenectomy refractory ITP/ AIHA
46.
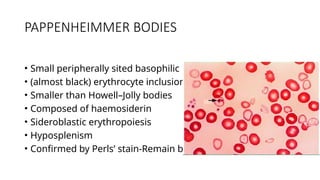
PAPPENHEIMMER BODIES
• Smallperipherally sited basophilic
• (almost black) erythrocyte inclusions
• Smaller than Howell–Jolly bodies
• Composed of haemosiderin
• Sideroblastic erythropoiesis
• Hyposplenism
• Confirmed by Perls’ stain-Remain blue
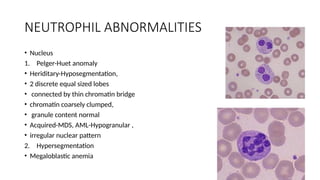
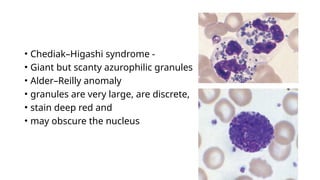
• Chediak–Higashi syndrome-
• Giant but scanty azurophilic granules
• Alder–Reilly anomaly
• granules are very large, are discrete,
• stain deep red and
• may obscure the nucleus
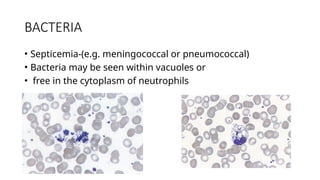
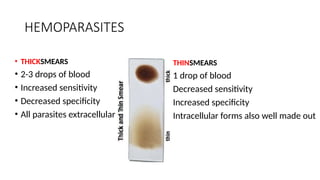
HEMOPARASITES
• THICKSMEARS
• 2-3drops of blood
• Increased sensitivity
• Decreased specificity
• All parasites extracellular
• THINSMEARS
• 1 drop of blood
• Decreased sensitivity
• Increased specificity
• Intracellular forms also well made out
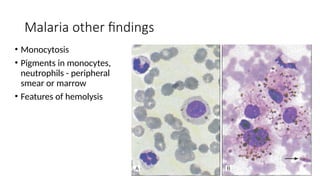
Malaria other findings
•Monocytosis
• Pigments in monocytes,
neutrophils - peripheral
smear or marrow
• Features of hemolysis
71.
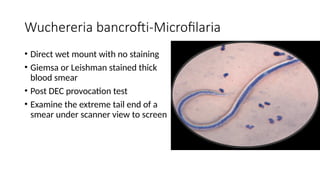
Wuchereria bancrofti-Microfilaria
• Directwet mount with no staining
• Giemsa or Leishman stained thick
blood smear
• Post DEC provocation test
• Examine the extreme tail end of a
smear under scanner view to screen
72.
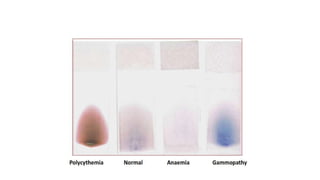
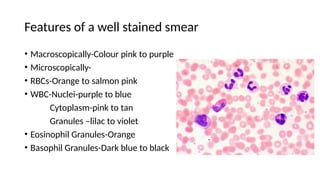
Features of awell stained smear
• Macroscopically-Colour pink to purple
• Microscopically-
• RBCs-Orange to salmon pink
• WBC-Nuclei-purple to blue
Cytoplasm-pink to tan
Granules –lilac to violet
• Eosinophil Granules-Orange
• Basophil Granules-Dark blue to black
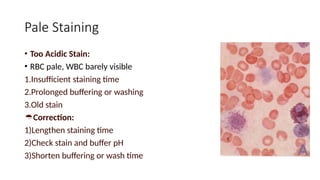
Pale Staining
• TooAcidic Stain:
• RBC pale, WBC barely visible
1.Insufficient staining time
2.Prolonged buffering or washing
3.Old stain
Correction:
1)Lengthen staining time
2)Check stain and buffer pH
3)Shorten buffering or wash time
75.
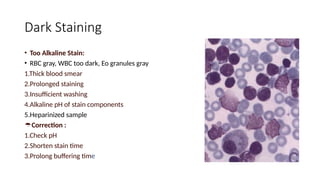
Dark Staining
• TooAlkaline Stain:
• RBC gray, WBC too dark, Eo granules gray
1.Thick blood smear
2.Prolonged staining
3.Insufficient washing
4.Alkaline pH of stain components
5.Heparinized sample
Correction :
1.Check pH
2.Shorten stain time
3.Prolong buffering time
76.
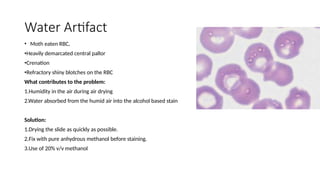
Water Artifact
• Motheaten RBC,
•Heavily demarcated central pallor
•Crenation
•Refractory shiny blotches on the RBC
What contributes to the problem:
1.Humidity in the air during air drying
2.Water absorbed from the humid air into the alcohol based stain
Solution:
1.Drying the slide as quickly as possible.
2.Fix with pure anhydrous methanol before staining.
3.Use of 20% v/v methanol
77.
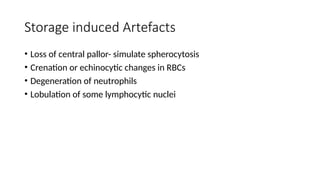
Storage induced Artefacts
•Loss of central pallor- simulate spherocytosis
• Crenation or echinocytic changes in RBCs
• Degeneration of neutrophils
• Lobulation of some lymphocytic nuclei